Diabetes Mellitus Is an Independent Predictor of Short-Term Mortality in Critically Ill ICU Patients
Mădălina Diana Daina (Fehér), Codrin Dan Nicolae Ilea, Cosmin Mihai Vesa, Alina Cristiana Venter, Adriana Vladu, Timea Claudia Ghitea, László Fehér, Cristian Marius Daina

TL;DR
Diabetes increases short-term death risk in ICU patients, even after adjusting for other factors, suggesting it should be considered in early risk assessments.
Contribution
This study identifies diabetes mellitus as an independent predictor of ICU mortality, contributing to improved risk stratification strategies.
Findings
Diabetes mellitus was present in 32.4% of ICU patients and linked to higher mortality.
Diabetes remained an independent predictor of ICU death after adjusting for confounders like age and sepsis.
Abstract
What are the main findings? Diabetes mellitus was present in nearly one-third of critically ill ICU patients and was associated with significantly higher short-term mortality.After adjustment for major clinical confounders, diabetes mellitus remained an independent predictor of ICU mortality. Diabetes mellitus was present in nearly one-third of critically ill ICU patients and was associated with significantly higher short-term mortality. After adjustment for major clinical confounders, diabetes mellitus remained an independent predictor of ICU mortality. What are the implications of the main findings? Diabetes status should be considered an important prognostic factor during early ICU risk assessment.Critically ill patients with diabetes may benefit from closer monitoring and individualized management strategies in intensive care settings. Diabetes status should be considered an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
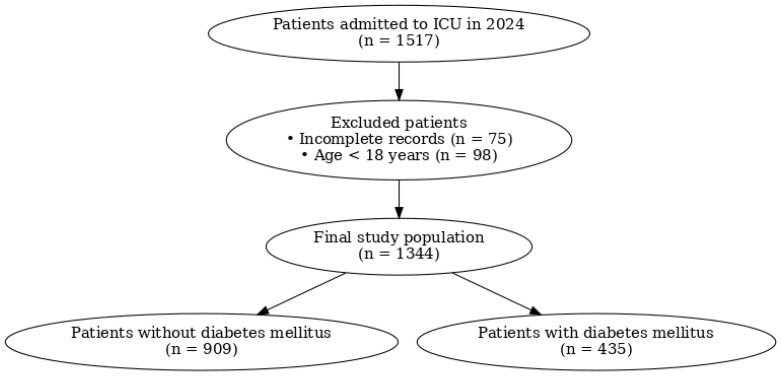 Figure 1
Figure 1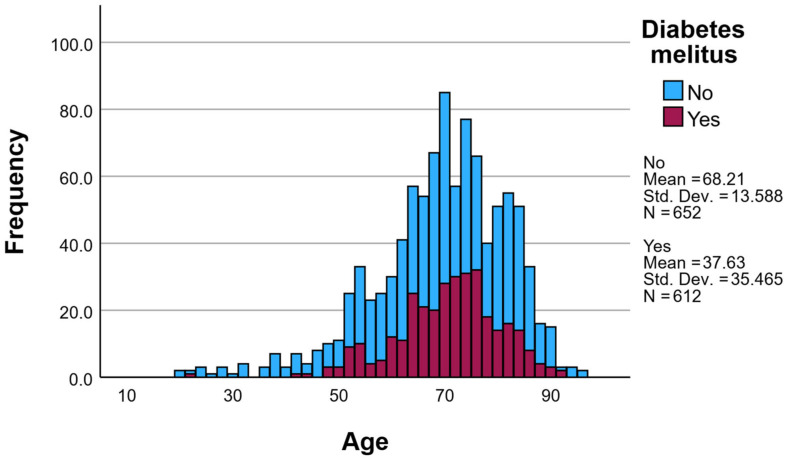 Figure 2
Figure 2- —UNIVERSITY OF ORADEA
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHyperglycemia and glycemic control in critically ill and hospitalized patients · Diabetes Treatment and Management · Sepsis Diagnosis and Treatment
1. Introduction
Diabetes mellitus (DM) is one of the most prevalent chronic diseases worldwide and represents a growing public health challenge. Its global burden continues to increase as a result of population aging, sedentary lifestyles, and the rising prevalence of obesity and cardiometabolic disorders. Consequently, diabetes mellitus is increasingly encountered among critically ill patients admitted to intensive care units (ICUs) [1,2,3].
In the critical care setting, patients with DM often present with a complex clinical profile characterized by multiple comorbidities, metabolic dysregulation, and reduced physiological reserve. These factors may contribute to a higher vulnerability during acute illness and may influence short-term outcomes, including survival. However, the independent role of diabetes mellitus in determining ICU mortality remains incompletely understood [4,5,6,7].
