Clinical Application of Inhaled Nitric Oxide in Conditions of Excessive Right Heart Load: A Review from Neonatal Pulmonary Hypertension to Perioperative Cardiac Surgery Management
Chengming Hu, Zhe Chen, Lizhi Lv, Yan Zhu, Yan Chen, Qiang Wang

TL;DR
This review examines the use of inhaled nitric oxide to manage right heart strain in neonates and cardiac surgery patients, highlighting its benefits and limitations in various clinical settings.
Contribution
The paper provides a comprehensive synthesis of iNO's clinical applications and outcomes in conditions of excessive right heart load across different patient populations.
Findings
iNO improves oxygenation in neonates with PPHN but does not significantly affect survival or neurodevelopment.
In adults with ARDS, iNO offers temporary benefits without mortality reduction and may increase acute kidney injury risk.
Perioperative iNO use in cardiac surgery can reduce pulmonary hypertension crises and ICU stays, though survival benefits remain unproven.
Abstract
Excessive right heart load imposes an acute or chronic injury on the right ventricle (RV), predisposing critically ill neonates and cardiac surgical patients to RV failure, low cardiac output syndrome, and death. Inhaled nitric oxide (iNO) is a selective pulmonary vasodilator that improves ventilation–perfusion matching and unloads the RV without systemic hypotension; nonetheless, its application beyond established neonatal indications remains contentious. Our review synthesizes current mechanistic, translational, and clinical evidence regarding iNO use in three major settings characterized by excessive RV load: (1) neonatal pulmonary hypertension, particularly PPHN; (2) acute and chronic RV overload in older children and adults, including secondary pulmonary hypertension, acute respiratory distress syndrome (ARDS), and acute pulmonary embolism; and (3) perioperative and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
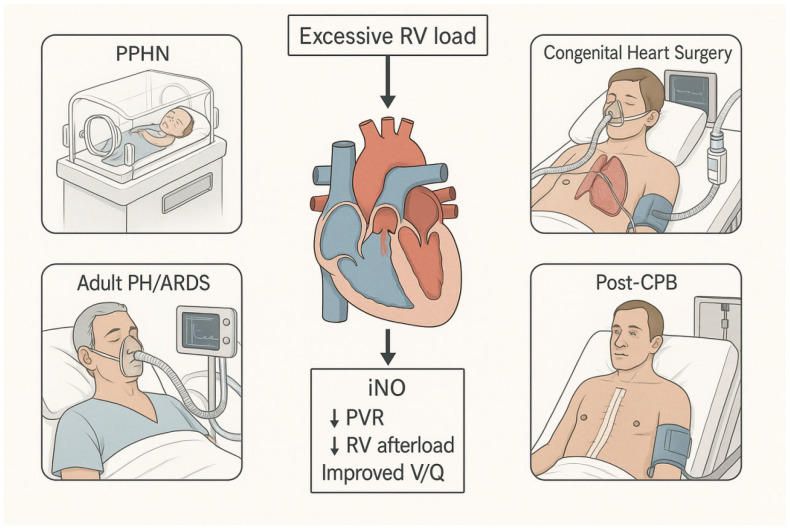 Figure 1
Figure 1- —Science and Technology Innovation Fund-Major Science and Technology Innovation Research and Development Special Project
- —Capital’s Funds for Health Improvement and Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Cardiac and Coronary Surgery Techniques · Congenital Heart Disease Studies
1. Introduction
1.1. Background
Nitric oxide (NO) is a gaseous signaling molecule synthesized endogenously by nitric oxide synthases (NOS) in vascular endothelium, where it plays an important role in the regulation of vascular tone, platelet function, and inflammation [1]. Across both the systemic and pulmonary vasculatures, endothelial-derived NO diffuses into adjacent vascular smooth muscle cells, activates soluble guanylate cyclase, and increases cyclic guanosine monophosphate (cGMP), thereby promoting smooth-muscle relaxation and vasodilation [2]. Pharmacologic delivery of NO by inhalation (inhaled nitric oxide, iNO) exploits these same pathways but confines the vasodilatory effect to the pulmonary vasculature: NO is delivered to ventilated alveoli, diffuses into the pulmonary capillary bed, and is rapidly bound and inactivated by hemoglobin, thereby avoiding the systemic vasodilation and hypotension induced by intravenous vasodilators [3].
