Development and Exploratory Validation of the Clinical Research Nursing Competencies-Self-Efficacy Scale
Mattia Bozzetti, Laura Apadula, Arianna Magon, Gianluca Conte, Daniele Napolitano, Giulia Villa, Monica Guberti, Rosario Caruso

TL;DR
A new scale to measure clinical research nurses' confidence in their skills was developed and validated, showing that experience and education influence confidence levels.
Contribution
The first validated self-efficacy instrument specifically for clinical research nursing, capturing its full scope and enabling targeted training and workforce planning.
Findings
The Se-CRN scale has a five-domain structure aligned with core clinical research nursing practice areas.
Higher self-efficacy is strongly linked to research-setting experience and, to a lesser extent, advanced education.
The scale shows excellent reliability and can identify strengths and gaps in nurses' perceived capabilities.
Abstract
What are the main findings? A new, theory-grounded self-efficacy scale for Clinical Research Nursing (Se-CRN) was developed and validated, supporting a five-domain structure aligned with core CRN practice areas.Competency-related self-efficacy was most strongly associated with research-setting experience (and, to a lesser extent, advanced education), with comparatively lower confidence in study management and scientific contribution domains. A new, theory-grounded self-efficacy scale for Clinical Research Nursing (Se-CRN) was developed and validated, supporting a five-domain structure aligned with core CRN practice areas. Competency-related self-efficacy was most strongly associated with research-setting experience (and, to a lesser extent, advanced education), with comparatively lower confidence in study management and scientific contribution domains. What are the implications of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
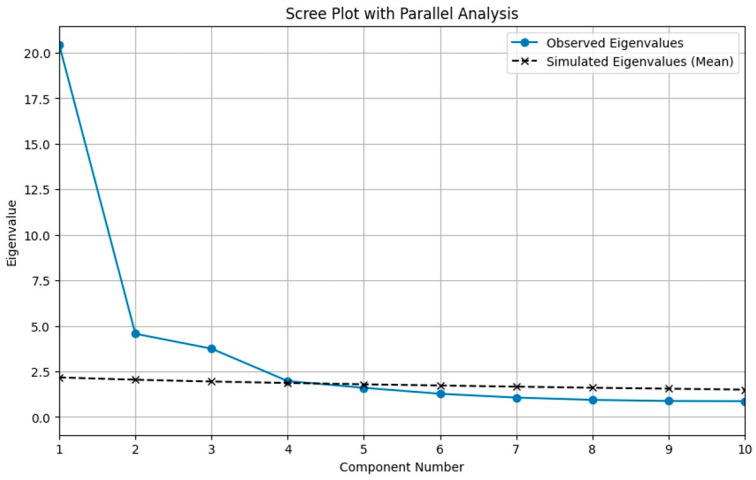 Figure 1
Figure 1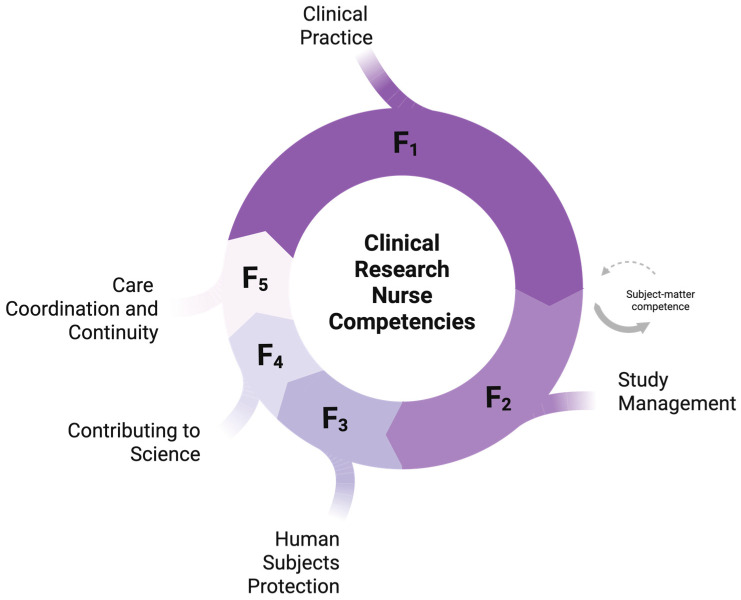 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Sciences Research and Education · Nursing education and management · Health Education and Validation
1. Introduction
Clinical research nursing is defined as the specialized practice of nursing that balances the protection of research participants with the fidelity to study protocols. Clinical research nursing represents a unique intersection between biomedical science and patient-centered care [1]. In accordance with this dual mandate, CRN competence must be both adequate and dynamically updated to safeguard the quality and safety of both patients and research [2,3]. At the same time, the next decade will see rising complexity in healthcare delivery, driven by technological innovation and the diversification of care settings, requiring evolving competency sets [4]. These pressures are especially acute for Clinical Research Nurses (CRNs), who must navigate trials that are becoming more complex in design and conduct—spanning multisite coordination, data-intensive platforms, and rigorous regulatory requirements—while maintaining high-quality patient care and protocol fidelity [5]. Against this backdrop, well-prepared and motivated nurses become indispensable for delivering safe and effective care across all levels of the health system [6]. Critically, where nurse shortages persist, organizations triage scarce staff toward mandated routine and acute care [7]; research functions are among the first to be curtailed [8]. These dynamics are exacerbated by short-term, project-based contracts and limited formal recognition of the CRN role, which make research capacity particularly vulnerable during staffing crises [9].
