A Circulating Signature of Tumour Hybrid Cells and Immune Checkpoints Predicts Metastatic Progression in Lung Cancer
Gonzalo Sáenz de Santa María-Diez, Sandra Liana Pardo-Prieto, Roberto Lozano-Rodríguez, Urko Aguirre-Larracoechea, María Elena Corpa-Rodríguez, Julia del Prado-Montero, Verónica Terrón-Arcos, Karla Montalbán-Hernández, Daniel Arvelo-Rosario, Jesús Fernández-Felipe, Laura Córdoba

TL;DR
This study identifies a blood-based signature of tumor hybrid cells and immune checkpoints that can predict metastasis and survival in lung cancer patients.
Contribution
The study introduces a novel combination of circulating tumor hybrid cells and soluble immune checkpoints as a predictive biomarker for lung cancer progression.
Findings
Tumor hybrid cells and specific immune checkpoints (sCTLA-4, s-41BB, sLAG-3, sTIM-3) strongly discriminate metastatic status in lung cancer patients.
Levels of tumor hybrid cells, sLAG-3, and sTIM-3 distinguish deceased from surviving patients.
Integrated models of these biomarkers show high accuracy in predicting patient outcomes.
Abstract
Lung cancer remains the leading cause of cancer-related mortality worldwide and is frequently diagnosed at advanced stages, when metastatic dissemination is already present. Tumour hybrid cells (THCs) are rare circulating cells formed through fusion between cancer stem cells with leukocytes, predominantly monocytes. These cells combine traits from both lineages, conferring enhanced migratory, invasive and immune-evasive capacities that could promote metastasis. In parallel, soluble immune checkpoints (sICs) have emerged as minimally invasive biomarkers and indicators of systemic immune dysregulation and tumour-driven immune escape. In this study, 31 patients with lung cancer were prospectively enrolled at La Paz University Hospital (Madrid, Spain). Circulating THCs were quantified by spectral flow cytometry, and plasma sICs concentrations were determined using multiplex immunoassays.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
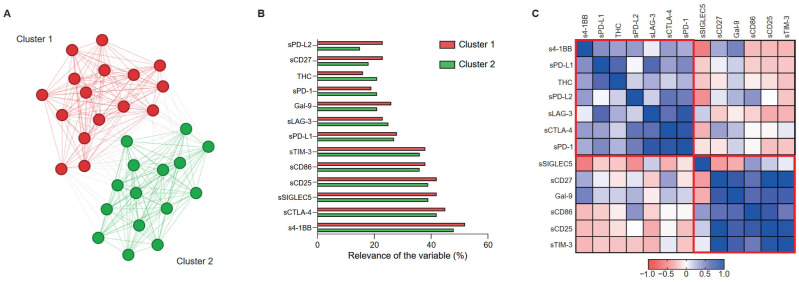 Figure 1
Figure 1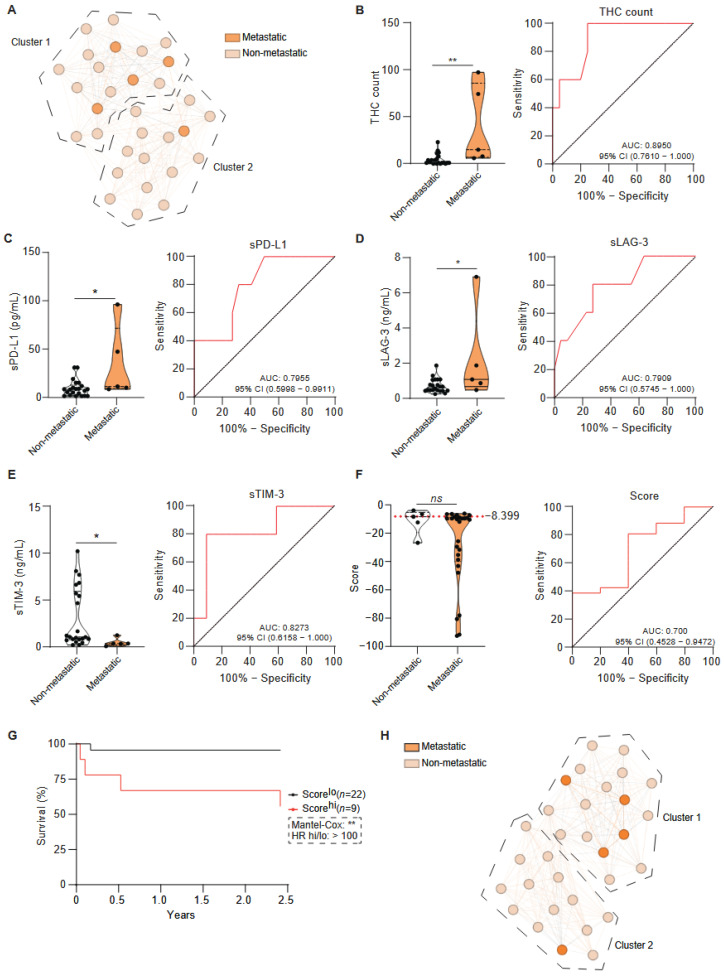 Figure 2
Figure 2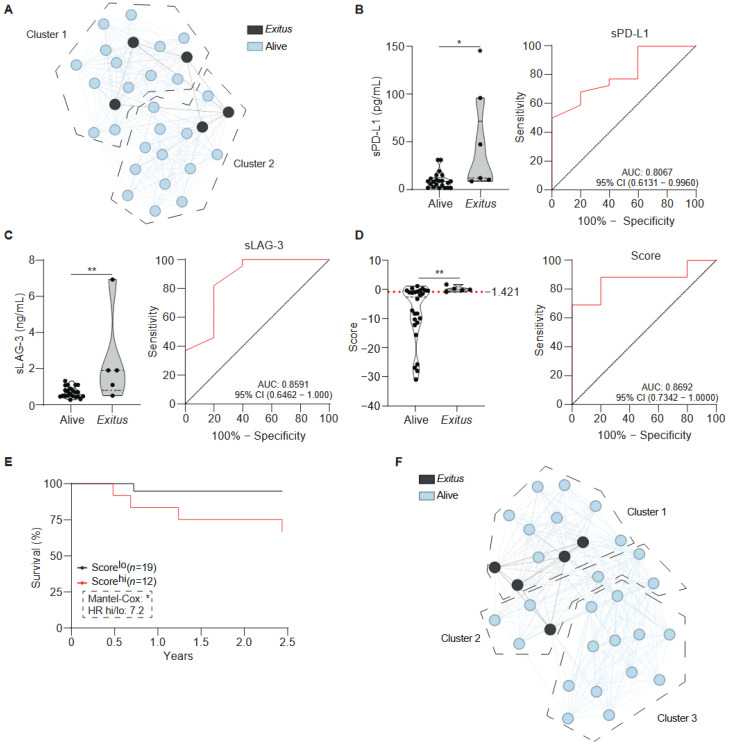 Figure 3
Figure 3- —Instituto de Salud Carlos III (ISCIII)
- —European Union
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Cells and Metastasis · Immune cells in cancer · Single-cell and spatial transcriptomics
1. Introduction