An increase in pulmonary vascular resistance (PVR), whether acute or chronic, imposes an excessive pressure load on the right ventricle (RV) [4,5,6]. In the acute setting, a steep rise in PVR abruptly increases RV afterload, reduces RV stroke volume, and can lead to RV dilation, an interventricular septal shift, and impaired left ventricular filling, ultimately lowering systemic cardiac output and hypotension [4,5,7]. Chronic elevation of PVR drives RV hypertrophy, progressive dilatation, and eventual RV failure [4,5]. These hemodynamic disturbances are particularly hazardous in perioperative and critical care settings, where small deteriorations in RV function may precipitate circulatory collapse. A selective pulmonary vasodilator that can rapidly reduce PVR without compromising systemic arterial pressure is, therefore, an attractive therapeutic option in patients with an already vulnerable RV [8,9,10].
1.2. Disease Burden and Clinical Impact
In clinical practice, many diseases can lead to an increase in pulmonary vascular resistance [11,12]. Persistent Pulmonary Hypertension of the Newborn (PPHN) is a rare but extremely threatening condition that can cause hypoxic respiratory failure in full-term and near-term infants. Numerous instances necessitate mechanical breathing and high-concentration oxygen treatment. When pharmacological intervention proves futile, the implementation of extracorporeal membrane oxygenation (ECMO) technology is necessary. These survivors frequently experience prolonged NICU stays and an increased risk of long-term neurodevelopmental, auditory, and respiratory sequelae [11,13,14]. Complex congenital heart disease (CHD) is another major source of morbidity related to excessive right ventricular (RV) load. Lesions with increased pulmonary blood flow or pre-existing pulmonary hypertension often require early repair under cardiopulmonary bypass (CPB). In this setting, the reactive pulmonary vasculature and elevated PVR predispose patients to perioperative pulmonary hypertensive crises, RV failure, and low cardiac output syndrome (LCOS). These complications are associated with higher perioperative mortality, increased inotrope and ECMO use, and prolonged ICU and hospital stays [15,16,17]. Similar hemodynamic challenges are seen in adults with secondary pulmonary hypertension due to left heart disease, chronic lung disease, or acute respiratory distress syndrome (ARDS), particularly during and after CPB [12]. Across these settings, current therapies—systemic vasodilators and inodilators—can reduce PVR but frequently cause systemic hypotension and impaired organ perfusion, while ECMO, although effective, is invasive, resource-intensive, and prone to complications [18,19].
1.3. Existing Therapeutic Strategies and Limitations
Currently, management of excessive PVR and RV load relies on a combination of high inspired oxygen, optimized ventilatory strategies (including high-frequency ventilation), inotropic and inodilator support (e.g., dobutamine, milrinone), and vasodilators with both systemic and pulmonary effects such as prostacyclin analogs or phosphodiesterase-5 inhibitors [20,21]. In refractory cases, ECMO is used as a salvage option to support gas exchange and circulation while PVR gradually falls or the underlying disease is treated [19,22,23].
These approaches are limited by non-selective vasodilation, systemic hypotension, and the need for high-resource infrastructure, particularly for prostacyclin infusions and ECMO. Such resources are often unavailable in resource-limited settings [24,25]. In this context, iNO is conceptually attractive as a selective pulmonary vasodilator and RV afterload reducer: it is delivered to ventilated lung units and rapidly inactivated in the bloodstream. It can lower PVR and improve ventilation–perfusion matching with minimal impact on systemic arterial pressure, filling an important therapeutic gap in the management of patients with excessive right heart load [18,26,27,28].
1.4. Objectives and Scope of the Review
The aim of this review is to summarize the clinical application of iNO in three key settings characterized by excessive right ventricular load: (1) neonatal pulmonary hypertension, particularly persistent pulmonary hypertension of the newborn (PPHN); (2) diseases with excessive right heart load in children and adults, including secondary pulmonary hypertension and acute or chronic right ventricular failure; and (3) patients undergoing cardiopulmonary bypass, with a focus on intraoperative and early postoperative periods. Our review updates the perioperative iNO evidence base with recent RCTs and large post-marketing studies, and integrates them into practical algorithms for right-heart-focused perioperative care. Because several studies span more than one clinical scenario (e.g., mixed neonatal, pediatric and perioperative contexts), we assigned each study to a primary category based on the predominant population and timing of iNO use; the classification is presented in Appendix A Table A1.
We emphasize clinical evidence from randomized and observational studies, integrate relevant pathophysiologic rationale, and critically examine current controversies regarding efficacy, safety, dosing, and cost-effectiveness. Particular attention will be paid to the surgical and perioperative implications of iNO use in congenital and adult cardiac surgery. Table 1 and Figure 1 will schematically depict the major clinical scenarios associated with excessive right ventricular load (PPHN, congenital heart surgery, adult PH/ARDS, and post-CPB RV dysfunction) and illustrate where iNO is typically incorporated into management algorithms. Other rare and heterogeneous entities (e.g., pulmonary vein obstruction and complex congenital shunt physiology, such as a large PDA or d-TGA with PH) are beyond the scope of this review and typically require individualized hemodynamic assessment [29,30].
