Household and Environmental Determinants Influencing Atopic Dermatitis Among Young Rural Children in the Ehlanzeni District Municipality
Thokozani P. Mbonane

TL;DR
This study explores how household and environmental factors influence atopic dermatitis in young children in rural South Africa, highlighting the need for better healthcare access and environmental interventions.
Contribution
The study identifies specific rural-specific risk factors for atopic dermatitis, such as second-hand smoke and traditional utensils, in a context with limited prior research.
Findings
The prevalence of atopic dermatitis in rural areas is high, with current AD affecting 18.62% of children.
Exposure to household tobacco smoke and use of traditional brooms are linked to increased AD risk.
Natural birth is a protective factor against both historical and current AD.
Abstract
Public health relevance—How does this work relate to a public health issue? Atopic dermatitis (AD) remains a prevalent condition among young children in both urban and rural settings.Access to primary health services for the management of atopic dermatitis is constrained in rural regions. Atopic dermatitis (AD) remains a prevalent condition among young children in both urban and rural settings. Access to primary health services for the management of atopic dermatitis is constrained in rural regions. Public health significance—Why is this work of significance to public health? The prevalence of atopic dermatitis in rural areas is comparable to that observed in urban areas, where there is a greater volume of research conducted.Exposure to second-hand smoke within the household environment serves as a trigger for atopic dermatitis in rural populations.The use of traditional, homemade…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
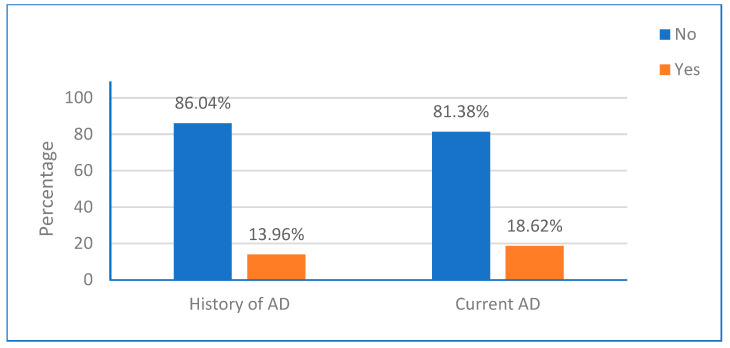 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatology and Skin Diseases · Asthma and respiratory diseases · Allergic Rhinitis and Sensitization
1. Introduction
Atopic dermatitis (AD) is a common multifactorial chronic skin disease that is influenced by environmental determinants. It affects a significant number of young children worldwide [1,2]. Studies estimate that 15–20% of children globally experience AD each year [3]. In sub-Saharan countries, the prevalence of AD in children ranges from 4.7% to 23% [4]. Scientific evidence suggests that children in urban areas have a higher risk of developing AD compared to those in rural areas [5]. However, there are limited studies conducted in sub-Saharan regions that reported the prevalence of AD among young rural children [6]. It is important to note that children in rural areas may have limited access to healthcare services, including those for skin conditions, due to the shortage or absence of primary healthcare facilities [7,8]. While genetic predisposition plays a role in AD, household and environmental determinants also contribute significantly to the development of this condition [9,10,11].
Current evidence shows that AD can be triggered by numerous individual, genetic, and household (home environment) determinants [12]. Family history of AD, personal hygiene products, sex (male children were at high risk), child diet, food allergies, and history of eczema, allergies, hay fever, or asthma have been linked to AD in different environments [13,14]. Furthermore, AD has been associated with season of birth, method of birth, breastfeeding duration, number of siblings, and ordinal position [15,16,17,18]. A few studies have shown that home/residential determinants such as indoor pet ownership, and household income, play a role in triggering AD.