Lung cancer (LC) is the second-most commonly diagnosed malignancy worldwide yet remains the leading cause of cancer-related mortality, responsible for nearly two million deaths each year [1]. Tobacco smoking is recognised as a predominant risk factor, contributing to approximately 85% of all lung cancer cases [2]. Despite notable advancements in diagnosis and therapy, most patients are diagnosed at advanced stages, when metastatic dissemination has already occurred [3]. This late detection profoundly limits therapeutic options and contributes to persistently poor overall survival associated with the disease. As with other solid tumours, metastatic spread accounts for more than 90% of LC-related deaths [4].
The biological mechanisms underlying metastasis remain poorly understood. Classical models emphasise the role of circulating tumour cells (CTCs), which detach from the primary lesion, intravasate into the bloodstream, survive immune attack, and colonise distant organs [4,5]. Several theories have been proposed to explain this process. The “seed and soil” hypothesis suggests that metastatic potential depends on the compatibility between tumour cells (the “seed”) and the target organ microenvironment (the “soil”) [6]. The epithelial-to-mesenchymal transition (EMT) model posits that tumour cells acquire migratory and invasive properties through a transient mesenchymal state, later reverting to an epithelial phenotype to colonise new sites [7,8].
An alternative and increasingly supported hypothesis is the cancer–cell fusion theory, first proposed by Otto Aichel in 1911 [5,9]. This model proposes that metastasis may be driven by tumour hybrid cells (THCs), which are heterogeneous cells formed through the fusion of tumour cells with leukocytes, particularly monocytes or macrophages [9,10]. It has been demonstrated that THCs retain essential leukocyte properties such as migration, chemotaxis, and immune evasion, while preserving the proliferative capacity of tumour cells [11]. Experimental evidence supports this hypothesis: THCs have been detected in both primary tumours and peripheral blood [12], and exhibit enhanced migratory and proliferative capacities compared with their parental cells [13]. Transcriptomic studies further suggest that these hybrids overexpress genes involved in motility, immune escape and metabolic adaptation [13]. Collectively, these findings position THCs as both a potential mechanistic driver of metastasis and a promising biomarker for early dissemination and prognosis [5].