Within this evolving landscape, CRNs must develop the capacity to recognize their knowledge gaps and professional development needs and to cultivate self-efficacy [10,11]. Nursing self-efficacy could be considered a reliable proxy for nurses’ work performance [12,13]. Self-efficacy is a core construct of social cognitive theory that denotes beliefs about one’s capability to perform task-specific activities and to manage challenging situations [14,15]. It is a modifiable predictor of performance that can be enhanced through targeted educational and motivational strategies, and it mediates the translation of knowledge into action. Self-efficacy is foundational to nursing practice and education because it can influence performance by influencing behaviors [12]. In this sense, domain-specific self-efficacy offers a theory-grounded, measurable indicator of competency development and readiness for increasingly complex trial work.
Beyond competence development, self-efficacy is embedded in broader psychosocial processes that shape nurses’ well-being, role functioning, and workforce sustainability. Recent evidence highlights how emotional functioning and psychological resources (such as emotional intelligence and perceived efficacy) relate to burnout and well-being in nursing populations and can be strengthened through structured learning experiences [16,17]. Complementary work from European settings also indicates that moral stressors and moral injury can erode nurses’ well-being and contribute to disengagement and turnover-related outcomes [18].
Yet, notwithstanding the availability of national and international competency frameworks [19,20,21], the evidence base underpinning their implementation remains mainly descriptive. A recent scoping review found that, although these frameworks comprehensively catalogue role domains and skills, institutional uptake is inconsistent, and psychometric or outcome-based evaluations are sparse or non-existent [9]. Most existing studies have focused on mapping CRN activities in terms of frequency and perceived importance, rather than investigating competence [22,23,24,25]. Moreover, the literature seldom links CRN competencies to patient-level outcomes and continues to document role ambiguity and organizational barriers that impede systematic evaluation [9]. This evidence gap underscores the need for empirically tested measures that operationalize competency-related constructs and enable hypothesis-driven studies on training, role development, and impact.
Thus far, no available tool has been designed or psychometrically tested to capture self-efficacy as a theory-grounded proxy of CRN competence across the full scope of research activities [9]. Existing measures typically assess generic professional confidence or focus on isolated task domains, providing limited value for evaluating readiness to manage increasingly complex trials or for guiding targeted professional development. Without robust self-efficacy metrics, educational interventions cannot be rigorously assessed, competency gaps cannot be systematically monitored, and the contribution of CRNs to research quality and participant safety remains under-operationalized [26]. For these reasons, this study reports the development and psychometric evaluation of the Clinical Research Nursing Competencies–Self-Efficacy (Se-CRN) scale, theoretically grounded in the Bevans–Castro taxonomy [20].
In this study, we aimed to develop and conduct an initial psychometric evaluation of the Se-CRN scale, a theory-grounded and practice-relevant instrument designed to assess CRNs’ self-efficacy across competency domains relevant to increasingly complex clinical trials. By operationalizing an established CRN competency taxonomy into measurable self-efficacy domains, we also provide empirical support for the coherence and measurability of these domains in an Italian CRNs sample.
