The Cascade of Care for Infectious Diseases in Newly Arrived Refugees
Mie Fryd Nielsen, Jane Agergaard, Rebecca Vigh Margolinsky, Line Kibsgaard, Mette Holm, Anne Mette Hvass, Christian Wejse

TL;DR
This study examines how newly arrived refugees in Denmark progress through healthcare after being diagnosed with infectious diseases, finding that many are lost to follow-up, which limits the effectiveness of screening programs.
Contribution
The study reveals significant loss to follow-up in refugee healthcare after infectious disease screening, highlighting systemic barriers in high-income countries.
Findings
Only 43% of refugees with hepatitis B surface antigen attended regular follow-up.
Loss to follow-up occurred in 57% of hepatitis B cases and both hepatitis C cases.
Only one syphilis case completed follow-up according to national guidelines.
Abstract
Public health relevance—How does this work relate to a public health issue? Newly arrived refugees are routinely screened for infectious diseases, yet little is known about what happens after a positive screening result and whether individuals successfully complete the cascade of care.Loss to follow-up after screening represents a critical gap in infectious disease control and refugee health, with potential consequences for both individual health outcomes and population-level disease prevention. Newly arrived refugees are routinely screened for infectious diseases, yet little is known about what happens after a positive screening result and whether individuals successfully complete the cascade of care. Loss to follow-up after screening represents a critical gap in infectious disease control and refugee health, with potential consequences for both individual health outcomes and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
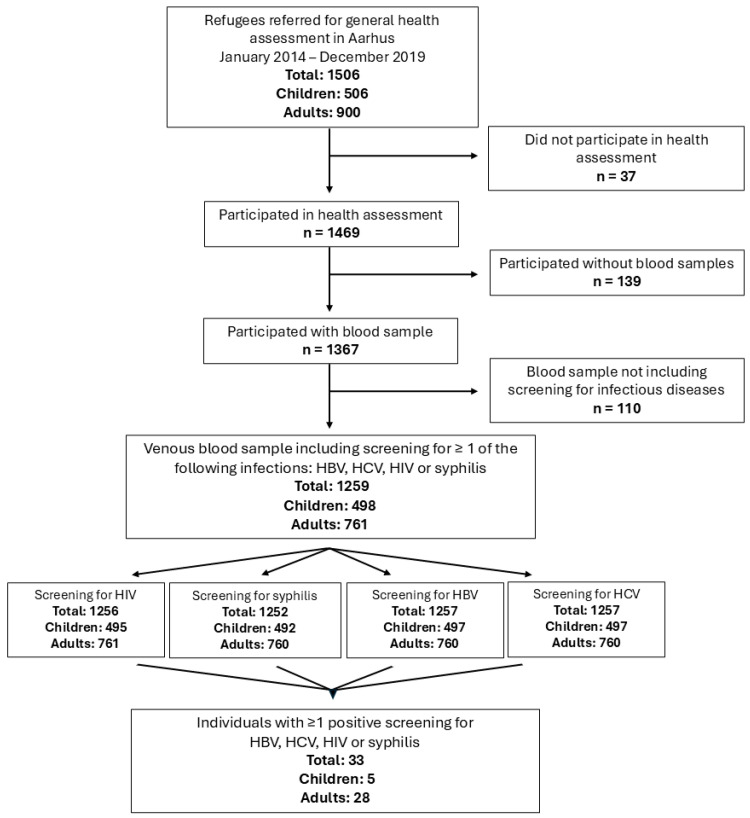 Figure 1
Figure 1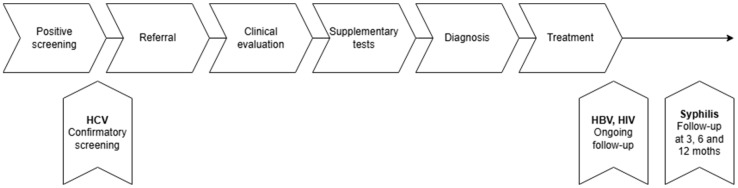 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigration, Health and Trauma · Travel-related health issues · Hepatitis B Virus Studies
1. Introduction
Global forced displacement has increased substantially over the past decades [1], and the health and care needed by this marginalised group is often neglected [2]. Refugees constitute a particularly vulnerable subgroup due to pre-migration exposure, precarious migration trajectories, and resettlement-related challenges [3]. Unlike migrants, whose movement is primarily voluntary, refugees are displaced due to conflict, persecution, or humanitarian crises, and therefore face distinct legal, social, and health-related vulnerabilities [4]. These factors contribute to an increased burden of both communicable and non-communicable diseases [5] compared with host populations, as well as heightened risks of unmet healthcare needs following arrival [6].