In parallel, the immune system plays a decisive role in tumour evolution, and immune checkpoints (ICs) have emerged as key regulators of immune surveillance [14]. Among the sICs analysed in this study, several exert non-redundant roles in the regulation of T-cell activation and immune tolerance. One such element is CD25, which corresponds to the α-chain of the Interleukin (IL)-2 receptor (IL-2rα). This IC is expressed by activated T cells and regulatory T cells, where it governs IL-2-dependent proliferation and immune tolerance [15,16]. In contrast, PD-L1, LAG-3, TIM-3 and CTLA-4 function as co-inhibitory ICs that restrain T-cell activation through complementary mechanisms, including the inhibition of T-cell receptor and co-stimulatory signalling, the promotion of T-cell dysfunction and immune exhaustion, and the maintenance of peripheral tolerance [14,16]. Tumours frequently exploit co-inhibitory pathways, most notably the PD-L1/PD-1 and CTLA-4 axes, to evade immune detection [17]. Although immune checkpoint blockade (ICB) therapy has revolutionised cancer therapy, eliciting durable responses in certain patients, its efficacy remains limited by resistance mechanisms, heterogeneity in checkpoint expression, immune exhaustion, and the absence of robust predictive biomarkers [18].
Given these challenges, the combined parallel study of tumour hybrid cells and soluble immune checkpoints may offer complementary insights into the intertwined mechanisms of metastasis and immune escape. While THCs may facilitate metastatic spread, sICs can reflect systemic immune dysregulation that promotes tumour persistence [5,14]. The integration of these two biological dimensions could therefore enable the identification of circulating biomarkers with both prognostic and stratification values in lung cancer. Despite the modest sample size and lack of an independent validation cohort, this study underscores the potential of uniting cellular and soluble immune biomarkers to advance our understanding of lung cancer progression and inform precision clinical management.
2. Results
2.1. Description of the Lung Cancer Cohort
To access the prognostic value of soluble immune checkpoints (sICs) and circulating tumour hybrid cells (THCs) in lung cancer (LC), 31 patients were prospectively recruited at the Thoracic Surgery Department of La Paz University Hospital (Madrid, Spain) between 11 March 2020 and 14 April 2023. Circulating THCs and twelve sICs were quantified. Patients were categorised according to key clinical parameters, including tumour histology, anatomical site, TNM classification, disease stage, relapse or progression status, metastatic involvement, prior cancer history, lymphovascular invasion, surgical approach, smoking status, and the presence of comorbid respiratory disease. Most patients were diagnosed at stage I disease, while a minority presented with stage III–IV. The single-stage IV patient underwent surgical intervention for diagnostic purposes, as prior less-invasive procedures had not yielded a definitive histopathological diagnosis. During the 2.5-year follow-up period, five patients experienced relapse or disease progression. Of these, one case had initially been classified as stage I, one as stage II, two as stage III, and one as stage IV disease. Two of these patients (one stage III and one stage IV) died during the follow-up period. Demographic and clinical characteristics of the cohort are summarised in Table 1.
Unsupervised data analysis based exclusively on circulating THCs and sICs levels, with no demographic or clinicopathological variables included, identified two distinct clusters of LC patients (Figure 1A). To facilitate interpretation of cluster formation, the relative relevance of the individual variables contributing to each cluster, as determined by Graphext, is shown in Figure 1B. This analysis revealed differential contributions of soluble immune checkpoint markers between clusters. sPD-1 showed greater relevance in Cluster 2, while sPD-L2 exhibited markedly higher relevance in defining Cluster 1 (Figure 1B). To further support this clustering, correlation mapping across all variables further revealed two coherent groups of immunomodulatory factors (Figure 1C), suggesting shared regulatory or functional relationships. Notably, sCD25, sCD86, and sTIM-3 showed strong positive correlations, forming a tightly correlated immunomodulatory module, whereas sCTLA-4, sPD-L1, and sLAG-3 grouped within an opposing correlation module (Figure 1C).