Numerous environmental determinants contribute or trigger the development of AD among children [10]. These determinants included climatological determinants, air pollution and related activities, house dampness, mold in the walls, and residing near bushes or green areas [19]. A recent analytical cross-sectional study in an urban area conducted among schoolchildren 7 years or younger showed that current AD was positively associated with household environmental tobacco smoke (ETS) exposure, fuel use for cooking and heating, use of building materials (renovation), house with new indoor painting and new furniture, broom stick, indoor dust, and frequency of trucks transit through the neighboring streets [20].
In recent years, several studies have indicated that AD is more common among urban children compared to those living in rural areas [6,21,22]. A community-based study conducted in China discovered that the prevalence of AD was higher in urban areas (10.2%) as opposed to rural areas (4.6%) [22]. However, many of the residential and environmental determinants associated with AD are linked to poor socio-economic conditions, which are often prevalent in rural communities. Therefore, the researcher hypothesized that children living in rural areas might be exposed to household and environmental determinants linked to atopic determinants. The objectives of the study were: (i) to describe the prevalence of AD among rural young children; (ii) to identify household and environmental determinants; and (iii) to assess the determinants that influence the prevalence of AD among young rural children from Louisville, Mpumalanga Province, South Africa.
2. Materials and Methods
2.1. Study Design and Setting
A cross-sectional analytical study was conducted between August 2021 and September 2023. The study was conducted in a rural residential area (Louisville) of Barberton town in Mpumalanga Province, South Africa. The area is situated near the Lily gold mine and is surrounded by agricultural activities. The main gravel road to access the farms and mine is in this residential area.
2.2. Population and Sampling
The study sample consisted of caregivers/mothers and their children residing in a rural residential area. The children were between the ages of 5 and 13, and it was required that the child had resided in the area with their parents/guardian from the age of 12 months old or younger. Children who were born outside the study site were excluded from the study, and child-headed households were not considered. Those who were approached and agreed to participate were enrolled in the study. Participants were enrolled in the study using convenience sampling (chosen to ensure direct access to identified potential participants residing near illegal mining activities); families with children were identified beforehand with the support of the local Ward-based outreach teams (WBOTs), and the research teams visited those households. The WBOTs are government structures that are linked to a local health care facility and are responsible for conducting “community, household, and individual-level health assessments”. These teams normally included community health workers led by a nurse. A register of the visited households was kept during data collection to ensure that there was no duplication or visiting of the same households.
To determine the sample size for the study, the following Formula (1) was used. In this formula, “n” represents the sample size, “Z” is the Z-value corresponding to a 95% confidence level (1.96), “p” is the estimated sample proportion (0.5), and “e” is the margin of error, which was set at 0.05. Thus, the estimated population for the study was 384.
2.3. Data Collection
The data was collected in three different timeframes: August 2021, September 2022, and September 2023. Household identification numbers (local stand numbers) were recorded to prevent visiting the same households multiple times. The data were collected using an adapted and modified International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire (see Supplementary File S1) [23,24,25,26]. The questionnaire has been used in South African studies and elsewhere [20,27,28]. Trained research assistants (fourth-year environmental health students) administered the questionnaire and interviewed mothers/caregivers. During data collection, the research assistants were paired (one research assistant needed to be conversant with either isiSwati or siTsonga). The questionnaire was translated into isiSwati and siTsonga, the two most common languages in Louisville, before data collection and the responses were translated back to English by two professional linguists. The questionnaire was divided into socio-demographics (participant characteristics), study health outcome, and household, dietary, and environmental determinants. The questions on determinants were based on the scientific literature and previous studies in a similar population [10,21,22,29,30,31,32,33,34,35,36,37].
Socio-demographic data included: the mother/caregiver’s educational level (no schooling/primary school/high school), income sources (government social grants/self-employed/salary), income level measured in South African Rands (ZAR) with the 14.6206 = 1 United States Dollars (USD) exchange rate at the time of data collection (equal or less than ZAR 2500/ZAR 2501–ZAR 7500/Above ZAR 7500), child sex (male/female), age (7 years old or younger/8–10 years old/11–13 years old), childbirth method (caesarian/natural birth), the ordinal position of the child (firstborn/middle/lastborn), preschool (remote/local), food allergy (no/yes), and history of AD in the family (no/yes).
