A Mixed Methods Evaluation of a Whole Food Plant-Based Nutrition Program for Medical Students
Tai Metzger, Deena Sukhon, Sophie Fisher, Zaheen Hossain, Virginia Uhley

TL;DR
A short plant-based nutrition program improved medical students' knowledge and confidence in dietary counseling, which could help reduce chronic diseases.
Contribution
The study introduces a scalable, experiential nutrition education model for medical students focused on plant-based diets.
Findings
Nutrition knowledge scores improved significantly from 73.3% to 87.0% after the intervention.
65% of participants reported increased knowledge of food ingredients, and 54% said they were more likely to choose plant-based options.
Themes included improved health, awareness of nutrition's role in medicine, and challenges with accessibility of plant-based diets.
Abstract
Public health relevance—How does this work relate to a public health issue? Diet-related chronic diseases, particularly cardiovascular disease and obesity, represent a leading and growing public health burden that is strongly influenced by modifiable dietary behaviors.Inadequate nutrition education among future physicians limits the healthcare system’s capacity to deliver effective, prevention-focused dietary counseling at the population level. Diet-related chronic diseases, particularly cardiovascular disease and obesity, represent a leading and growing public health burden that is strongly influenced by modifiable dietary behaviors. Inadequate nutrition education among future physicians limits the healthcare system’s capacity to deliver effective, prevention-focused dietary counseling at the population level. Public health significance—Why is this work of significance to public…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
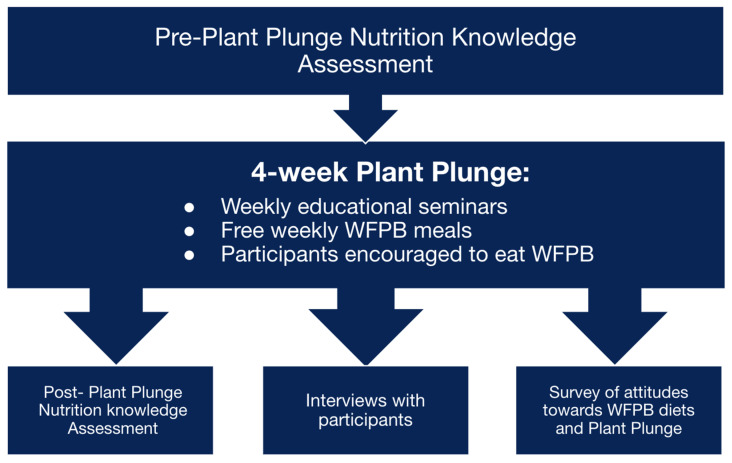 Figure 1
Figure 1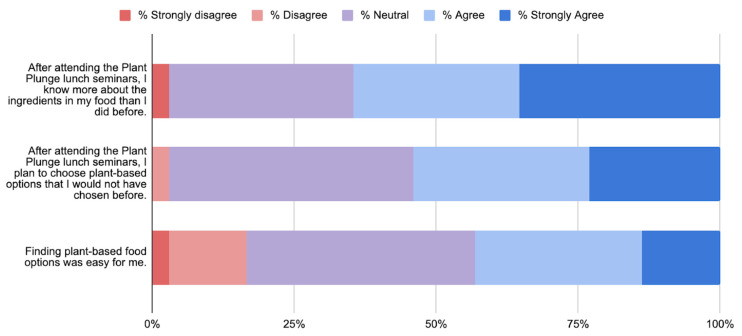 Figure 2
Figure 2- —Oakland University William Beaumont School of Medicine
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAgriculture Sustainability and Environmental Impact · Obesity and Health Practices · Food Security and Health in Diverse Populations
1. Introduction
Chronic diseases such as cardiovascular disease, type 2 diabetes, hyperlipidemia, and obesity-related cancers represent the leading causes of morbidity and mortality in the United States and globally. A significant body of evidence points to poor dietary habits as one of the most modifiable and impactful contributors to this burden [1,2,3]. The standard American diet, characterized by high consumption of saturated fats, refined carbohydrates, added sugars, excessive sodium, and ultra-processed foods, has been consistently linked with the development and progression of these chronic conditions [1,2]. As healthcare systems continue to shift their focus toward preventive models, dietary interventions have emerged as a key strategy in mitigating risk and improving long-term health outcomes. Systematic reviews and meta-analyses have shown that even modest weight gain in adulthood is associated with significant increases in risk for multiple comorbidities [3].
The urgency of addressing dietary behavior is further underscored by the rapid and ongoing rise in global obesity rates. Since 1975, the worldwide prevalence of obesity has tripled, with current estimates indicating that nearly 60% of adults are classified as overweight or obese in some regions [4]. Evidence strongly supports that lifestyle modification—particularly through improved dietary patterns—offers a scalable, sustainable, and cost-effective approach to both primary and secondary prevention of chronic disease [1,2,3]. Among the dietary strategies gaining widespread attention for their health-promoting potential is the whole food, plant-based (WFPB) diet. This dietary pattern emphasizes the consumption of minimally processed plant-derived foods, including fruits, vegetables, legumes, whole grains, nuts, and seeds [2]. It differs from vegetarian or vegan diets in that it does not strictly exclude animal products but instead focuses on maximizing plant food intake while minimizing processed and high-fat animal-derived products [2,3]. Research has shown that rather than targeting individual nutrients or food items, broader adherence to healthy dietary patterns yields more robust and long-lasting health benefits, particularly in reducing the risk of cardiovascular disease [5].