2.2. Immune Profiling Identifies a Four-Parameter Model Associated with Metastatic Progression in Lung Cancer
Using the same patient clustering obtained in Figure 1A, metastatic status was overlaid to evaluate their distribution across clusters; however, this unsupervised framework did not discriminate metastatic from non-metastatic patients (Figure 2A). Survival analyses were restricted to a 2.5-year follow-up period, as all observed deaths occurred within this interval. Among metastatic cases, the single individual located within Cluster 1 exhibited clinical and demographic features comparable to the remaining metastatic patients, except for a greater burden of pre-existing pulmonary disease, including COPD, obstructive sleep apnoea, and prior pulmonary thromboembolism. No additional distinguishing clinical variables were identified.
Direct comparison between metastatic and non-metastatic groups revealed significantly higher THC counts in metastatic patients (Figure 2B). Among soluble markers, levels of sPD-L1 and sLAG-3 were markedly increased in the metastatic subgroup (Figure 2C,D). Conversely, sTIM-3 concentrations were significantly lower in metastatic patients (Figure 2E). No significant differences were detected for s4-1BB, sCD25, sCTLA-4, Galectin-9, sCD27, sPD-1, sPD-L2, sSIGLEC5 or sCD86 (Supplementary Figure S1).
To further assess the prognostic value of these parameters for metastatic progression, variables with a receiver operating characteristic (ROC) area under the curve (AUC) above 0.7 were included in a binary logistic regression model with backward stepwise selection. This included statistically significant parameters (Figure 2B–E), as well as variables with an AUC value above 0.7 that did reach statistical significance (Supplementary Figure S1A–D). These variables were considered for their potential to improve the performance of the multivariate model (Supplementary Figure S1A–C).
After iterative removal of non-informative predictors, the final model retained five —THC count, CTLA-4, s4-1BB, sTIM-3, and sLAG-3— as the optimal predictors of metastasis. The resulting composite score demonstrated potential discriminatory power, with an optimal cut-off value of −8.399 (Youden index) and an AUC of 0.70 (95% CI: 0.4528–0.9427; p > 0.05; Figure 2F) with a sensitivity of 80.77% and a specificity of 60% at this threshold. Kaplan–Meier survival analysis confirmed that higher immune scores were significantly associated with reduced metastasis-free survival (Figure 2G). Furthermore, a UMAP projection that used only the variables that made up the composite score showed two distinct patient groups, with metastatic patients appearing more closely distributed than in the initial unsupervised model (Figure 2H). Notably, the outlier in this model did not correspond to that observed in Figure 2A, and no consistent clinical or demographic features distinguished the clusters generated.
2.3. Predictive Modelling of Survival Based on Circulating and Soluble Immune Markers
To explore the prognostic relationship between the circulating THCs, soluble markers, and overall survival, patients were monitored for up to 2.5 years of follow-up. The same analytical strategy was applied. As observed for the metastatic subgroups, unsupervised clustering did not differentiate alive (n = 28) from exitus (n = 5), and no clinical or demographic characteristics distinguished non-survivor individuals assigned to the different clusters (Figure 3A).
Comparative analysis revealed that sPD-L1 and sLAG-3 levels were significantly elevated in the individuals who deceased (Figure 3B,C). THC counts, sTIM-3, and sCD25 approached statistical significance (Supplementary Figure S2A–C), with THC counts showing a trend towards higher values in exitus, whereas sTIM-3 and sCD25 tended to be higher in the alive. No significant differences were observed for sCTLA-4, sSIGLEC5, sCD86, sPD-L2, sCD27, sPD-1, Galectin-9 and s4-1BB (Supplementary Figure S2D–K).
Variables exhibiting an AUC above 0.7 were included in a binary logistic regression model with backward stepwise selection to identify predictors of survival. The final model incorporated three key parameters—THC count, sLAG-3 and sTIM-3— which collectively defined a survival-associated immune profile (Figure 3D). ROC analysis confirmed the robustness of this model, yielding an AUC of 0.8692 (95% CI: 0.7342–1.0000; p < 0.01 **; Figure 3D). The optimal cut-off value, determined by the Youden index, was −1.421, with a sensitivity of 69.23% and a specificity of 100% at this threshold.
Kaplan–Meier analysis demonstrated that patients with higher composite (exitus) score had significantly reduced 2.5 year-survival (Figure 3E). UMAP clustering based on this composite score produced three distinct clusters that closely grouped non-survivors in the embedding space (Figure 3F).