2. Materials and Methods
2.1. Design
A validation study was conducted from July 2022 to September 2025, comprising two sequential phases within an exploratory sequential mixed-method design [27]. The first phase involves scale derivation, including construct definition and item generation, expert consultation and item revision, quantitative content validity analysis, and pilot testing for comprehensibility. The second phase consists of a cross-sectional study for psychometric evaluation. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies [28].
2.1.1. Theoretical Framework and Item Pooling
According to Castro et al. [20], the conceptualization of the role draws on the five theoretical dimensions originally proposed by Hastings [21]: (1) clinical practice, (2) study management, (3) care coordination and continuity, (4) human subject protection, and (5) contributing to the science.
To operationalize these domains, 51 competencies for each dimension were developed and subsequently validated using the Delphi technique. The competencies were distributed as follows: clinical practice (4 activities), study management (24 activities), care coordination and continuity (9 activities), human subject protection (6 activities), and contributing to the science (8 activities). Based on the validated taxonomy and its corresponding competencies, the first version of the Se-CRN instrument was developed, comprising 51 items that reflect the various functions performed by CRNs in their professional roles. A back-translation procedure [29] was conducted for all items, and two were modified to ensure conceptual and contextual equivalence with the Italian National Health Service. During the item pooling phase, collegial discussions among subject-matter experts were held to critically examine and synthesize findings from the literature review [9], aiming to reach consensus on the most relevant competencies defining the CRN role. Based on this consensus, the conceptual dimensions underlying the Se-CRN questionnaire were confirmed, and an initial item pool was identified for inclusion in the instrument’s development.
2.1.2. Face and Content Validity
Following the identification of the item pool, a panel of domain experts—comprising both methodological experts (nurse researchers and university faculty) and content experts (experienced CRNs)—was invited to assess the pertinence and relevance of each item for inclusion in the Se-CRN.
Face validity involves assessing the expert group’s perception of the completion of the Se-CRN Questionnaire [30]. To address this need, three open-ended questions were administered and subsequently analyzed using a qualitative approach [31]. Consideration was given to any suggestions for clarifying the items in relation to their linguistic form. Additionally, the questionnaire was revised based on the results. Each expert was asked to indicate their degree of agreement for every identified item through two distinct evaluations: essentiality (rated on a 3-point Likert scale where 1 = “not essential”; 3 = “essential”) and relevance (rated on a 4-point Likert scale where 1 = “not relevant”; 4 = “completely relevant”). These assessments were used to calculate the Content Validity Index (CVI) and the Content Validity Ratio (CVR) [32], which quantify the representativeness and essentiality of each item. In line with commonly accepted criteria, an Item-CVI (I-CVI) of ≥0.78 was considered the minimum acceptable threshold for adequate relevance when evaluated by six or more experts [33]. For the CVR, Lawshe’s critical values were adopted; therefore, a CVR ≥ 0.62 was required to determine that an item met the threshold for essentiality with a panel of ten experts [32].
2.2. Data Collection
The final version of the Se-CRN Questionnaire was administered through an online survey platform (SurveyMonkey©). The Se-CRN is a 5-point Likert-type scale ranging from 1 (“Not at all confident”) to 5 (“Completely confident”), with higher scores indicating greater perceived self-efficacy in performing specific professional competencies. The response anchors were designed to capture both the strength and frequency of confidence judgments, consistent with Bandura’s self-efficacy theory. Each item is introduced by the trigger question: “How confident are you in your ability to perform the following activity?”. Higher total or domain-specific scores reflect stronger perceived self-efficacy within the corresponding area of clinical research nursing practice. In addition to the self-efficacy items, the questionnaire includes a brief introductory section that collects socio-demographic and professional information (e.g., gender, age, educational background, years of experience in clinical research, institutional setting) to contextualize participants’ self-efficacy profiles.
2.3. Inclusion Criteria
Participation in this study was voluntary. CRNs (as the nurses caring for patients enrolled in clinical trials) [9] were eligible for inclusion if they met the following criteria: (i) Full-time employment contract; (ii) Professional experience in clinical research exceeding six months. A non-probability purposive and snowball sampling strategy was adopted, leveraging the Italian Association of Oncology Nursing network of affiliated professionals and relevant social media platforms.