Consequently, several countries, including Denmark [7], offer post-arrival health assessments targeting selected infectious diseases such as hepatitis B virus (HBV), hepatitis C virus (HCV), human immunodeficiency virus (HIV), and syphilis [8,9]. While such screening initiatives are effective in identifying previously undiagnosed conditions [7,10] and are generally well accepted among refugees [11], their impact depends not only on case detection but also on successful progression through subsequent steps of care [4,12].
This progression is commonly conceptualised as the cascade of care, a model used for describing and evaluating the care provided by a healthcare system [8]. Breakdowns at any stage of this cascade may compromise individual health outcomes and undermine the public health benefit of screening programmes [11]. Previous studies have reported substantial loss to follow-up after initial screening, yet empirical data describing where and why refugees disengage from care remain limited, particularly in a Danish context.
In Denmark, responsibility for post-arrival health assessments lies with individual municipalities, resulting in marked local variation in scope, organisation, and systematic execution [13]. Unlike many municipalities, Aarhus has offered structured and systematic health assessments to newly arrived refugees since December 2013 [7]. This local initiative includes screening for HBV, HCV, HIV, and syphilis, providing a unique opportunity to examine not only disease prevalence but also the continuity of care within a defined municipal healthcare setting.
The present study examines a local cohort of newly arrived refugees screened for HBV, HCV, HIV, and syphilis in Aarhus, Denmark. The objectives were to (i) estimate the prevalence of these infectious diseases within the cohort and (ii) assess progression through the cascade of care following a positive screening result. Specifically, the study evaluates referral, attendance at clinical evaluation, follow-up according to national guidelines, and the documented reasons for attrition. By identifying critical points of loss to follow-up, the study aims to inform targeted improvements in the organisation and delivery of post-arrival infectious disease care for refugees.
2. Materials and Methods
2.1. Data from the AARHAUS Study
From January 2014 to January 2020 health assessments, consisting of medical history, a physical examination, and blood samples, were offered to 1506 newly arrived refugees in Aarhus, Denmark. The assessments were performed as a part of the AARHAUS study (Aarhus Refugee Health Assessments Using Systematic approaches) [7]. Participants arrived through three pathways: “quota refugees”, defined as refugees arriving through the quota system of The UN Refugee Agency; “asylum seeking refugees”, defined as refugees with asylum seeking backgrounds; and “family reunited refugees” defined as immigrants becoming reunited with family. The three groups are hereafter collectively referred to as “type of migration,” and the overall study population is referred to as “refugees.” All age groups were included. The practical aspects of the health assessments and inclusion criteria along with information about consent and permissions are described elsewhere. (Hvass et al.) [7]
A variety of screening tests were performed: (i) HBs-Ag detection, (ii) antibodies against HCV, (iii) HIV antibodies against HIV-1, HIV-2 and p24 antigen, or (iv) detection of syphilis non-specific antibodies through Wassermann reaction (WR) or rapid plasma regain (RPR). The tests were performed on blood samples. If venous punctures proved difficult, the blood samples were only repeated after consultation with a medical doctor. The results for tuberculosis screening are described elsewhere [14].
The cascade of care for patients who had positive screenings in any of the tests was evaluated in terms of referral, attendance at clinical evaluation and follow-up.
In addition to infectious disease screening results, baseline data on sex, age, country of origin, educational attainment, and migration status were extracted from the AARHAUS study. Age was recorded at the time of the health assessment. Participants aged 18 years or older were classified as adults, whereas those younger than 18 years were classified as children. The country of origin was defined according to participants’ self-reported country of origin. All participants who had received a residence permit within the last three years and who agreed to participate in the aforenamed health screening were included [7].
2.2. Statistical Analysis
The storage of the data is described elsewhere [7].
Because only 33 screened individuals had a positive result for an infectious disease, no statistical analyses were performed on this subgroup. Given the very small number of positive cases, we, as authors, chose not to present disaggregated data in order to avoid potential breaches of data protection and confidentiality regulations. The cascade of care was described descriptively based on information extracted from electronic medical records.