2. Theoretical Background
2.1. Key Phenotype-Specific Mechanisms Across PH Groups
The predominant cause of PH phenotypes, and consequently the anticipated function of iNO, varies by WHO classification and clinical scenario (Table 2) [30]. Neonatal PH, PPHN and perioperative (e.g., CPB-related) reactive PH are characterized mainly by acute, recruitable vasoconstriction and endothelial dysfunction with reduced NO bioavailability, making iNO most plausibly effective for rapid, lung-selective PVR reduction and RV unloading [47]. Group 1 PAH combines endothelial imbalance with progressive arteriolar remodeling, so iNO may be useful for short-term stabilization or vasoreactivity assessment, but responses diminish as fixed structural disease predominates. Group 2 PH is primarily post-capillary with elevated left-sided filling pressures, with some patients developing combined post- and pre-capillary remodeling; in this setting, selective pulmonary vasodilation may increase pulmonary blood flow and worsen pulmonary edema, so iNO should be a tightly monitored in a short trial with clear stopping rules. Group 3 PH associated with lung disease reflects hypoxic vasoconstriction, inflammatory endothelial injury, microthrombosis, and marked V/Q heterogeneity; iNO can transiently improve oxygenation via V/Q redistribution and may reduce RV afterload when ventilated units are recruitable, but it does not reverse underlying parenchymal pathology. Group 4 PH is driven by pulmonary arterial obstruction, where iNO serves mainly as short-term RV support rather than definitive therapy. Group 5 PH is multifactorial and heterogeneous, often presenting mixed pre-/post-capillary components, leading to unpredictable iNO responsiveness and emphasizing individualized, mechanism-guided use.
2.2. Pathophysiology of Excess Right Heart Load
The right ventricle (RV) is coupled to low-pressure, high-compliance pulmonary circulation, so even modest acute or chronic rises in PVR markedly increase RV afterload, leading to RV dilation, septal shift, reduced left ventricular filling, and ultimately systemic hypotension and organ hypoperfusion [48,49]. In neonates, failure of the normal postnatal decline in PVR maintains a fetal pattern of circulation with persistent patency of the ductus arteriosus and foramen ovale, resulting in right-to-left shunting, severe hypoxemia, and progressive RV dysfunction [50]. After cardiopulmonary bypass (CPB), blood–surface interactions trigger contact activation, referring to activation of the intrinsic coagulation and contact system (factor XII–kallikrein–kinin), with downstream complement, inflammatory cascades and platelet activation [51,52]; together with ischaemia–reperfusion injury, and inflammatory mediator release, these processes promote endothelial dysfunction and vasoconstriction in the pulmonary bed, acutely raising PVR and predisposing susceptible patients to RV failure and pulmonary hypertensive crises [53,54,55]. In adult patients, when ARDS is accompanied by secondary pulmonary hypertension, acute pulmonary embolism, and decompensated chronic pulmonary hypertension, the right ventricle is also subjected to similar hemodynamic pressure effects. In these cases, acute or progressive obstruction and remodeling of the pulmonary vessels suddenly increase the afterload of the right ventricle and may lead to rapid hemodynamic collapse [12].
2.3. Endogenous NO and Exogenous iNO
2.3.1. Endogenous NO Production and the NO–sGC–cGMP Axis
Endogenous NO is generated from L-arginine by nitric oxide synthase (NOS) isoforms, with endothelial NOS (eNOS) being the dominant vascular source [2]. Shear stress, oxygen tension, and cofactors such as tetrahydrobiopterin regulate eNOS coupling; oxidative stress can uncouple eNOS and reduce NO bioavailability. NO diffuses into pulmonary arterial smooth-muscle cells and activates soluble guanylate cyclase (sGC), increasing intracellular cyclic guanosine monophosphate (cGMP) [56]. cGMP activates protein kinase G, decreases intracellular calcium, and promotes smooth-muscle relaxation; it also exerts anti-proliferative and anti-platelet effects that are relevant to chronic pulmonary vascular disease [57].
cGMP signaling is terminated primarily by phosphodiesterase enzymes, especially phosphodiesterase type 5 (PDE5), which is highly expressed in the pulmonary vasculature and upregulated in several PH phenotypes [58]. PDE5 inhibitors (e.g., sildenafil and tadalafil) can potentiate NO-mediated vasodilation and help prevent rebound PH during iNO weaning. Milrinone (a PDE3 inhibitor) may be used as adjunct support, but because it dilates both systemic and pulmonary arteries, it can cause systemic hypotension and should be carefully titrated with hemodynamic monitoring [59]. Conversely, in patients with elevated left-sided filling pressures, augmenting pulmonary blood flow through NO–cGMP pathways may increase pulmonary edema risk; thus, combined use requires careful titration and hemodynamic monitoring.