2.3.1. Study Health Outcomes
The study’s health outcome variables were based on previous scientific literature and studies conducted in similar areas and aligned to the ISAAC criteria for screening for AD [20,27]. History of AD was determined by the positive (yes) to the following question by the mother/caregiver: Has the child had AD at any time before the last six months? The current AD diagnosis was determined by asking the mothers/guardians the following: (i) has the child experienced a persistent dry and itchy rash, (ii) a rash with inflamed skin, and (iii) persistent dry and itchy rash and inflamed skin in the past 6 months.
2.3.2. Household and Dietary Determinants
Household and dietary determinants of AD included were as follows: having an indoor domestic cat (yes/no), having an outdoor domestic dog (yes/no), using chemicals for cleaning (occasional/every day), using a traditional broom for sweeping the floor (yes/no), having an old mat or rag at home (yes/no), consuming house milked dairy products (yes/no), consuming household hatched eggs and homegrown vegetables and fruits (yes/no), frequency of dietary intake by the child of eggs, homegrown vegetables and fruits and peanuts (seldom/sometimes/regularly), and buying (or replacing) new furniture during the mother’s pregnant period, or when the child was younger than 12 months of age (yes/no).
2.3.3. Environmental Determinants
Environmental determinants were as follows: exposure to environmental tobacco smoking at home (yes/no), location of the household street (back street/away from the busy main road)/main street), house surrounding (bushes/no bushes), cooking and heating fuel (electricity/paraffin/coal), dampness on the inside of the house (yes/no), stagnant water within walking distance of the home (yes/no) and house, any house renovations during the mother’s pregnancy or while the child was younger than 12 months (yes/no).
2.4. Data Analysis
The data was analyzed using Stata MP software (version 18). Tables and figures were used to present the findings regarding frequency and percentages. Fischer’s exact test was employed to determine statistically significant differences between variables. The association between the prevalence of AD and socio-demographic variables and household and environmental determinants was examined. Initially, a bivariate regression analysis was conducted, and the variables that demonstrated a statistically significant association (p-value of 0.05 or less) with the prevalence of AD were reported as an unadjusted odds ratio (UOR). The final model consisted of a multivariate automated stepwise backwards regression analysis (all the determinants were included in the final model), utilizing statistical variables where a p-value of 0.05 or lower was considered statistically significant and reported as an adjusted odds ratio (AOR).
2.5. Ethical Approval and Consent to Participate
The study obtained ethical clearance from the University of Johannesburg, Faculty of Health Sciences Research Ethics Committee (REC-01-11-2019). Parents and mothers/caregivers gave their informed consent before data collection.
3. Results
3.1. Characteristics of the Study Participants
Most of the mothers/caregivers had a high school educational level (n = 360, 41.32%), were dependent on government social grants for survival as the source of income (n = 314, 35.64%), and 443 (50.28%) were living on ZAR 2500 or less per month. This study had more boys (n = 477, 54.14%) than girls (n = 404, 45.86%). Most of the study participants were between the ages of 6–8 (n = 332; 37.68%) and were naturally born (n = 709; 80.48%). Furthermore, most were either a middle child (n = 318; 36.10%) or a lastborn (n = 300; 34.05%) in their family structure (position). There were 275 (31.21%) study participants who lived with someone who was dependent on a government social grant for the source of income. Lastly, 452 (51.31%) lived with a mother who is a smoker. Table 1 shows a detailed description of the characteristics of the study participants.
3.2. Prevalence of Current AD and History of AD
In the study, 123 children (13.96%) had previously experienced AD. Additionally, 164 children (18.62%) had experienced AD in the past six months, as shown in Figure 1.