Diabetes mellitus is also characterized by chronic low-grade inflammation and immune dysregulation, which may amplify the systemic inflammatory response during critical illness. Inflammation plays a central role in the pathophysiology of organ failure and mortality in ICU patients. Therefore, the coexistence of diabetes and acute critical illness may create a pro-inflammatory milieu that contributes to worse outcomes [8].
Previous studies evaluating the impact of diabetes on ICU mortality have reported inconsistent findings. While some investigations suggest that diabetes is associated with increased short-term mortality, others have found comparable or even lower mortality rates among diabetic patients compared to non-diabetic patients. These discrepancies may be explained by differences in study populations, ICU case-mix, severity of illness, and methodological approaches [9,10,11,12].
Given this variability and the limited availability of real-world data derived from heterogeneous ICU populations, further evaluation of the prognostic role of diabetes mellitus is warranted. Therefore, the present study aimed to assess the association between diabetes mellitus and short-term mortality in critically ill adult patients admitted to a tertiary care intensive care unit.
Although the association between diabetes and ICU outcomes has been previously explored, contemporary real-world data from Eastern European ICU settings remain limited. Our study provides updated evidence from a large tertiary-care cohort reflecting current ICU practice and the increasing prevalence of diabetes among critically ill patients. This context-specific evidence may help refine local risk stratification and resource planning [13].
Therefore, the aim of this study was to evaluate whether diabetes mellitus is independently associated with short-term mortality in critically ill adult ICU patients. To address this objective, we conducted a retrospective observational study in a tertiary care intensive care unit, analyzing demographic and clinical characteristics as well as ICU outcomes in critically ill adult patients with and without diabetes mellitus.
2. Materials and Methods
2.1. Study Design and Population
We conducted a retrospective observational study in the Intensive Care Unit of the Bihor County Emergency Clinical Hospital, including all adult patients admitted between 1 January and 31 December 2024.
During the study period, 1517 patients were admitted to the ICU from medical wards, surgical wards (both postoperative and non-operative cases), or transferred from other hospitals. Patients younger than 18 years, those with incomplete medical records, patients with secondary forms of diabetes mellitus (drug-induced or related to endocrinopathies), and patients with gestational diabetes were excluded. After applying the exclusion criteria, a total of 1344 adult patients were included in the final analysis (Figure 1). The ICU serves a mixed medical–surgical population, including medical, postoperative, and emergency admissions, reflecting a heterogeneous tertiary-care ICU setting.
Diabetes mellitus was defined based on a documented medical history of diabetes, ongoing antidiabetic therapy, or diagnostic glycemic criteria including HbA1c ≥ 6.5%. Patients presenting with transient hyperglycemia without elevated HbA1c were not classified as diabetic, thereby reducing misclassification due to stress hyperglycemia.
Differentiation between type 1 and type 2 diabetes and precise disease duration were not consistently available in the medical records. Therefore, diabetes was analyzed as a binary variable.
Organ-support therapies such as mechanical ventilation, vasopressor use, and renal dysfunction were used as proxies for severity, as they represent core components of validated ICU scores.
Because validated ICU severity scores (e.g., APACHE II, SOFA, SAPS II) could not be calculated from the available retrospective data, illness severity was partially accounted for using clinically relevant organ-support variables. Specifically, the need for mechanical ventilation, inotropic/vasopressor support, and renal dysfunction were included as proxies for organ failure. These variables represent core components of established ICU severity scores and are recognized indicators of critical illness severity.
2.2. Data Collection
For each patient, the following data were collected from electronic medical records: demographic characteristics (age and sex), diabetes mellitus status, primary reason for ICU admission, and clinical outcome.
Additional clinical variables included major acute conditions and interventions relevant to critical illness, such as sepsis, acute kidney injury, and the need for mechanical ventilation. The primary outcome of interest was mortality during ICU hospitalization.
In addition to overall ICU mortality, 7-day and 28-day mortality were calculated based on the interval between ICU admission and death.
2.3. Statistical Analysis
Continuous variables were expressed as mean ± standard deviation, while categorical variables were reported as absolute numbers and percentages. Comparisons between patients with and without diabetes mellitus were performed using Student’s t-test for continuous variables and the chi-square test or Fisher’s exact test, as appropriate, for categorical variables.
To identify independent predictors of ICU mortality, a multivariate logistic regression model was constructed. Variables were selected a priori based on clinical relevance and established associations with mortality in critically ill patients, including age, sex, sepsis, acute kidney injury, mechanical ventilation, and diabetes mellitus status. Results were reported as adjusted odds ratios (ORs) with 95% confidence intervals (CIs).