3. Discussion
Despite considerable therapeutic advances, lung cancer (LC) remains associated with poor prognosis, largely due to delayed diagnosis, early metastatic dissemination, and therapeutic resistance [19,20]. The introduction of immunotherapy with immune checkpoint inhibitors (ICIs) has improved survival in selected patients; however, a substantial proportion derive limited or no clinical benefit, underscoring the urgent need for robust prognostic biomarkers capable of capturing tumour aggressiveness and immune escape beyond conventional staging and histopathology [21,22].
The primary objective of this study was to investigate whether circulating immune-related biomarkers, specifically soluble immune checkpoints (sICs) and tumour hybrid cells (THCs), could provide prognostic information in lung cancer. Patients were stratified according to metastatic progression and survival over a 2.5-year follow-up period, enabling the identification of biomarkers associated with both disease dissemination and clinical outcome.
The PD-1/PD-L1 axis represents a central mechanism of tumour-mediated immune evasion [23]. PD-1, also known as CD279, is an inhibitory receptor expressed on activated T cells, B cells, Natural Killer (NK) cells and antigen-presenting cells (APCs), where it limits immune activation [24]. Its ligand, PD-L1 (B7-H1), is induced under inflammatory conditions and is frequently upregulated on tumour cells, allowing them to suppress antitumour T-cell activity through PD-1 engagement [25]. This interaction has been shown to inhibit T-cell proliferation, cytokine release and cytotoxic function, thereby promoting an immunosuppressive microenvironment that favours tumour progression [26]. In lung cancer, PD-L1 expression has been correlated with advanced disease stages, smoking history, and a poor prognosis for patients [27]. In our cohort, soluble PD-L1 (sPD-L1) levels were significantly higher in patients with metastatic disease and in non-survivors. These findings support the notion that circulating PD-L1 reflects a systemic immunosuppressive state associated with aggressive tumour biology. Importantly, the heterogeneous clinical response to PD-1/PD-L1 blockade highlights the limitations of relying on a single immune checkpoint as a prognostic or predictive marker [28,29], reinforcing the value of multiplex immune profiling.
Similarly, soluble LAG-3 (sLAG-3) was markedly increased in metastatic patients and non-survivors. LAG-3 is a key inhibitory receptor expressed on activated T cells and plasmacytoid dendritic cells, where it promotes T-cell exhaustion and immune suppression through engagement with ligands such as FGL1 and Galectin-3 [30,31,32]. Previous studies have reported LAG-3–positive tumour-infiltrating lymphocytes in both NSCLC and SCLC, often correlating with aggressive tumour features and poor outcome [33,34]. Moreover, lung adenocarcinoma patients with higher numbers of LAG-3^+^ positive cells correlated with features of aggressive tumour characteristics [35]. Our findings extend these observations to the systemic level, suggesting that sLAG-3 may serve as a circulating marker of advanced immune dysfunction [31,36].
In contrast to sPD-L1 and sLAG-3, soluble TIM-3 (sTIM-3) was elevated in non-metastatic patients and alive individuals, indicating a distinct immunological role. TIM-3 is expressed across multiple immune compartments and participates in both immune activation and regulation depending on disease stage [37,38,39,40]. Notably, recent spatial and single-cell analyses have shown TIM-3 enrichment in early lung adenocarcinoma lesions, suggesting a role in initial immune modulation rather than terminal exhaustion [41]. This contrasts with the case of advanced tumours, where membrane-bound TIM-3 on TILs has been found to correlate with metastasis and poor survival [42,43]. This is consistent with our observation that higher sTIM-3 levels predominated in early-stage, non-metastatic survivors. Together, these findings highlight that the prognostic value of immune checkpoints is context-dependent and stage-specific.
Importantly, soluble immune checkpoints are not merely passive biomarkers: they retain biological activity and can actively modulate immune signalling by engaging cognate receptors and ligands [32,39]. Within this context, CTLA-4 represents a central regulator of early T-cell activation, acting upstream of PD-1–mediated inhibition by limiting CD28-dependent co-stimulatory signalling. Consistent with its role in the regulation of early T-cell activation, CTLA-4 has been established as a clinically relevant therapeutic target for immune checkpoint blockade, including in lung cancer [44,45].
Beyond immune checkpoints, a major strength of this study is the integration of tumour hybrid cells (THCs) into the prognostic framework. We demonstrate that circulating THCs are significantly increased in patients with metastatic disease and in non-survivors, strongly implicating these cells in aggressive clinical behaviour. THCs arise through tumour–leukocyte fusion, a process that confers both malignant traits (genomic instability, proliferative capacity) and leukocyte-derived properties such as enhanced motility, immune evasion, and tissue tropism [5,46,47]. This hybrid phenotype provides a compelling biological explanation for their heightened invasive and metastatic potential.