3.3. Household Determinants of Atopic Dermatitis in the Study
Table 2 shows the distribution of history and current atopic dermatitis (AD) according to household determinants. Among children residing in households with cats, the reported cases of a history of AD were 17.07% (n = 21) out of 358 households that owned a cat, while 55 children (44.72%) with a reported history of AD lived in households with dogs as pets. Furthermore, the number of cases of children with a history of AD from households that used daily cleaning chemicals and traditional brooms were 48.78% (n = 60) and 92.68% (n = 114), respectively. Out of 459 households (52.10%) that owned old mats or rugs, 63 reported having children with a history of AD. The cases with a history of AD were high concerning specific dietary factors: 76.67% (n = 98) among those consuming household eggs, 79.67% (n = 98) among those eating homegrown vegetables and fruits, and 60.16% (n = 74) among those who regularly consumed peanuts. Comparative analysis between children with a history of AD and those without indicated statistically significant differences for the following categorical variables: cats (p = 0.001), cleaning chemicals (p < 0.001), traditional broom (p < 0.001), household eggs (p = 0.001), eggs (p = 0.001), and furniture (p < 0.001). There was a high number of current AD reported among children residing in households that utilize cleaning chemicals daily (n = 82; 50%), employ traditional brooms (n = 117; 71.34%), consume household-produced eggs (n = 132; 80.49%), and regularly consume homegrown vegetables and fruits (n = 132; 80.49%). Additionally, a significant proportion of these children reported regular consumption of peanuts (n = 102; 62.20%). Among children diagnosed with current AD, a statistically significant difference was observed when compared to those without current AD across several household and dietary factors: the presence of cats (p = 0.001), daily use of cleaning chemicals (p < 0.001), ownership and use of traditional grass brooms (p < 0.001), consumption of household eggs (p < 0.001), regular egg consumption (p < 0.001), intake of homegrown vegetables and fruits (p < 0.001), regular vegetable consumption (p = 0.010), regular peanut consumption (p = 0.025), and the presence of new furniture during pregnancy (p < 0.001), see Table 2.
3.4. Environmental Determinants of Atopic Dermatitis in the Study
Table 3 shows the descriptive analysis of environmental determinants according to and current cases of atopic dermatitis. There were children with AD in both history (n = 97, 75.78%) and current (n = 124, 96.88%) cases in households with environmental tobacco smoking exposure. There were more children with current AD (n = 77, 18.51%) who stayed in households surrounded by bushes when compared to those with a history of AD (n = 59, 14.18%). Most children with AD come from households that use coal for cooking and heating. In children with a history of AD, 14.86% (n = 70) and 13.80% (n = 93) used coal for cooking and heating, respectively. Of children with current AD, 86 (18.26%) and 121 (17.95%) were from households that use coal for cooking and heating, respectively. The analysis reveals a statistically significant difference between children with a history of atopic dermatitis (AD) and those without several environmental determinants. These determinants include exposure to environmental tobacco smoke (p = 0.001), house location (p = 0.001), type of cooking fuel used (p = 0.007), and residing in a house with renovations (p < 0.001). Additionally, significant differences were observed for environmental tobacco smoke exposure (p = 0.001), street location of the house (p = 0.001), cooking fuel type (p < 0.001), and the presence of renovations in the house (p < 0.001).
3.5. Determinants of Atopic Dermatitis in the Study
The bivariate analyses of determinants that were not associated with history and current atopic dermatitis are presented in the appendices (Table A1, Table A2, Table A3 and Table A4). While in Table 4 and Table 5 present the determinants that had an individual association with the health outcome in the study. In the bivariate analysis, history of AD had a significant association with using cleaning chemicals daily (p = 00.001), consuming household eggs (p = 0.001), recently changed or bought furniture (p = 0.001), the use of a childbirth method (p = 0.001), using a traditional broom (p = 0.001), ETS (p = 0.001), and house renovation (p = 0.001).