2.3.2. Exogenous iNO
Clinically, iNO is delivered via the inspiratory limb of the ventilatory circuit or through nasal continuous positive airway pressure and high-flow systems in spontaneously breathing patients, allowing precise titration of the inspired concentration [60,61]. Inhaled nitric oxide (iNO) induces selective pulmonary vasodilation via administered directly to ventilated alveoli, diffusion into neighboring pulmonary vessels, and swift binding and inactivation by hemoglobin, thereby confining its effects to pulmonary circulation and reducing systemic vasodilation [18,26,27]. However, iNO responsiveness depends on the presence of recruitable, well-ventilated lung units. In patients with extensive consolidation, atelectasis and alveolar flooding (e.g., surfactant deficiency, edema, and pneumonia), iNO delivery to functional alveoli may be limited, so it is necessary to first optimize the expansion effect of the lungs and treat any potential lung parenchymal lesions before iNO [37]. In clinical practice, iNO is generally administered at concentrations ranging from 5 to 40 parts per million (ppm), exhibiting a swift onset and offset of effect within minutes of dose modification, showing that most oxygenation and hemodynamic benefit is achieved at relatively low doses (20 ppm in many neonatal and adult studies) [8,31,32]. It also demonstrates a distinct “ceiling effect,” where further increases in dosage beyond a modest threshold (typically 20–40 ppm) yield minimal additional enhancement in oxygenation or hemodynamics [31,32]. Upon absorption, NO interacts with haemoglobin to produce methaemoglobin (metHb) and nitrate; it also interacts with thiol-containing compounds to yield nitrite and S-nitrosothiols, which may serve as a circulating reservoir of NO and contribute to more nuanced systemic effects [9,62,63].
2.4. Preclinical and Translational Evidence
Recent experimental work has refined our understanding of how NO-based interventions interact with pulmonary vascular mechanics and remodeling. In a monocrotaline-induced PAH rat model, inhaled NO produces frequency-dependent improvements in pulmonary arterial impedance, suggesting that the mechanical response to NO varies with disease state rather than reflecting a uniform vasodilatory effect [64]. In hypoxia-induced PH models, modulation of multiple nodes along the NO–sGC–cGMP pathway (e.g., augmenting NO availability and limiting cGMP degradation) attenuated pulmonary vascular changes and right ventricular remodeling, supporting the concept that impaired NO signaling is both a marker and a mechanistic contributor to experimental PH progression [65]. These in vivo findings complement clinical observations by highlighting when NO responsiveness may reflect recruitable vasoconstriction versus fixed structural disease.
Mechanistic insight from in vitro and cellular systems further supports phenotype-specific NO biology. In the Sugen–hypoxia model, carbonic anhydrase inhibition improved pulmonary artery reactivity and enhanced NO-mediated relaxation mechanisms, illustrating that restoring vasodilatory reserve can be model- and pathway-dependent [66]. Cellular studies also implicate dysregulated NOS activity in remodeling: macrophage inducible NOS (iNOS) signaling has been linked to proliferative crosstalk with adjacent pulmonary artery smooth muscle cells, providing a plausible inflammatory–NO axis for vascular remodeling [67]. In ARDS, iNOS-driven high-output NO together with inflammation-associated superoxide favors rapid peroxynitrite (ONOO−) formation (k = 1.6 × 10^−10^ M^−1^s^−1^), which can contribute to nitro-oxidative tissue injury and may help explain the limited response to iNO [68,69,70]. Finally, translational formulation work has tested alternative NO-delivery strategies in small-animal lung injury models; for example, NO-releasing nanoparticles reduced inflammatory injury in an LPS-induced ARDS model, supporting ongoing development of NO-based platforms beyond conventional gaseous delivery [71]. Collectively, these experimental studies provide updated mechanistic rationale for future research, including phenotype-guided use and combination strategies targeting the NO–cGMP axis.
2.5. Clinical Delivery, Monitoring and Safety
Inhaled nitric oxide is usually supplied as a compressed gas and delivered via a calibrated injector/blender with inline monitoring of NO, NO_2_ and FiO_2_ integrated into the ventilator circuit [72,73,74]. It can be administered through conventional invasive mechanical ventilation, high-frequency oscillatory ventilation, selected non-invasive or high-flow systems, and, in the cardiac surgical setting, by adding NO to the sweep gas of the CPB oxygenator [75,76]. Safe use requires regular measurement of methaemoglobin, continuous surveillance of delivered NO and NO_2_ concentrations with alarm thresholds, adherence to recommended exposure limits for staff, and appropriate scavenging to minimize ambient contamination [35,77,78]. Recognized adverse effects include dose-related methaemoglobinemia, NO_2_-induced pulmonary toxicity at excessive concentrations, rebound pulmonary hypertension with abrupt withdrawal, and potential oxidative or nitrosative stress with prolonged or high-dose therapy; key delivery modes, target doses, monitoring parameters, and safety thresholds are summarized in Table 3.