2.4. Data Analysis
Data were analyzed using R 4.5.0 [34] and Python 3.3.1. Descriptive statistics were computed using means, standard deviations, and frequencies. Prior to factor extraction, assumptions of multivariate adequacy and factorability were evaluated. Sampling adequacy was assessed using the Kaiser–Meyer–Olkin (KMO) index, with values ≥0.80 considered meritorious for factor analysis and individual MSAs ≥ 0.70 acceptable. Bartlett’s Test of Sphericity was used to test the null hypothesis of an identity correlation matrix (α = 0.05). The number of factors to be extracted was determined using Parallel Analysis (PA) with 500 random permutations, retaining factors whose empirical eigenvalues exceeded the 95th percentile of the simulated distributions.
An Exploratory Factor Analysis (EFA) was performed using Maximum Likelihood (ML) extraction with oblimin rotation to allow for correlated latent dimensions. Factor retention was guided by convergent criteria: (i) parallel analysis, (ii) incremental improvement in model fit across competing solutions (three to six factors), (iii) interpretability/simple structure, and (iv) consistency with the a priori competency framework. Item evaluation followed an iterative inspection of the oblimin-rotated pattern matrix, communalities, and item complexity. Items were retained when primary factor loadings were ≥0.40 and secondary loadings were <0.30, or when the primary–secondary loading difference was ≥0.20. In a small number of cases with marginal cross-loadings (i.e., slightly above 0.30), items were retained if the primary loading remained clearly dominant and the content was theoretically essential to the domain. Structural validity was further evaluated using hierarchical reliability indices consistent with bifactor modelling. Internal consistency was examined using Cronbach’s alpha (α ≥ 0.70 acceptable; ≥0.90 excellent), McDonald’s omega total (ωt), omega hierarchical (ωh), Composite Reliability (CR ≥ 0.70), Signal-to-Noise Ratio (S/N > 1), and the Explained Common Variance (ECV) to evaluate the presence and strength of a general factor [35].
For inferential comparisons, three variables were dichotomized a priori based on conceptual and practice rationale within CRN literature. For setting-based comparisons, we created a dichotomous variable distinguishing Oncologic (nurses working in oncology or in both oncology and non-oncology settings) versus Non-oncologic (nurses working exclusively in non-oncology settings). Participants indicating ‘Both’ were therefore included in the Oncologic group (i.e., ‘any oncology exposure’ rule). Educational level was dichotomized as Post-basic (Master’s, postgraduate, or PhD) versus Basic (Bachelor’s degree or equivalent). Experience in setting was dichotomized as Experienced versus Novice using a ≥ 2 years threshold. The 2-year benchmark reflects the period commonly reported as necessary to transition beyond initial familiarization and to consolidate autonomous performance in complex nursing practice systems [36]. Accordingly, ≥2 years was considered an empirically defensible milestone for meaningful competency consolidation in CRN practice contexts. Associations between competence scores and participant characteristics were examined using non-parametric Mann–Whitney U tests (two-tailed α = 0.05) due to non-normality and unequal group sizes. Effect sizes were calculated as rank-biserial correlation (r) and classified according to Cohen’s criteria (≈0.10 small, ≈0.30 moderate, ≈0.50 large) [37]. Total and domain scores were calculated as the mean of their constituent items.
2.5. Ethical Statement
The non-interventional, minimal-risk, anonymous online survey of healthcare professionals was conducted in accordance with the principles of the Declaration of Helsinki [38] and national regulations governing research involving human participants. Participation was voluntary and anonymous, and all participants provided electronic informed consent prior to completing the questionnaire. The study protocol was reviewed and approved by the Scientific Committee of the Italian Society of Oncology Nursing under approval number 01/INT/2022. All participants gave their consent to the processing of their personal data in an anonymous and computerized format. Data were collected and analyzed in anonymous/aggregated form in accordance with data-protection requirements (GDPR).
According to applicable institutional policies for anonymous questionnaire studies, formal ethics committee was not required.
3. Results
A total of n = 183 CRNs with an average of 14.30 (SD = 8.90) years of professional experience and 7.67 (SD = 7.65) years in their current setting participated in the survey (Table 1). The majority of nurses worked in oncological settings (72.7%), while a minority worked in non-oncological settings (18.6%). In specific settings, most were in medical wards (68.9%), followed by other areas (16.4%), maternal–infant units (6.6%), surgical units (6.0%), and intensive care units (2.2%).