Consistent with our findings, fusion-derived hybrid cells have been reported in multiple malignancies, including melanoma, colorectal cancer, and breast cancer, where their presence correlates with metastatic spread and poor survival [48,49,50]. Importantly, THCs have been shown to upregulate immune checkpoints such as PD-L1, SIGLEC5 and CTLA-4, further facilitating immune escape [49,51,52,53]. The concurrent increase in THCs and immunosuppressive sICs observed in our cohort suggests a relationship between tumour dissemination capacity and systemic immune suppression.
Taken together, our data indicate that THCs and sICs capture two complementary dimensions of tumour progression. THCs reflect the tumour’s intrinsic ability to disseminate physically, while sICs could mirror a permissive immunological environment that enables metastatic outgrowth. Their co-detection may therefore define a “pro-metastatic state”, characterised by both enhanced migratory competence and impaired immune surveillance.
Although this study is limited by a relatively small cohort size, this limitation is mitigated by the depth of immune profiling and the longitudinal clinical follow-up. The consistency of associations across metastatic status and survival outcomes strengthens the robustness of our conclusions. Importantly, both THCs and sICs can be quantified from peripheral blood, highlighting their potential as minimally invasive biomarkers suitable for repeated monitoring.
From a translational perspective, the integration of THCs and sICs could support personalised medicine by identifying patients at higher risk of early metastasis or poor survival who may benefit from intensified surveillance, combination immunotherapies, or early systemic intervention. Future studies should focus on validating these findings in larger, independent cohorts, integrating THC and sIC profiling with tumour genomics, immune infiltration patterns, and treatment response. Phenotypic and functional characterisation of THCs, alongside longitudinal immune monitoring, will be essential to establish their clinical utility.
4. Materials and Methods
4.1. Participant Recruitment and Eligibility Criteria
Peripheral blood samples were obtained from patients with lung cancer (LC, n = 31) recruited at the Thoracic Surgery Service of La Paz University Hospital (Madrid, Spain) prior to surgery. All patients had a histologically confirmed diagnosis of LC prior to enrolment, were evaluated in the outpatient clinic, and subsequently reviewed by the hospital’s multidisciplinary Lung Tumour Committee.
The inclusion criteria were based on a histopathological diagnosis of primary non-small cell lung cancer (specifically adenocarcinoma and squamous cell carcinoma) in patients requiring diagnostic or therapeutic surgical intervention by the Thoracic Surgery Department at University Hospital La Paz. Furthermore, eligible participants were required to have provided written informed consent for both biobank storage and the collection of peripheral blood samples during routine follow-up prior to surgery.
Patients were excluded from the study if they presented with benign lesions, secondary lung metastases, or pulmonary neuroendocrine tumours. Furthermore, exclusion was applied to patients whose clinical status, such as those in palliative care or elderly patients with mobility issues, prevented sample collection without exceeding the standard of care. Finally, patients receiving postoperative follow-up at external healthcare facilities were excluded to prevent redundant clinical visits and unnecessary blood draws.
Blood samples were collected and processed within 24 h prior to surgical intervention. Detailed clinical and demographic information for this cohort is provided in Table 1.
4.2. Clinical Definitions
The following clinical definitions were applied to ensure consistent classification of disease status and outcomes throughout the study.
Metastasis was defined as the dissemination of neoplastic cells to organs different from the primary tumour site, as confirmed by clinical and radiological assessment, during follow-up (e.g., lymph nodes, bone, contralateral lung, or other distant organs). Relapse was defined as the reappearance of neoplastic disease after a documented period of clinical, radiological, and/or analytical remission following initial treatment (surgery, chemotherapy, radiotherapy and/or immunotherapy). The progression of the disease was defined as a deterioration in the patient’s condition during the follow-up period, as evidenced by the enlargement of existing tumours and/or the emergence of new metastatic lesions, in the absence of a prior interval without disease. The term “exitus” was defined as death from any cause during the follow-up period.
4.3. Plasma Collection
Plasma was isolated from EDTA-anticoagulated venous blood either by density gradient centrifugation using Ficoll-Plus solution (GE Healthcare BioSciences, Uppsala, Sweden) or by centrifugation at 3000 rpm for 15 min. The plasma fraction was aliquoted and stored at −80 °C until analysis. Prior to use, samples were thawed at 4 °C and clarified by centrifugation at 15,000× g for 10 min to remove residual cellular debris.