Model performance was assessed using discrimination and calibration metrics, including the area under the receiver operating characteristic curve (AUC/ROC), the Hosmer–Lemeshow goodness-of-fit test, and the Brier score.
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 30.0 (IBM Corp., Armonk, NY, USA). A two-sided p-value < 0.05 was considered statistically significant.
2.4. Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Bihor County Emergency Clinical Hospital (Approval No. 36976/23.10.2023) and the Ethics Council of the same institution (Opinion No. 36746/20.10.2023). Due to the retrospective nature of the study, the requirement for informed consent was waived. All data were anonymized prior to analysis to ensure patient confidentiality.
3. Results
3.1. Study Population and Baseline Characteristics
During the study period, a total of 1344 adult patients admitted to the intensive care unit were included in the final analysis (Figure 1). The age of the patients ranged from 19 to 96 years, with a mean age of 67.95 ± 13.14 years and a median age of 70 years.
The largest proportion of patients belonged to the 60–79 years age group, accounting for 58.56% of the total cohort, with a peak observed in the 60–69 years interval (409 patients, 30.4%). Younger patients were underrepresented, with only 1.64% aged 18–29 years and 0.97% aged over 90 years.
Diabetes mellitus (DM) was identified in 435 patients (32.37%), while 909 patients (67.63%) had no documented diagnosis of diabetes. The prevalence of diabetes increased with age, reaching its highest value in patients aged 70–79 years (43.39%), followed by those aged 60–69 years (34.23%) (Figure 2). In patients younger than 40 years, diabetes was rare.
Patients with diabetes were significantly older than non-diabetic patients, with a mean age of 69.62 ± 10.26 years compared to 67.16 ± 14.26 years in the non-diabetic group (p < 0.001). The median age was 71 years in patients with DM versus 69 years in those without DM (Table 1).
Regarding sex distribution, diabetic patients were predominantly female (248 women, 57.0%), whereas the non-diabetic group showed a male predominance (491 men, 54.0%). This difference was statistically significant (p = 0.0002).
Concerning the reason for ICU admission, patients with diabetes were significantly more likely to be admitted for medical conditions compared to non-diabetic patients (73.79% vs. 64.36%, p = 0.0007). In contrast, surgical admissions were more frequent among patients without diabetes (35.64% vs. 26.21%, Table 2).
Overall, the study population represents a heterogeneous cohort of critically ill adults, with a substantial proportion of elderly patients and a high prevalence of diabetes mellitus, underscoring the clinical relevance of evaluating diabetes as a prognostic factor in the ICU setting.
3.2. ICU Mortality
Overall ICU mortality in the study population was 49.1% (660 deaths out of 1344 patients). Mortality differed significantly according to diabetes mellitus status.
Patients with diabetes mellitus had a significantly higher ICU mortality rate compared to non-diabetic patients (54.9% vs. 46.3%, p = 0.004). This difference remained clinically relevant and could not be explained solely by age distribution or admission type.
The proportion of deaths was consistently higher among patients with diabetes, indicating an increased short-term risk of adverse outcomes during critical illness. These findings support the hypothesis that diabetes mellitus is associated with a higher risk of mortality in the ICU setting.
Diabetes mellitus was associated with higher 28-day mortality compared to non-diabetic patients (52.8% vs. 44.3%, p = 0.005), while the difference in 7-day mortality did not reach statistical significance (32.6% vs. 28.9%, p = 0.18).
3.3. Multivariate Logistic Regression Analysis
To identify independent predictors of ICU mortality, a multivariate logistic regression model was constructed including clinically relevant covariates selected a priori: age, sex, sepsis, acute kidney injury, mechanical ventilation, and diabetes mellitus status, presented in Table 3. The dependent variable was death during ICU hospitalization.
After adjustment for these covariates, diabetes mellitus remained independently associated with increased ICU mortality (OR = 1.47, 95% CI 1.09–1.98, p = 0.011). Mechanical ventilation showed the strongest association with ICU death (OR = 49.98, 95% CI 29.12–85.77, p < 0.001), while acute kidney injury was also independently associated with mortality (OR = 2.02, 95% CI 1.46–2.79, p < 0.001). Increasing age was associated with a small but significant increase in risk per year (OR = 1.02, 95% CI 1.01–1.03, p = 0.002). Sex and sepsis were retained in the model due to clinical relevance; however, they did not reach statistical significance in this adjusted analysis.