3.1. Content Validity
The initial 51-item pool was reduced to 49 items based on expert ratings. The average scale content validity index (S-CVI/Ave) was 0.96 (Supplementary File S1).
3.2. Structural Validity
Parallel analysis suggested a five-factor solution (Figure 1). The four-factor model fit significantly better than the three-factor model, TRd_(52)_ = 410.56, p < 0.001, CD = 1.07; adding a fifth factor further improved model fit, TRd_(53)_ = 210.34, p < 0.001, CD = 1.03. By contrast, the six-factor solution did not provide an improvement over the five-factor model, TRd_(54)_ = 42.18, p = 0.882, CD = 1.01.
The collected data were suitable for EFA, χ^2^(1176) = 8418.63, p < 0.001, KMO = 0.90 (range = 0.86–0.94).
The EFA yielded five distinct factors with interpretable loadings and minimal cross-loadings, corresponding to the theoretical domains: “Clinical Practice” (F1), “Study Management” (F2), “Human Subjects Protection” (F3), “Contributing to the Science” (F4), and “Care Coordination and Continuity” (F5) (Table 2).
3.3. Reliability
Internal consistency was excellent at the scale level (ωt = 0.96, (ωh) = 0.82, α = 0.96, CR = 0.96, S/N = 24.6, and ECV = 0.74), supporting a hierarchical structure with a strong general factor. Factor-level reliability indices are reported in Table 3.
3.4. Self-Efficacy Levels
Mean self-efficacy scores by factor and total scale are reported in Table 4.
Self-efficacy levels did not differ by clinical setting (oncology vs. non-oncology) for any factor (W range: 839–1189.5, all p > 0.16), as shown in Table 5. Educational level (post-basic vs basic) was associated with higher self-efficacy in Study Management (W = 1613.5, p = 0.002) and Contributing to the Science (W = 1631, p = 0.001), and on Total score (W = 1529, p = 0.013). The strongest differences emerged for experience in the current setting (≥2 years vs. <2 years), with higher self-efficacy across all five domains (W = 1084.5–1247, all p ≤ 0.010) and the Total score (W = 1247, p < 0.001).
4. Discussion
This study developed and tested the Se-CRN scale, providing the first quantitative measurement of self-efficacy across the competency domains of CRN. Whereas prior literature has primarily catalogued competencies and delineated role boundaries, our work operationalizes these domains into a psychometrically evaluated instrument anchored to the conceptual framework articulated by Bevans and Castro [20], originally derived from Hastings [21]. In a national Italian sample of CRNs, the scale showed excellent internal consistency at both total and subscale levels, and a five-factor structure that mirrors the theoretical model.
Exploratory analysis supported a five-factor solution: Clinical Practice, Study Management, Human Subject Protection, Contributing to the Science, and Care Coordination and Continuity (Figure 2). At the scale level, hierarchical reliability indices suggested a plausible bifactor structure with a robust general factor, supporting the concurrent reporting of total and domain scores.
The pattern observed—higher self-efficacy in Human Subject Protection and Care Coordination and Continuity, alongside comparatively lower levels in Study Management and Contributing to the Science—aligns with prior work showing that CRN practice is often supported for protocol safety functions, whereas managerial and scholarly activities are more variably enabled by organizations [9]. Study management and scientific contribution frequently depend on access to protected time, formal authority within trial governance, and structured research method support (e.g., opportunities to contribute to protocol development) [39]. Where these conditions are limited, lower domain-specific self-efficacy may reflect constrained role enactment rather than individual deficit. Accordingly, implementation strategies that operationalize competency frameworks into local training pathways (such as structured onboarding, mentorship and competency-based benchmarking) may be particularly relevant for strengthening self-efficacy in these domains [40,41]. In parallel, widespread role ambiguity—where the CRN role is often blurred with broader “research nurse” profiles (e.g., nurses involved only in academic research setting)—and inconsistent institutional recognition may further blunt perceived capability in cross-boundary competencies such as study leadership and scholarly contribution, precisely the areas where our subscale means were lower [42,43,44]. By operationalizing the CRN taxonomy into measurable self-efficacy domains, the Se-CRN offers a way to render these historically “invisible” competencies visible and trackable.