4.4. Detection of Soluble Immune Checkpoints
Plasma concentrations of soluble immune checkpoints (sICs) were quantified using the LegendPlex™ (BioLegend, San Diego, CA, USA, catalogue number 740867) following the manufacturer’s instructions. The panel 1 included: sCD25, s4-1BB, sCD27, sCD86, TGF-β1 (free active form), sCTLA-4, sPD-L1, sPD-L2, sPD-1, sTIM-3, sLAG-3, and Galectin-9. Prepared samples were acquired on a FACS Calibur flow cytometer (BD Biosciences, Franklin Lakes, NJ, USA), and data were analysed using LegendPlex software (v.8, BioLegend, San Diego, CA, USA).
4.5. Enzyme-Linked Immunosorbent Assay (ELISA)
Soluble SIGLEC5 levels in plasma were measured using a Human SIGLEC5 ELISA kit (Invitrogen, Carslbad, CA, USA, Cat No. EHSIGLEC5) in accordance with the manufacturer’s protocol. Absorbance was read at 450 nm using an Epoch™ microplate reader (BioTek, Instruments, Winooski, VT, USA).
4.6. Sample Processing and Full-Spectrum Flow Cytometry
Whole blood samples were collected in EDTA (ethylenediaminetetraacetic acid anticoag-ulated) tubes (Vacuette^®^, Greiner Bio One, Kremsmünster, Austria). Red blood cell lysis was performed using BD PharmLyse™ Lysing Buffer (BD Biosciences, Franklin Lakes, NJ, USA), yielding a leuko-cyte cell suspension, which was washed twice with phosphate-buffered saline (PBS). Cell viability was assessed using LIVE/DEAD™ Fixable Blue dye (Invitrogen, Carslbad, CA, USA). Subsequently, cells were incubated with an antibody panel detailed in Supplementary Table S1. The staining panel was designed to measure circulating tumour hybrid cells, gated as the CD14+ population expressing EpCAM+ and CD45+ and non-expressing CD3^−^, CD56^−^, CD16^−^, CD19^-^ and CD1c^−^, as shown in Supplementary Figure S3.
4.7. Statistical Analysis and Bioinformatic Processing
All statistical analyses and graphical representation were performed using GraphPad Prism 10.3.1 (GraphPad Software, Inc., San Diego, CA, USA). Outliers were identified and excluded using the ROUT method (Q = 1%). Data normality was assessed by the Shapiro–Wilk test. Results are presented as violin plots displaying median values and interquartile ranges (IQRs). For two-group comparisons, the Mann–Whitney U test was used in non-parametric data, and the unpaired t-test was applied for parametric data.
Binary logistic regression models were constructed using the backward Wald method with IBM SPSS Statistics v.23 software (IBM Corp, Armonk, NY, USA). This stepwise approach begins with the full set of candidate independent variables and repeatedly removes them based on their statistical significance. For each variable included in the final model, a corresponding coefficient (B-factor) was calculated to reflect its impact on the differentiation between groups. The final scores were obtained using the following formula: Score = ([Parameter A] × B-factor A) + ([Parameter B] × B-factor B) + … + ([Parameter X] × B-factor X), as previously described [54,55]. Classifying scores were used to construct receiver operating characteristic (ROC) curves, where the area under the curve (AUC) and optimal cut-off values were obtained as the Youden index. The objective of selecting the most appropriate regression model was to identify a minimal number of variables while ensuring the retention of those exhibiting the greatest statistical significance.
Kaplan–Meier survival analyses were performed using Microsoft Office Excel and Kaplan–Meier Plotter web page (version 2025.06.16). For unsupervised data exploration, including Uniform Manifold Approximation and Projection (UMAP) visualisation and hierarchical clustering, Graphext (Madrid, Spain) was employed. Parameters were set as follows: Euclidean metrics, n_neighbours = 30, 127 n_components = 10 and min_dist = 0.01. The number of clusters was automatically determined by the algorithm based on variable strength.
Statistical significance was defined as follows: p > 0.05, not significant (ns); *, p < 0.05; **, p < 0.01; ***, p < 0.001; and ****, p < 0.0001.
5. Conclusions
This study provides evidence that the combined assessment of circulating tumour hybrid cells and soluble immune checkpoints offers a powerful, minimally invasive approach to prognostic stratification in lung cancer. By capturing both tumour plasticity and immune suppression, this dual biomarker strategy opens new avenues for understanding metastatic progression and tailoring precision oncology strategies.