3.4. Model Performance
The performance of the multivariate logistic regression model was evaluated using discrimination and calibration metrics. The model demonstrated good discriminatory ability, with an area under the receiver operating characteristic curve (AUC/ROC) of 0.88 (95% CI: 0.86–0.90), indicating a good discriminatory ability between survivors and non-survivors during ICU hospitalization.
Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test, which showed no evidence of poor fit (p = 0.80), suggesting good agreement between observed and predicted outcomes across risk deciles. Overall prediction accuracy was further supported by a low Brier score (0.137), indicating good probabilistic performance of the model.
Together, these results confirm that the multivariate model provides robust discrimination and adequate calibration for predicting ICU mortality in critically ill patients.
4. Discussion
In this retrospective cohort study of critically ill adult patients admitted to a tertiary care ICU, diabetes mellitus was associated with a significantly increased risk of short-term mortality. Importantly, this association persisted after adjustment for key demographic and clinical confounders, including age, sex, sepsis, acute kidney injury, and mechanical ventilation, confirming diabetes mellitus as an independent prognostic factor for ICU mortality.
The prevalence of diabetes mellitus in our ICU population (32.4%) is consistent with previous reports from mixed medical–surgical ICUs, reflecting the growing burden of diabetes among critically ill patients. As expected, patients with diabetes were older and more frequently admitted for medical conditions, highlighting a distinct clinical profile compared to non-diabetic patients. Despite these baseline differences, the persistence of the association between diabetes and mortality after multivariable adjustment suggests that diabetes itself contributes to increased vulnerability during critical illness, beyond age or admission type alone [6,10,14,15,16,17,18].
Notably, a prior meta-analysis [10] did not demonstrate a consistent association between diabetes and ICU mortality. Several factors may explain the discrepancy with our findings. First, that meta-analysis included studies conducted before contemporary ICU management strategies and before the widespread adoption of standardized glycemic control protocols. Second, ICU case-mix and patient profiles have evolved substantially over the past decade, with a higher burden of multimorbidity and metabolic disease in current ICU populations. Third, heterogeneity across earlier studies regarding diabetes definitions, severity adjustment, and outcome measures may have diluted potential associations. In contrast, our study used standardized diagnostic criteria, contemporary data, and multivariable adjustment for key confounders, which may provide a more updated estimate of the prognostic impact of diabetes in modern ICU practice. Nevertheless, differences in design and residual confounding should be considered when interpreting these comparisons [10,19].
Our findings align with several observational studies reporting higher ICU or in-hospital mortality among patients with diabetes, particularly in the context of acute organ dysfunction and severe infections. Although the exact mechanisms were not explored in the present analysis, the increased mortality risk observed in diabetic patients may be related to a combination of factors, including impaired immune response, reduced physiological reserve, and a higher susceptibility to acute metabolic and renal complications during critical illness. However, the present study was not designed to investigate mechanistic pathways, and such interpretations should be made with caution [4,10,17,20,21,22,23].
While the association between diabetes and ICU mortality has been previously explored, most evidence derives from older datasets or highly selected populations. Contemporary real-world data from Eastern European ICU settings remain limited. Our study provides updated evidence from a large tertiary-care cohort reflecting current ICU practices and case mix. Additionally, the relatively high prevalence of diabetes in our cohort underscores the growing clinical relevance of this issue in modern critical care. The association persisted in both early and 28-day mortality analyses, supporting the robustness of the findings.
Mechanical ventilation emerged as the strongest predictor of ICU mortality, reflecting the severity of respiratory failure rather than a modifiable risk factor. Acute kidney injury was also independently associated with death, underscoring the prognostic importance of organ dysfunction in critically ill patients. Within this clinical context, diabetes mellitus appears to act as a risk amplifier, increasing the likelihood of poor outcomes when critical illness occurs. Importantly, these results support the inclusion of diabetes status in early ICU risk assessment, alongside traditional markers of disease severity [9,24,25,26,27,28,29].
From a clinical standpoint, the identification of diabetes mellitus as an independent predictor of ICU mortality has practical implications. Early recognition of diabetic status on ICU admission may aid in risk stratification and support closer monitoring and individualized management strategies in this high-risk population. Given the increasing prevalence of diabetes worldwide, these findings are particularly relevant for contemporary intensive care practice [20,30,31,32,33,34,35].
Limitations
This study has several limitations that should be acknowledged. First, its retrospective observational design precludes the establishment of causal relationships between diabetes mellitus and ICU mortality, and residual confounding by unmeasured variables cannot be excluded.
Second, this was a single-center study, which may limit the generalizability of the findings to ICUs with different patient case-mix, admission policies, or management protocols. Multicenter studies are needed to confirm these results across diverse healthcare systems.