3. Research Status
3.1. Neonatal Pulmonary Hypertension and Hypoxic Respiratory Failure
The pivotal randomized trials of iNO in term and near-term infants with hypoxic respiratory failure involved enrolling mechanically ventilated neonates ≥ 34 weeks of gestation with oxygenation index (OI) ≥ 25 (OI = FiO_2_ × MAP × 100/PaO_2_) and no structural heart disease, and comparing conventional therapy alone with adjunctive iNO [31,79]. In the multicenter Neonatal Inhaled Nitric Oxide Study Group trial, infants received 20 ppm iNO (with escalation to 80 ppm in non-responders) or 100% oxygen, and iNO significantly reduced the composite of death or ECMO at 120 days (46% vs. 64%) by lowering ECMO use (39% vs. 54%), while mortality was unchanged (14% vs. 17%) [31]. In the low-dose trial by Clark et al., neonates meeting similar criteria received 20 ppm iNO for up to 24 h followed by 5 ppm for ≤96 h versus control gas, leading to a reduction in ECMO requirement from 64% to 38%, with no difference in 30-day mortality (7% vs. 8%) and a lower incidence of chronic lung disease (7% vs. 20%) [32]. Collectively, these RCTs demonstrate that iNO reliably improves oxygenation and decreases the need for ECMO in severe neonatal pulmonary hypertension, but confers little or no survival advantage.
3.2. Diseases with Excessive Right Heart Load in Children and Adults
3.2.1. ARDS with Secondary Pulmonary Hypertension
In adults and children with ARDS and secondary pulmonary hypertension, randomized trials and meta-analyses show that iNO produces only transient physiological benefit without improving survival [8,80,81,82]. More recently, high-dose iNO has been explored in COVID-19-related acute hypoxemic respiratory failure; a multicenter phase II trial reported improved oxygenation at 48 h versus usual care, but was not powered to detect differences in mortality or longer-term outcomes [83]. The Cochrane review (14 RCTs, ~1300 patients) found a significant increase in PaO_2_/FiO_2_ at 24 h (mean difference 15.9, 95% CI 8.3–23.6) and an improved oxygenation index, but no reduction in longest-follow-up mortality (38.2% vs. 37.5%; RR 1.04, 95% CI 0.90–1.19), no gain in ventilator-free days, duration of mechanical ventilation, or ICU/hospital length of stay [80]. A separate meta-analysis of nine ARDS trials (n = 1142) likewise showed no mortality benefit in either severe (PaO_2_/FiO_2_ ≤ 100; RR 1.01, 95% CI 0.78–1.32) or mild–moderate ARDS (RR 1.12, 95% CI 0.89–1.42) [84]. Importantly, iNO was associated with an increased risk of renal impairment (RR 1.59, 95% CI 1.17–2.16) [80]. These data support the physiological theoretical basis—in ventilated lung units, selective pulmonary vascular dilation can improve the matching of ventilation and perfusion, reduce pulmonary vascular resistance, and quickly alleviate the burden on the right ventricle. But at the same time, they also indicate that this cannot translate into better long-term efficacy. Therefore, in acute ARDS, iNO should be regarded as a short-term emergency treatment for refractory hypoxemia and right ventricular dysfunction, rather than a treatment that can improve the condition, particularly considering its potential adverse effects, substantial cost and resource implications [8,80,81].
3.2.2. Acute Pulmonary Embolism and Acute RV Failure
In acute pulmonary embolism (PE) with right ventricular (RV) failure, evidence for iNO comes mainly from studies with small case series and one randomized trial [85,86,87,88,89]. Case series of massive PE treated with 20–25 ppm iNO report rapid improvements in pulmonary and systemic arterial pressures, heart rate, and gas exchange within minutes, with all four patients in one series surviving to hospital discharge [85,86]. A systematic review of iNO for acute PE identified a majority of case reports and small cohorts (plus an 8-patient phase I trial) and concluded that most patients showed prompt gains in oxygenation and hemodynamics; however, the data were insufficient to prove safety or efficacy or any mortality benefit [87,88]. In the multicenter iNOPE randomized trial of 76 patients with submassive PE and RV dysfunction, 50 ppm iNO for 24 h did not significantly increase the proportion of patients achieving a composite endpoint of normal RV size/function and low troponin (13% placebo vs. 24% iNO; p = 0.375), although a pre-planned post hoc analysis showed a higher rate of resolution for RV hypokinesis/dilation with iNO (+29%; p = 0.010) [89]. Beyond PE, observational data in cardiogenic shock and severe RV failure (often on VA-ECMO or ECPELLA) suggest that iNO can improve RV performance and device flows and may facilitate earlier weaning from mechanical support, but without robust controlled outcome data [90,91]. Overall, these studies support the use of iNO as a rescue bridge therapy to acutely unload the RV and stabilize oxygenation while definitive treatment (anticoagulation, thrombolysis, catheter/surgical embolectomy, or mechanical circulatory support) is instituted, rather than as a stand-alone, outcome-modifying therapy for acute PE or RV failure [87,89,91].