2.3. Data from Electronic Medical Records
In Denmark every patient has a unique personal social security number referred to as a CPR number, which is used as an ID number. When in contact with the hospital system in Denmark, the documentation provided by healthcare personnel is linked to the patient’s CPR number in specific electronic medical systems depending on which region the patient is seen. In the Central Region of Denmark, information is stored in the “Electronic Patient Journal” (EPJ) and data are available by healthcare providers involved in the hospitalisation.
The following data was collected from EPJ: (i) whether a referral to evaluation was received; (ii) whether the patient showed up to an evaluation at the hospital clinic; (iii) whether the patient was diagnosed by paraclinical test; and (iv) if any treatment was commenced/initiated and if so, what kind. We compared national guidelines to each medical record of the enrolled participants, to investigate the adherence to these guidelines. The correlation between the two indicated a sufficient cascade of care. The guidelines regarding supplementary tests and examinations on each infectious disease can be found in Table 1. We also used the electronic medical records to find data on compliance/adherence to treatment (a measurable virus was used as an indicator for non-adherence to treatment) and outpatient controls, follow up and outcome along the cascade of care. Data was collected retrospectively by February 2022.
As the infectious diseases of interest in this study require different procedures, the information extracted from the electronic medical files relied on what screening was positive.
For individuals with detected HBs-Ag or HIV antibodies against HIV-1, HIV-2 or p24 antigen, we investigated if the patient had ongoing appointments in the outpatient clinic, as infections with HBV and HIV are chronic and therefore require lifelong control. Furthermore, we investigated whether treatment was prescribed.
For participants with antibodies against HCV, we investigated if treatment was prescribed in case HCV-RNA was detected. As HCV is a disease often found in drug users, we searched for any data on reinfections.
With regard to participants with a positive screening test of syphilis, we investigated whether supplementary tests (Table 1), and antibiotics were offered according to the clinical stage [15]. As recommended by the International Union Against Sexually Transmitted Infection (IUSTI), participants that were syphilis positive were advised to consult the venereology outpatient clinic three, six and twelve months after the treatment had been provided [15].
During the execution of this study, the authors used ChatGPT (software GPT-5.2) for language revision. After using this tool, the authors reviewed and edited the content as needed and therefore take full responsibility for the content of the publication.
3. Results
A total of 1506 refugees underwent the health assessment. Participants originated primarily from Western Asia (67.1%), predominantly Syria (64.2%). Women constituted 46.2% of the cohort. Among all participants, the mean age was 22 years, and age ranged from 0 to 76. (Table 2).
Overall, 33 individuals (2.2%) had a positive screening result for at least one infectious disease: hepatitis B virus (HBV; n = 14), hepatitis C virus (HCV; n = 10), HIV (n = 1), or syphilis (n = 10). Three individuals screened positive for more than one infection. One initial positive syphilis screening was later refuted by confirmatory testing.
The total number of individuals screened for infectious diseases, as well as the distribution of positive screening results, is shown in Figure 1.
Given the small number of positive cases, the results are presented descriptively and no inferential statistical analyses were performed.
Of the 33 participants with a positive screening result, 29 (91%) were referred for specialist evaluation, and 25 (78.1%) attended at least one clinical assessment.
The reasons for non-attendance were inconsistently documented; all non-attenders had screened positive for HCV antibodies but had negative confirmatory HCV-RNA testing, after which no further follow-up was required.
3.1. HBV
Fifteen participants (13 adults and two adolescent) screened as positive for HBsAg. All were referred and evaluated at a specialist clinic and diagnosed with chronic inactive HBV infection. Six participants remained in follow-up at the time of inclusion, while eight were discharged from follow-up, most commonly due to repeated non-attendance. Overall, six of the fifteen participants completed follow-up consistent with the intended cascade of care.
One of the identified children with a positive HBV test was identified following a subsequent revision of the study population. However, the authors were unable to retrieve the corresponding medical record for this individual, and therefore the clinical course could not be examined or described in the present study.
3.2. HCV
Ten participants screened positive for HCV antibodies. Confirmatory HCV-RNA testing was positive in three cases and negative in seven. Seven individuals were referred for further evaluation; three attended clinical assessment. One participant completed antiviral treatment with documented adherence and no reinfection, while no participants with confirmed HCV infection completed the full cascade of care as defined in this study (Figure 2).
3.3. HIV
One adult participant screened positive for HIV-1 antibodies and was confirmed as HIV positive. The individual was referred, evaluated, and initiated on antiretroviral therapy, with documented attendance at follow-up visits until loss to follow-up later in the study period.