The bivariate analysis showed that current AD was significantly associated with having a pet cat (p = 0.001), using cleaning chemicals daily (p = 0.001), consuming household eggs (p = 0.001), consuming homegrown vegetables and fruits (p = 0.014), recently changed or bought furniture (p = 0.001), using a traditional broom (p = 0.001), ETS (p = 0.001), residing in house surrounded by bushes (p = 0.001), and house renovation (p = 0.001).
In the final multivariate analysis model (Table 4 and Table 5), being born through caesarean was a protective factor for both children with a history of AD (AOR: 0.094; p < 0.001) and current AD (AOR: 0.261, p < 0.001). While residing in a household that used a grass broom for cleaning the floor (AOR: 1.106, p < 0.001), ETS exposure (AOR: 1.141; p < 0.001), and renovated house (AOR: 4.020; p < 0.001) were determinants for history of AD. Similar current AD was associated with residing in a household that used a grass broom for cleaning the floor (AOR: 1.113; p < 0.001), ETS exposure (AOR: 1.721; <0.001), and renovated house (AOR: 3.998, p < 0.001). The multivariate analysis findings of determinants that had no significant association either with a history of or current AD in the study are presented in Appendix B.1 and Appendix B.2, respectively.
4. Discussion
The study aimed to elucidate the prevalence of AD, both and current, while also assessing determinants, particularly household, dietary, and environmental determinants, associated with the prevalence of AD within the population. The findings indicated the prevalence of both and current AD among the study population. The study revealed that the method of childbirth may significantly influence the development of atopic dermatitis [16,38,39], with natural birth identified as a protective factor. Furthermore, the study revealed a significant positive association between both history and current AD and the utilization of traditional brooms (shown in Figure 2) for floor cleaning, exposure to household environmental tobacco smoke, and experiences of home renovations. Additionally, it was found that the current AD was positively correlated with the presence of an indoor domestic cat. The prevalence of a history of and current atopic dermatitis among children aged 7 to 13 years in rural areas was found to be 13.96% and 18.62%, respectively. This study’s findings fall within the range of prevalence reported in studies conducted in urban areas of South Africa. This similarity may be attributed to the presence of industrial activities, such as agricultural practices and the now-defunct Lily gold mine, close to these rural communities. Previous research has suggested that industrial activities in urban settings may contribute to the onset and progression of atopic dermatitis [6].
Previous studies have reported the role of ETS and house renovation on the development of atopic dermatitis [20,30,40,41,42]. Recently, a South African study in an urban area has shown that there is a positive association between ETS and atopic dermatitis among preschool children aged 7 years [20]. This is similar to other South African studies and elsewhere among young children and adolescents [27,35,36,43,44,45]. The study was in line with previous studies; ETS was associated with history and current atopic dermatitis. The study also shows an association between house renovation during pregnancy or infancy with history and current atopic dermatitis. This finding is consistent with previous studies [19,30]. A cross-sectional study conducted among Chinese children aged 3–6 found that home renovation was a determinant for atopic dermatitis. Both findings are important for parental educational awareness for preventing environmental determinants of atopic dermatitis and similar conditions, especially during pregnancy and infancy.
The utilization of a grass broom to sweep the floor was positively associated with both history and current atopic dermatitis. One potential explanation for this association may be the presence of grass allergens originating from the broom itself, as previous research has indicated that grass pollen can trigger the development of atopic dermatitis [46,47]. Additionally, the broom may serve as a device that captures dust mites and other mites commonly found on the floor daily [48,49]. Nevertheless, further investigation is warranted to determine the underlying cause for the correlation between the use of a grass broom and atopic dermatitis.