In adult diseases characterized by excessive load on the right ventricle, iNO can reliably provide short-term physiological benefits, enabling rapid improvement in oxygenation, pulmonary artery pressure, and right ventricular function in many patients. However, in this study, iNO did not significantly reduce mortality, mechanical ventilation time, or length of stay in the intensive care unit, and long-term use may cause damage to the kidneys. Taken together, these data support positioning iNO not as a chronic or disease-modifying therapy, but as a targeted, time-limited support tool—used to transiently reduce RV afterload and stabilize gas exchange while definitive treatments (reperfusion, surgery, optimization of heart failure and PH therapy, or mechanical support) are implemented.
3.3. Perioperative and Post-Cardiopulmonary Bypass Use
3.3.1. Rationale in Cardiac Surgery
Cardiopulmonary bypass (CPB) triggers a systemic inflammatory and ischaemia–reperfusion response that promotes endothelial dysfunction, oxidative stress and vasoconstriction in the pulmonary circulation, leading to increased PVR, impaired RV–pulmonary artery coupling and a predictable fall in cardiac output after surgery; in infants and children with pre-existing high pulmonary flow or pressure, this milieu predisposes to postoperative pulmonary hypertensive crises, RV failure and LCOS [53,54,92,93]. iNO acting directly on pulmonary vascular smooth muscle and rapidly inactivated by hemoglobin, can counteract this surge in PVR, improve RV forward flow and attenuate the cascade leading to PHT crises and LCOS, providing a strong mechanistic rationale for its prophylactic or early postoperative use in high-risk congenital and adult cardiac surgery [15,38,54].
3.3.2. Prophylactic Postoperative iNO in Congenital Heart Surgery
In congenital heart surgery, the best evidence for prophylactic postoperative iNO comes from the randomized double-blind trial by Miller et al., which enrolled 124 infants (median age 3 months) with high pulmonary flow and/or pressure undergoing corrective surgery for lesions such as large VSD, complete AVSD, truncus arteriosus, or total anomalous pulmonary venous drainage, all with preoperative pulmonary hypertension. Infants were randomized to continuous 10 ppm iNO or placebo from arrival in the ICU until just before extubation [15]. Compared with placebo, iNO significantly reduced pulmonary hypertensive crises (median 4 [IQR 0–12] vs. 7 [1–19] episodes; adjusted RR 0.65, p = 0.045) and shortened the time to meeting extubation criteria (80 [38–121] vs. 112 h [63–164], p = 0.019), with fewer patients still ventilated at 7 days (10% vs. 26%, p = 0.02) and a shorter total time on gas (87 [43–125] vs. 117 h [67–168], p = 0.023). Trends toward reduced total ventilation time (117 vs. 140 h) and ICU stay (138 vs. 162 h) favored iNO but did not reach statistical significance; in addition, mortality (6.5% overall) was similar between groups [15]. Collectively, these data support routine low-dose postoperative iNO in selected high-risk congenital repairs to prevent pulmonary hypertensive crises and accelerate postoperative stabilization, while its effects on ICU length of stay and survival remain modest and uncertain [15,16].