3.4. Syphilis
Ten participants (eight adults and two children) screened positive for syphilis and were referred for evaluation. Five individuals initiated treatment, and four completed the treatment as prescribed. Follow-up after treatment was documented in one case only. No participant fulfilled all components of the recommended cascade of care for syphilis (Figure 2).
3.5. Interpreters
Among the 27 participants who attended at least one clinical evaluation, an interpreter was present in 20 cases, either in person or via telephone or video. In cases without an interpreter, reasons were variably documented. In one instance, interpreter assistance was limited to part of the consultation.
4. Discussion
In this retrospective cohort study focusing on newly arrived refugees screened for selected infectious diseases in a Danish municipal setting, 2.1% of participants had at least one positive screening result for HBV, HCV, HIV, or syphilis. For HBsAg and HCV antibodies, the observed prevalences were 0.9% and 0.7%, respectively (Table 3). When compared with the systematic review by Hahné et al. [16], these estimates correspond more closely to the prevalence reported in the general European population (HBV: 0.1–5.6%; HCV: 0.4–5.2%) than to the higher prevalences previously described among refugee populations (HBV: 1.0–15.4%; HCV: 0–23.4%).
Several factors may contribute to this finding. The so-called “healthy migrant effect” [17], whereby individuals who migrate are often healthier at the time of arrival than both the host population and those remaining in the country of origin, may partially explain the low prevalence observed. In addition, the present cohort differed from many previously studied refugee populations in terms of country of origin, with a predominance of refugees from Syria and neighbouring regions, which is consistent with earlier studies reporting similarly low prevalence estimates among refugees from the Middle East and Western Asia [18,19].
A substantial loss to follow-up was observed among participants with chronic HBV infection, with only six of fourteen individuals completing follow-up consistent with national recommendations. This finding is directly supported by our results and represents one of the central observations of the study. Comparable challenges in continuity of care have been reported previously. A report by Médecins du Monde found that only 26% of undocumented migrants completed treatment or follow-up [20]. However, it should be noted that this population differs substantially from the present cohort of newly arrived refugees with legal residency and formal access to healthcare in Denmark. The comparison therefore serves primarily to illustrate that loss to follow-up is a recurrent challenge across vulnerable populations, rather than to suggest equivalence between settings.
Low adherence to follow-up among individuals with HBV and HCV may partly relate to the largely asymptomatic nature of these infections in early and intermediate stages [21,22]. In the absence of symptoms, patients may underestimate the importance of regular monitoring, despite the risk of long-term complications such as chronic liver disease [23,24]. This underscores the importance of adequate counselling and communication at the time of diagnosis, including clear information about disease progression and follow-up needs, ideally delivered with professional interpreter support. Stigma associated with blood-borne viral infections, often linked to sexual transmission or injection drug use, may further contribute to disengagement from care.
Only one participant screened positive for HIV, corresponding to a prevalence of 0.1%. Although this estimate is based on a single case, it is consistent with findings from other studies involving refugee populations from similar regions of origin [25]. Importantly, this individual was successfully linked to care and initiated on antiretroviral therapy, illustrating that post-arrival screening can facilitate timely HIV diagnosis and treatment even when its prevalence is low.
Syphilis remains a relevant infection to consider as it can remain asymptomatic for prolonged periods, and untreated infection may lead to severe late complications affecting the nervous system and sensory organs [26]. In the present study, wide variation in diagnostic work-up and follow-up was observed, and no participant completed the full recommended cascade of care. These findings suggest a need for clearer standardisation of diagnostic evaluation and follow-up, including the consistent use of WR and RPR as part of syphilis screening protocols among newly arrived refugees in Denmark.
In several cases, the documentation regarding interpreter use was limited. Among participants attending clinical evaluation, 26% did not have a documented interpreter present at the first consultation. While documentation quality does not directly determine patient outcomes, the absence of professional interpreter support represents a potential risk to effective communication and patient safety, as misinterpretation may lead to the misunderstanding of diagnoses, inadequate treatment, or poor adherence [27,28,29]. Improved documentation may help identify structural gaps and support quality improvement initiatives.
Strengths and Limitations
The strengths of this study include its six-year observation period and the inclusion of all newly arrived refugees undergoing systematic post-arrival screening in a large Danish municipality. In addition, the use of Denmark’s national electronic health record system allowed for the linkage of screening results with subsequent clinical management at the individual level.