6. Clinical Implications
The identification of circulating THCs and sICs as complementary prognostic biomarkers has direct clinical relevance for the management of lung cancer. As both parameters can be quantified from peripheral blood, they offer a minimally invasive approach to risk stratification that may complement conventional staging and tissue-based biomarkers. The co-detection of elevated THCs and immunosuppressive sICs could identify patients in a pro-metastatic state, characterised by enhanced tumour dissemination and impaired immune surveillance, who may benefit from closer clinical monitoring, early systemic intervention, or combination immunotherapeutic strategies. Moreover, integrating THC and sIC profiling into longitudinal patient follow-up may enable dynamic assessment of disease evolution and treatment response, supporting more personalised and adaptive therapeutic decision-making in lung cancer care.
7. Limitations of the Study
It is important to note that the present study is subject to certain limitations, which must be considered when interpreting the results. The cohort size was modest, with 31 patients included, which limits statistical power and may increase the risk of overfitting in the predictive models, particularly in complex models such as those applied in this study. Moreover, the single-centre design restricts the generalisability of the findings, as population characteristics, clinical management, and laboratory conditions may differ across institutions. Another important limitation is the absence of an independent validation cohort, meaning the logistic regression models should be regarded as exploratory and require external confirmation in larger, multicentre datasets. The heterogeneity of tumour histology, clinical stages, comorbidities and treatments within the cohort introduces biological variability that may influence both THC counts and sIC levels, although this reflects real-world clinical practice. Furthermore, all biomarkers were measured at a single pre-surgical time point, thereby preventing the analysis of temporal dynamics or treatment-related changes in THC or sIC profiles. In addition, the cellular sources of the analysed sIC were not characterised, which limits the interpretation of the mechanisms involved, since these circulating factors may originate from multiple tumour and immune cell compartments. Consequently, further mechanistic work is required to elucidate the biological pathways connecting tumour–immune fusion events with systemic immune dysregulation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhou J. Xu Y. Liu J. Feng L. Yu J. Chen D. Global Burden of Lung Cancer in 2022 and Projections to 2050: Incidence and Mortality Estimates from GLOBOCAN Cancer Epidemiol.20249310269310.1016/j.canep.2024.10269339536404 · doi ↗ · pubmed ↗
- 2World Cancer Research—Lung Cancer Available online: https://www.wcrf.org/preventing-cancer/cancer-types/lung-cancer/#what-causes-lung-cancer(accessed on 24 November 2025)
- 3González J. de Castro F. Barrueco M. Cordovilla R. Fernández J. Gómez F. Moreno de Vega B. Ramos J. Serrano A. Delays in the Diagnosis of Lung Cancer Arch. Bronconeumol.20033943744110.1016/S 0300-2896(03)75425-814533992 · doi ↗ · pubmed ↗
- 4Fares J. Fares M.Y. Khachfe H.H. Salhab H.A. Fares Y. Molecular Principles of Metastasis: A Hallmark of Cancer Revisited Signal Transduct. Target. Ther.202052810.1038/s 41392-020-0134-x 32296047 PMC 7067809 · doi ↗ · pubmed ↗
- 5López-Collazo E. Hurtado-Navarro L. Cell Fusion as a Driver of Metastasis: Re-Evaluating an Old Hypothesis in the Age of Cancer Heterogeneity Front. Immunol.202516152478110.3389/fimmu.2025.152478139967663 PMC 11832717 · doi ↗ · pubmed ↗
- 6Akhtar M. Haider A. Rashid S. Al-Nabet A.D.M.H. Paget’s “Seed and Soil” Theory of Cancer Metastasis: An Idea Whose Time Has Come Adv. Anat. Pathol.201926697410.1097/PAP.000000000000021930339548 · doi ↗ · pubmed ↗
- 7Pastushenko I. Brisebarre A. Sifrim A. Fioramonti M. Revenco T. Boumahdi S. Van Keymeulen A. Brown D. Moers V. Lemaire S. Identification of the Tumour Transition States Occurring during EMT Nature 201855646346810.1038/s 41586-018-0040-329670281 · doi ↗ · pubmed ↗
- 8Diepenbruck M. Christofori G. Epithelial-Mesenchymal Transition (EMT) and Metastasis: Yes, No, Maybe?Curr. Opin. Cell Biol.20164371310.1016/j.ceb.2016.06.00227371787 · doi ↗ · pubmed ↗