3.3.3. Intra-CPB NO Administration
Intraoperative delivery of nitric oxide via the CPB oxygenator has been evaluated most rigorously in the single-center RCT by James et al., in which 198 children undergoing congenital heart surgery were randomized to receive 20 ppm NO blended into oxygenator sweep gas for the entire duration of CPB or standard bypass without NO [17]. Children in the NO group developed LCOS significantly less often than controls (15% vs. 31%, p = 0.007), with the greatest benefit observed in those <6 weeks of age (20% vs. 52%, p = 0.012) and in those 6 weeks–2 years (6% vs. 24%, p = 0.026); in these younger cohorts, ICU length of stay was also reduced (median 43 vs. 84 h, p = 0.031). The incidence of LCOS after more complex procedures was similarly lower with intra-CPB NO (17% vs. 48%, p = 0.018); ECMO use was also markedly reduced (1% vs. 8%, p = 0.014) [17]. Earlier small pediatric and adult studies introducing NO into the CPB circuit demonstrated reductions in biochemical markers of myocardial injury and inflammation and suggested the potential for shorter ventilation and ICU stays, but were underpowered for hard clinical endpoints [94,95,96]. A recent systematic review and meta-analysis pooling pediatric and adult CPB studies similarly suggests improved early postoperative outcomes (e.g., shorter ICU stay), but heterogeneity and limited long-term endpoints preclude firm conclusions [97]. The NITRIC double-blind, multicenter randomized clinical trial (JAMA, 2022; n = 1371 children < 2 years) reported that NO delivered into the CPB oxygenator did not increase ventilator-free days compared with standard care, suggesting limited benefit of routine intra-CPB NO supplementation in this population [98]. Taken together, the current evidence does not support routine intra-CPB NO administration. While some single-center trials suggest potential benefits, the large multicenter NITRIC trial failed to show efficacy, indicating that intra-CPB NO should be considered investigational and further studies should be conducted in carefully designed, phenotype- and endpoint-driven trials.
3.3.4. After-CPB NO Administration
After CPB, many congenital and adult cardiac surgery patients develop acute pulmonary hypertension and RV dysfunction that can delay separation from bypass and compromise early postoperative stability [16,38,99]. In infants and children with preoperative pulmonary hypertension who develop elevated pulmonary pressures immediately after CPB, Russell et al. reported that iNO reduced mPAP without systemic hypotension, supporting its role in stabilizing hemodynamics in the early post-bypass period [99]. Evidence for routine prophylactic low-dose postoperative iNO after high-risk congenital heart surgery is discussed in detail in Section 3.3.2 [15]. In adults with severe postoperative pulmonary hypertension, iNO has been shown to lower mPAP more effectively with less systemic hypotension than intravenous prostacyclin [100,101,102], and to maintain higher RV ejection fraction and lower vasopressor requirements compared with milrinone in cardiac surgery patients [102]. Together, these data support inhaled NO as a selective pulmonary vasodilator that facilitates separation from CPB in patients with elevated PVR, stabilizes RV function, and promotes earlier postoperative recovery, particularly in high-risk congenital repairs and adult operations complicated by pulmonary hypertension [15,99,100,101,102]. Across these diverse clinical scenarios, multiple randomized trials and meta-analyses have evaluated the efficacy, safety, and organ-specific effects of iNO. The key randomized controlled trials and systematic reviews with major indications are summarized in Table A1.
4. Research Challenges and Controversies
Despite robust physiologic effects on oxygenation and pulmonary artery pressure, most randomized and observational studies of iNO have failed to demonstrate consistent improvements in hard outcomes such as mortality, neurologic sequelae, or long-term functional status. This might be due to the late initiation, short exposure, and the fundamentally multifactorial nature of neonatal PPHN, ARDS, and perioperative low-cardiac output [31,80]. Important uncertainties remain regarding optimal timing, dose, and duration—for example, prophylactic versus rescue use in cardiac surgery, early versus late initiation in PPHN, and the wide heterogeneity in clinical practice (with starting doses of 5–20 ppm or higher, variable titration and weaning schemes) in the absence of robust dose–response trials [38,103]. A rapid cessation of iNO may precipitate a clinically substantial rebound in pulmonary hypertension. Consequently, the dosage must be incrementally diminished, comprehensive hemodynamic monitoring should be performed throughout the drug cessation process, and for high-risk patients, it is essential to administer oral or intravenous pulmonary vasodilators concurrently [104,105]. Safety issues, while normally manageable, encompass methemoglobinemia, pulmonary toxicity associated with nitrogen dioxide, fluid-sensitive pulmonary edema in the presence of left-sided lesions, and the possibility of systemic oxidative or nitrosative stress. The enduring consequences of neonatal exposure on neurodevelopment and pulmonary growth, together with the effects of repeated treatments in geriatric patients, remain inadequately studied [31]. In parallel, the high cost and logistical complexity of iNO delivery (proprietary gas systems, continuous monitoring, and trained staff) in contrast to cheaper systemic alternatives such as sildenafil or prostacyclin, which themselves carry risks of systemic hypotension, and with the extreme resource demands of ECMO, create significant access and health-economic challenges, especially in low- and middle-income settings [35,106,107]. Finally, much of the evidence base is limited by small, single-center trials, heterogeneous patient populations and outcome definitions, and short follow-up periods focused on physiological or ICU end points, particularly in CPB-related studies and adult right-heart failure, leaving key questions about long-term efficacy, safety, and cost-effectiveness unanswered [38,103].