The factor solution reflects the dual identity of the clinical research nurse as, first and foremost, a clinical nurse who practices within a research-intensive environment [45,46]. In particular, the Clinical Practice and Care Coordination and Continuity domains capture core elements of advanced clinical nursing practice, such as patient and family education, advocacy, monitoring of clinical status and adverse events, interdisciplinary care planning, and coordination of care across visits and settings. Although the wording of the items is anchored in the context of clinical research, the underlying behaviors draw on fundamental clinical nursing competencies and presuppose robust subject-matter expertise in the conditions, treatments, and trajectories of illness involved in the studies. In this sense, CRN self-efficacy, as measured by the Se-CRN, is grounded in—and cannot be disentangled from—a solid clinical foundation.
Moreover, the present study shows that, within a pool of nurses who already possess advanced clinical expertise, competence self-efficacy is not simply a function of working in oncologic versus non-oncologic contexts. Estimates did not support meaningful differences by clinical specialty. Instead, experience within the research setting emerged as the most powerful explanatory mechanism for competence. Nurses with ≥2 years of experience demonstrated materially higher levels of self-efficacy across all five factors and in the total score, with moderate non-parametric effect sizes. This pattern should not be interpreted as diminishing the centrality of clinical expertise or subject-matter knowledge; being a CRN presupposes being a clinically competent nurse in a specific field. Instead, our data suggest that, once this clinical foundation is in place, the incremental development of CRN self-efficacy is primarily driven by situated role exposure, progressive enactment, and legitimate participation in research work—rather than by disciplinary label alone [36]. In this sense, CRN competence constitutes a distinct work domain that builds on, but does not replace, specialty-based nursing practice and develops within the epistemic, regulatory, and organizational logics of clinical research itself [20]. Educational level showed greater domain-specific influence, particularly in management and scientific contributions, indicating that formal advanced education may augment learning curves preferentially in the cognitive/analytic components of the role rather than in core operational safety and coordination functions. These findings collectively underscore the importance of structured experiential pathways, supervised practice, and professional role socialization mechanisms in accelerating progression toward competent, autonomous research nursing practice [9]. Given the cross-sectional design, these associations should be interpreted cautiously: they may reflect the accumulation of mastery experiences and role socialization in research environments, but they may also be influenced by selection and retention processes (i.e., nurses who remain in CRN roles may differ from those who exit). From an implementation standpoint, the findings reinforce the value of creating early, supported exposure to research work through supervised practice and mentorship, with progressive responsibility and benchmarking against domain-specific competencies—conditions that map onto the mechanisms through which self-efficacy is strengthened (mastery experiences, vicarious learning, and social persuasion) [47].
Beyond the Italian context, the theoretical grounding of the Se-CRN in internationally established competency frameworks supports its potential applicability in other health systems where CRNs contribute to the conduct of clinical trials. At the same time, contextual interpretation is warranted. Italy does not currently maintain a national registry of CRNs; therefore, available figures are necessarily approximate. Based on expert mapping, the Italian CRN workforce is estimated at about 200–250 nurses holding formally designated research-nursing posts, largely concentrated in IRCCS and other high-volume clinical trial centers [48], and this may undercount nurses contributing to research activities in non-IRCCS hospitals under non-standardized role titles. Within this denominator, our sample of 183 respondents likely represents more than two-thirds of the target population, enabling a robust picture of current self-efficacy patterns in the national workforce. Nevertheless, international validation, particularly in systems with different regulatory structures, role delineations, and professional pathways, is essential to test the generalizability and cultural adaptability of the scale, and to expand its utility in informing education, workforce planning, and quality improvement globally [49].