Several limitations should be acknowledged. First, data were derived exclusively from electronic medical records, limiting insight into patient-reported barriers and reasons for disengagement from care. Second, heterogeneity in clinical practice—particularly in the management of syphilis across medical specialties—complicated the assessment of the adherence to guidelines. Moreover, incomplete documentation regarding interpreter use may have led to misclassification in some cases. An additional limitation relates to the very low number of participants with positive screening results. While this reflects a genuine finding of low disease prevalence, it limited the level of detail with which results could be presented and precluded meaningful subgroup analyses. Moreover, given the small number of positive cases within a well-defined local cohort, particular care was required to protect participant anonymity and comply with data protection regulations. As a consequence, data presentation was necessarily aggregated, and some potentially informative clinical characteristics could not be reported.
The descriptive nature of the analysis should be interpreted in light of these constraints. The study was not designed to assess associations or predictors of loss to follow-up, but rather to document progression through the cascade of care and identify critical points of attrition following post-arrival screening.
A subsequent revision of the study population identified one additional child with a positive HBV test who was included in the statistical analyses; however, the corresponding medical record could not be retrieved, and the individual clinical course could therefore not be examined or described.
5. Conclusions
In this local Danish cohort of newly arrived refugees, the prevalence of HBV, HCV, HIV, and syphilis identified through post-arrival screening was low and consistent with findings from comparable settings. While screening effectively enabled case identification, the principal finding of this study was substantial attrition at multiple stages of the cascade of care following a positive screening result.
In particular, loss to follow-up among individuals with chronic infections—most notably HBV—significantly limited the clinical impact of screening. These findings indicate that the effectiveness of post-arrival screening programmes depends not only on diagnostic testing but also on the healthcare system’s capacity to ensure sustained engagement in follow-up and treatment.
Targeted efforts to strengthen continuity of care, including clearer follow-up pathways, improved coordination across services, and the consistent use of professional interpreters, are needed to address these gaps. Future research should focus on identifying structural and individual barriers to retention in care and on developing interventions that support equitable and effective follow-up for refugees diagnosed through post-arrival screening.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1UNHCR Global Trends—Forced Displacement in 20202021 Available online: https://www.unhcr.org/60b 638e 37/unhcr-global-trends-2020(accessed on 1 December 2025)
- 2Matlin S.A. Depoux A. Schütte S. Flahault A. Saso L. Migrants’ and refugees’ health: Towards an agenda of solutions Henrique Barros, Bent Greve, Walter Ricciardi Public Health Rev.2018395510.1186/s 40985-018-0104-9 · doi ↗
- 3Zimmerman C. Kiss L. Hossain M. Migration and health: A framework for 21st century policy-making P Lo S Med.20118 e 100103410.1371/journal.pmed.100103421629681 PMC 3101201 · doi ↗ · pubmed ↗
- 4Office of the United Nations High Commissioner for Human Rights (OHCHR) Differentiation Between Migrants and Refugees 2018 Available online: https://www.ohchr.org/sites/default/files/Documents/Issues/Migration/Global Compact Migration/Migrants And Refugees.pdf(accessed on 15 November 2025)
- 5Hvass A.M.F. Wejse C. Systematic health screening of refugees after resettlement in recipient countries: A scoping review Ann. Hum. Biol.20174447548310.1080/03014460.2017.133089728562071 · doi ↗ · pubmed ↗
- 6Norredam M. Olsbjerg M. Petersen J.H. Bygbjerg I. Krasnik A. Mortality from infectious diseases among refugees and immigrants compared to native Danes: A historical prospective cohort study Trop. Med. Int. Health 20121722323010.1111/j.1365-3156.2011.02901.x 22032340 · doi ↗ · pubmed ↗
- 7Hvass A.M.F. Norredam M. Sodemann M. Wejse C. Is there a need of health assessments for resettling refugees? A cross-sectional study of 1431 refugees who arrived in Denmark between 2014 and 2018 J. Migr. Health 2021310004410.1016/j.jmh.2021.10004434405189 PMC 8352093 · doi ↗ · pubmed ↗
- 8Subbaraman R. Nathavitharana R.R. Satyanarayana S. Pai M. Thomas B.E. Chadha V.K. Rade K. Swaminathan S. Mayer K.H. The Tuberculosis Cascade of Care in India’s Public Sector: A Systematic Review and Meta-analysis P Lo S Med.201613 e 100214910.1371/journal.pmed.100214927780217 PMC 5079571 · doi ↗ · pubmed ↗