The relationship between the childbirth method and the development of atopic dermatitis and other allergic conditions has been a subject of investigation. Although there is no conclusive worldwide evidence, several studies have suggested a potential link between cesarean birth and allergic conditions. For instance, a Swedish National Cohort study involving children aged 5 or younger found that those born by cesarean section were at a higher risk of developing atopic dermatitis in early childhood. These findings align with a Scandinavian cohort study by Hoel et al. in 2023 [38]. Conversely, a cohort study conducted in the United States did not find an association between cesarean section and atopic dermatitis [39]. Similarly, a prospective birth cohort study conducted in Greece also found no association between atopic dermatitis and cesarean-section birth [37]. Notably, the Greek study found that natural birth was a protective factor against atopic dermatitis, which supports the hypothesis that children born through cesarean sections are at risk of developing AD, and natural birth is a protective factor. This is also highlighted in the study findings, which indicate that natural birth is a protective factor. These findings could be valuable for maternal education and encourage expecting mothers to consider natural birth when it is safe, as part of primary prevention for childhood atopic dermatitis.
One of the study’s strengths was using the ISAAC questionnaire, which has been used globally and in local settings. There were two study limitations. The study determined the association using a cross-sectional study and does not show the cause–effect relationship between atopic dermatitis and determinants. Hence, the study recommends a longitudinal study in the same or a similar setting. Lastly, the study did not conduct a clinical diagnosis of atopic dermatitis among participants.
5. Conclusions
The study findings show a high prevalence of AD among children in rural areas. The study’s key findings on the determinants of AD, using traditional brooms for floor cleaning, exposure to household environmental tobacco smoke, and experiences of home renovations were found to influence AD in the study, while natural birth was a protective factor. Further investigation is warranted in rural areas regarding the occurrence of atopic dermatitis among children, as these areas often suffer from limited access to healthcare services. Consequently, there is a pressing need to implement environmental prevention programs aimed at safeguarding children residing in rural areas from the triggers of atopic dermatitis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nutten S. Atopic Dermatitis: Global Epidemiology and Risk Factors Ann. Nutr. Metab.20156681610.1159/00037022025925336 · doi ↗ · pubmed ↗
- 2Sasaki M. Yoshida K. Adachi Y. Furukawa M. Itazawa T. Odajima H. Saito H. Hide M. Akasawa A. Environmental factors associated with childhood eczema: Findings from a national web-based survey Allergol. Int.20166542042410.1016/j.alit.2016.03.00727134054 · doi ↗ · pubmed ↗
- 3Luschkova D. Zeiser K. Ludwig A. Traidl-Hoffmann C. Atopic eczema is an environmental disease Allergol. Select 2021524425010.5414/ALX 02258 E 34476334 PMC 8383845 · doi ↗ · pubmed ↗
- 4Sendrasoa F.A. Razafimaharo T.I. Ramarozatovo L.S. Rapelanoro Rabenja F. Quality of life in children with atopic dermatitis seen in the department of dermatology at the university hospital, Antananarivo Madagascar JAAD Int.202310575810.1016/j.jdin.2022.11.00436688103 PMC 9850171 · doi ↗ · pubmed ↗
- 5Schram M.E. Tedja A.M. Spijker R. Bos J.D. Williams H.C. Spuls P.h.I. Is there a rural/urban gradient in the prevalence of eczema? A systematic review Br. J. Dermatol.201016296497310.1111/j.1365-2133.2010.09689.x 20331459 · doi ↗ · pubmed ↗
- 6Shin J.O. Kim K. Kim H.S. Ko H.C. Kim B. Kim M.B. Shin K. Kim Y.H. Geographic differences in atopic dermatitis risk between urban and rural area: A systematic review and meta-analysis JDDG J. Der Dtsch. Dermatol. Ges.20232197398210.1111/ddg.1513537560937 · doi ↗ · pubmed ↗
- 7Nielsen M. D’Agostino D. Gregory P. Addressing Rural Health Challenges Head On Mo. Med.201711436336630228634 PMC 6140198 · pubmed ↗
- 8Morris-Paxton A.A. Reid S. Ewing R.-M.G. Primary healthcare services in the rural Eastern Cape, South Africa: Evaluating a service-support project Afr. J. Prim. Health Care Fam. Med.202012 a 220710.4102/phcfm.v 12i 1.2207 PMC 720318632242430 · doi ↗ · pubmed ↗