4.1. Limitations
A primary limitation is reliance on EFA without confirmatory analysis. This decision was methodologically pragmatic given the realistically small national population of CRNs in Italy (estimated ~200–250) and the absence of a national registry, which constrained the feasibility of an adequately powered independent CFA sample. Within these constraints, EFA with parallel analysis and strong sampling adequacy criteria represents a rational first step. Additionally, the sample was predominantly oncology-based and highly educated, which may limit generalizability to other settings. Recruitment through professional networks and social media platforms may have introduced selection bias, potentially over-representing nurses who are more motivated, digitally engaged, and already interested in clinical research. As a result, the sample may not fully reflect the broader population of Italian clinical research nurses, including those with lower levels of engagement, fewer formal opportunities for research involvement, or different contractual arrangements. Also, our sample was highly educated and predominantly oncology-based. Oncology trials often involve more intensive monitoring, protocol-driven workflows, and frequent safety assessments than other areas. This context may elevate self-efficacy and could contribute to higher ‘Clinical Practice’ scores and potential ceiling effects. Therefore, mean levels and variability may differ in lower-intensity research settings (e.g., observational studies) or among nurses with less advanced education. Future studies should validate the Se-CRN in more diverse samples and examine measurement invariance across specialties and educational strata.
These factors should be considered when extrapolating the present findings to other organizational and national contexts. Importantly, the Se-CRN should be interpreted as assessing self-efficacy (perceived capability) in clinical research practice on the assumption of an existing foundation of specialty-specific clinical competence. For workforce development and educational planning, Se-CRN scores are thus best used alongside, rather than instead of, initiatives that maintain and strengthen underlying clinical expertise.
4.2. Implications for Practice
The Se-CRN provides a theory-grounded, measurable indicator of perceived capability in the core domains of clinical research nursing. It offers practical utility for training needs’ assessment and targeted curriculum design, particularly in areas where confidence levels are lower, such as study management and research methods. The strong general factor supports the use of a total score for screening/benchmarking. In contrast, subscale scores could guide domain-specific interventions and workforce planning decisions (e.g., skill-mix and supervision models). Because self-efficacy is intertwined with broader well-being and burnout-related processes, using the Se-CRN to detect low-confidence domains may also support early identification of psychosocial support needs and preventive strategies alongside competency development.
5. Conclusions
The Se-CRN provides the first validated measure of clinical research nursing self-efficacy aligned with internationally recognized competency frameworks. Its psychometric structure enables reliable assessment of perceived capability at both the general and domain-specific levels. In applied settings, the Se-CRN may support early identification of domain-specific support needs, inform preventive and targeted professional development strategies (e.g., mentorship and training in study management and scientific contribution), and guide workforce planning. Future research should confirm the factor structure, test measurement invariance, and evaluate responsiveness to education and practice change across diverse health systems.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Nurses Association International Association of Clinical Research Nurses Clinical Research Nursing: Scope and Standards of Practice American Nurses Association Silver Spring, MD, USA 2016
- 2Kalsoom Z. Victor G. Virtanen H. Sultana N. What really matters for patient safety: Correlation of nurse competence with international patient safety goals J. Patient Saf. Risk Manag.20232810811510.1177/25160435221133955 · doi ↗
- 3Zaitoun R.A. Said N.B. de Tantillo L. Clinical nurse competence and its effect on patient safety culture: A systematic review BMC Nurs.20232217310.1186/s 12912-023-01305-w 37208727 PMC 10196295 · doi ↗ · pubmed ↗
- 4Stievano A. Caruso R. FriganovićA. The Specialist Nurse in European Healthcare 2030: ESNO Congress 2024 Highlights Healthcare 202412162310.3390/healthcare 1216162339201181 PMC 11353440 · doi ↗ · pubmed ↗
- 5Gumber L. Agbeleye O. Inskip A. Fairbairn R. Still M. Ouma L. Lozano-Kuehne J. Bardgett M. Isaacs J.D. Wason J.M. Operational complexities in international clinical trials: A systematic review of challenges and proposed solutions BMJ Open 202414 e 07713210.1136/bmjopen-2023-077132 PMC 1102945838626966 · doi ↗ · pubmed ↗
- 6Cooper E. Spilsbury K. Mc Caughan D. Thompson C. Butterworth T. Hanratty B. Priorities for the professional development of registered nurses in nursing homes: A Delphi study Age Ageing 201746394510.1093/ageing/afw 16028181630 · doi ↗ · pubmed ↗
- 7Park H. Yu S. Effective policies for eliminating nursing workforce shortages: A systematic review Health Policy Technol.2019829630310.1016/j.hlpt.2019.08.003 · doi ↗
- 8Thornton J. Clinical trials suspended in UK to prioritise COVID-19 studies and free up staff BMJ 2020368 m 117210.1136/bmj.m 117232205354 · doi ↗ · pubmed ↗