5. Conclusions and Future Directions
Inhaled nitric oxide now has an established role as a standard of care in term and near-term infants with persistent pulmonary hypertension of the newborn and severe hypoxic respiratory failure, where it reliably improves oxygenation and reduces ECMO use. In older children and adults, it functions mainly as an adjunctive therapy—a selective, short-acting pulmonary vasodilator used perioperatively in cardiac surgery for pulmonary hypertension and vulnerable right ventricles, and as temporary support in acute RV failure (e.g., ARDS-related PH, acute PE, post-CPB PH crises). In these settings, iNO is best viewed as a targeted tool to acutely reduce PVR, unload the RV, and stabilize gas exchange rather than a disease-modifying or chronic therapy, and should be integrated into multimodal RV support alongside inotropes, vasopressors, other pulmonary vasodilators, and, when necessary, mechanical circulatory support [8,80]. For surgeons, anesthesiologists, and intensivists, the practical take-home message is that iNO should be implemented judiciously and phenotype-specifically, with a clear understanding of the underlying pathophysiology and patient-specific hemodynamics, and delivered through standardized protocols for initiation, monitored response, titration, and weaning within a multidisciplinary team.
Looking forward, key research priorities include adequately powered multicenter RCTs in clearly defined high-risk subgroups (such as complex congenital heart surgery and adult RV failure), dose-finding and timing studies—including intra-CPB vs. postoperative strategies—systematic long-term follow-up of neonatal and pediatric cohorts, and robust cost-effectiveness and implementation analyses across different health systems. Mechanistic work on myocardial and distant organ protection, and on systemic NO biology in the context of CPB and critical illness, will help refine when and how iNO is most beneficial. Taken together, the existing evidence and strong physiologic rationale support a continued but judicious use of iNO: when applied in the right patient, at the right time, and embedded in comprehensive perioperative and critical-care pathways, it remains a valuable tool for managing conditions of excessive right heart load.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Palmer R.M. Ferrige A.G. Moncada S. Nitric Oxide Release Accounts for the Biological Activity of Endothelium-Derived Relaxing Factor Nature 198732752452610.1038/327524 a 03495737 · doi ↗ · pubmed ↗
- 2Loscher T.F. Endothelium-Derived Nitric Oxide: The Endogenous Nitrovasodilator in the Human Cardiovascular System Eur. Heart J.19911221110.1093/eurheartj/12.suppl_E.21790780 · doi ↗ · pubmed ↗
- 3Roberts J.D. Lang P. Bigatello L.M. Vlahakes G.J. Zapol W.M. Inhaled Nitric Oxide in Congenital Heart Disease Circulation 19938744745310.1161/01.CIR.87.2.4478425292 · doi ↗ · pubmed ↗
- 4Arrigo M. Huber L.C. Winnik S. Mikulicic F. Guidetti F. Frank M. Flammer A.J. Ruschitzka F. Right Ventricular Failure: Pathophysiology, Diagnosis and Treatment Card. Fail. Rev.2019514014610.15420/cfr.2019.15.231768270 PMC 6848943 · doi ↗ · pubmed ↗
- 5Vonk Noordegraaf A. Chin K.M. Haddad F. Hassoun P.M. Hemnes A.R. Hopkins S.R. Kawut S.M. Langleben D. Lumens J. Naeije R. Pathophysiology of the Right Ventricle and of the Pulmonary Circulation in Pulmonary Hypertension: An Update Eur. Respir. J.201953180190010.1183/13993003.01900-201830545976 PMC 6351344 · doi ↗ · pubmed ↗
- 6Lankhaar J.-W. Westerhof N. Faes T.J.C. Marques K.M.J. Marcus J.T. Postmus P.E. Vonk-Noordegraaf A. Quantification of Right Ventricular Afterload in Patients with and without Pulmonary Hypertension Am. J. Physiol. Heart Circ. Physiol.2006291 H 1731 H 173710.1152/ajpheart.00336.200616699074 · doi ↗ · pubmed ↗
- 7Bryce Y.C. Perez-Johnston R. Bryce E.B. Homayoon B. Santos-Martin E.G. Pathophysiology of Right Ventricular Failure in Acute Pulmonary Embolism and Chronic Thromboembolic Pulmonary Hypertension: A Pictorial Essay for the Interventional Radiologist Insights Imaging 2019101810.1186/s 13244-019-0695-930758687 PMC 6375098 · doi ↗ · pubmed ↗
- 8Griffiths M.J.D. Evans T.W. Inhaled Nitric Oxide Therapy in Adults N. Engl. J. Med.20053532683269510.1056/NEJ Mra 05188416371634 · doi ↗ · pubmed ↗