Third, validated ICU severity scores (e.g., APACHE II, SOFA, SAPS II) and detailed baseline comorbidity data were not consistently available and therefore could not be included in the multivariable model. To partially address illness severity, major organ-support variables such as mechanical ventilation, vasopressor use, and renal dysfunction were used as proxies; however, these do not fully replace formal severity scores, and residual confounding related to baseline severity remains possible.
Fourth, diabetes-related characteristics—including disease duration, subtype, prior glycemic control, HbA1c levels, and pre-admission antidiabetic treatments—were not consistently available. In addition, admission glucose levels, glycemic variability, insulin therapy, and hypoglycemic events were not analyzed. These factors may influence ICU outcomes and could partially mediate the observed association between diabetes and mortality.
Fifth, data on several chronic comorbidities (e.g., cardiovascular disease, chronic liver disease, obesity, and malignancy) were incomplete, which may have contributed to residual confounding.
Finally, only short-term ICU mortality was evaluated. Long-term outcomes, including post-discharge mortality and functional recovery, were beyond the scope of this study and warrant further investigation.
5. Conclusions
In this retrospective cohort study of critically ill adult patients, diabetes mellitus was independently associated with increased short-term mortality in the intensive care unit. Even after adjustment for major demographic and clinical confounders, the presence of diabetes remained a significant predictor of ICU death.
These findings highlight diabetes mellitus as an important prognostic marker in critically ill patients and emphasize the need for early recognition and appropriate risk stratification upon ICU admission. Given the increasing prevalence of diabetes in aging populations, integrating diabetic status into routine ICU assessment may help refine risk stratification in critically ill patients.
Further prospective and multicenter studies are warranted to better elucidate the mechanisms underlying this association and to identify targeted strategies aimed at improving outcomes in critically ill patients with diabetes mellitus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hossain M.J. Al-Mamun M. Islam M.R. Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused Health Sci. Rep.20247 e 200410.1002/hsr 2.200438524769 PMC 10958528 · doi ↗ · pubmed ↗
- 2Pan C. Cao B. Fang H. Liu Y. Zhang S. Luo W. Wu Y. Global burden of diabetes mellitus 1990–2021: Epidemiological trends, geospatial disparities, and risk factor dynamics Front. Endocrinol.202516202510.3389/fendo.2025.1596127 PMC 1225945740666058 · doi ↗ · pubmed ↗
- 3Khan M.A.B. Hashim M.J. King J.K. Govender R.D. Mustafa H. Al Kaabi J. Epidemiology of type 2 diabetes—Global burden of disease and forecasted trends J. Epidemiol. Glob. Health 20201010711110.2991/jegh.k.191028.00132175717 PMC 7310804 · doi ↗ · pubmed ↗
- 4Guan H. Tian J. Wang Y. Niu P. Zhang Y. Zhang Y. Fang X. Miao R. Yin R. Tong X. Advances in secondary prevention mechanisms of macrovascular complications in type 2 diabetes mellitus patients: A comprehensive review Eur. J. Med. Res.20242915210.1186/s 40001-024-01739-138438934 PMC 10910816 · doi ↗ · pubmed ↗
- 5Antar S.A. Ashour N.A. Sharaky M. Khattab M. Ashour N.A. Zaid R.T. Roh E.J. Elkamhawy A. Al-Karmalawy A.A. Diabetes mellitus: Classification, mediators, and complications; A gate to identify potential targets for the development of new effective treatments Biomed. Pharmacother.202316811573410.1016/j.biopha.2023.11573437857245 · doi ↗ · pubmed ↗
- 6Bodke H. Wagh V. Kakar G. Diabetes Mellitus and Prevalence of Other Comorbid Conditions: A Systematic Review Cureus 202315 e 4937410.7759/cureus.4937438146555 PMC 10749406 · doi ↗ · pubmed ↗
- 7Paduraru L. Vesa C.M. Popoviciu M.S. Ghitea T.C. Zaha D.C. Interrelationship between dyslipidemia and hyperuricemia in patients with uncontrolled type 2 diabetes: Clinical implications and a risk identification algorithm Healthcare 202513260510.3390/healthcare 1320260541154282 PMC 12562356 · doi ↗ · pubmed ↗
- 8Alexander M. Cho E. Gliozheni E. Salem Y. Cheung J. Ichii H. Pathology of diabetes-induced immune dysfunction Int. J. Mol. Sci.202425710510.3390/ijms 2513710539000211 PMC 11241249 · doi ↗ · pubmed ↗