The potential health benefits of WFPB diets are supported by an expanding body of clinical and epidemiological research [6,7,8,9,10]. Observational and interventional studies have found that individuals who adopt WFPB dietary patterns experience reductions in body weight and improvements in weight-related biomarkers [6,7]. In addition, long-term adherence to these dietary patterns has been associated with lower all-cause mortality and decreased cardiovascular disease incidence and mortality [9,10]. Moreover, WFPB diets have been shown to decrease the risk of developing type 2 diabetes and to support better glycemic control and metabolic regulation in patients already diagnosed with the condition [9,11]. These findings support the clinical utility of WFPB diets not only as a preventive strategy but also as an adjunctive treatment in managing chronic illnesses.
Despite the wealth of evidence highlighting the importance of nutrition in health and disease, medical education has not kept pace with this paradigm shift. Major medical and professional organizations, including the American Society for Clinical Nutrition and the American Medical Student Association, have repeatedly emphasized the necessity of integrating comprehensive nutrition training into the medical school curriculum [12]. However, surveys and curriculum reviews indicate that current nutrition education remains insufficient and inconsistently applied across medical schools [13,14]. For example, many institutions do not meet the National Academy of Sciences recommended minimum of 25 h of nutrition instruction during medical school [15,16].
A closer look at the structure of nutrition education reveals further challenges. In a multi-institutional review of 30 medical schools, the majority of nutrition-related content was delivered through didactic lectures (33%) or stand-alone sessions (57%), with only 10% offered as electives [17]. The Nutrition Education in Medical Schools project identified notable gaps between what is taught and what is needed in clinical practice, advocating for a multidisciplinary approach to teach basic, applied, and clinical nutrition [18]. The lack of robust, experiential learning opportunities in medical school contributes to a gap in knowledge and confidence among physicians, hindering their ability to deliver nutritional care effectively [19,20,21]. The importance of addressing this gap is compounded because medical students themselves often struggle with maintaining healthy dietary habits. One study found that only 20% of medical students met the World Health Organization’s recommendation of consumption of fruits and vegetables [22]. Moreover, their dietary patterns tended to be high in sodium and animal fats [22]. The COVID-19 pandemic further exacerbated these trends, leading to increased consumption of fast food and energy drinks [23].
Encouragingly, recent interventions have shown that even brief, structured nutrition education programs can have a meaningful impact. In one experimental study, a four-week nutrition curriculum significantly improved students’ nutrition knowledge, confidence in counseling, dietary diversity, and consumption of fruits and vegetables [24]. By integrating nutrition education into both the formal curriculum and co-curricular activities, medical schools can empower students to adopt healthier lifestyles and enhance their capacity to deliver evidence-based dietary counseling in clinical practice.
In response to these needs, our study sought to evaluate the impact of a four-week WFPB dietary intervention and nutrition seminar series, known as the Plant Plunge, on medical students’ dietary knowledge and perceptions of nutrition education. Organized in partnership with Chickpea and Bean, a nonprofit dedicated to promoting plant-based nutrition, the Plant Plunge combined self-directed dietary changes, structured seminars, and biometric health assessments of participants blood pressure, weight, cholesterol, and glucose. Our aim was to explore participants’ perspectives on the value of the Plant Plunge nutrition seminars and their broader views on nutrition education within their medical training. This study contributes to the growing body of literature advocating for integrated, practical nutrition education in medical school and offers insights into the potential health benefits of plant-based eating among future healthcare providers.
2. Materials and Methods
2.1. Program Overview
“Plant Plunge” was a prospective, observational intervention conducted at Oakland University William Beaumont School of Medicine (OUWB), an allopathic (M.D.) medical school, in collaboration with Chickpea and Bean, a minority-led nonprofit based in Detroit (chickpeaandbean.com accessed on 18 December 2025). The organization is dedicated to promoting the benefits of WFPB nutrition through community engagement and education. Chickpea and Bean designed the Plant Plunge as a four-week intervention to increase awareness and adoption of plant-based dietary patterns while enhancing nutrition education for medical students. Methods are summarized in Figure 1.
The total population of medical students available for recruitment was 250, and all were invited to voluntarily participate in the Plant Plunge program, which was delivered in-person and free of cost. The program was advertised via GroupMe messages sent to the GroupMe chats of all OUWB classes. We did not have an a priori sample size goal. The program included three core components: (1) a personal challenge to eat a WFPB diet; (2) weekly nutrition seminars; and (3) biometric health screenings before and after the intervention, including weight, blood pressure, glucose, and cholesterol concentration. Glucose and cholesterol concentrations were measured using point-of-care machines from finger-prick collection rather than blood draw and were immediately available to participants. Biometric data was collected so that participants could see their own improvements, rather than for analysis in this paper. However, information on the biometric data was indirectly analyzed through references to these measurements during interviews.
Nutrition seminars were held weekly for four weeks, each one hour in duration and paired with a complimentary WFPB meal. The sessions took place in a lecture-style format and were facilitated by Chickpea and Bean educators and guest clinicians. A four-week intervention was selected in order to give participants sufficient time to experience eating a WFPB diet without having to make a long-term commitment greater than one month. This length also gave sufficient time to cover the content over the course of four, weekly sessions and fit with the budget and schedule of Chickpea and Bean. The content of the curriculum was developed by Chickpea and Bean based on the educational content that they provide in the community and consisted of PowerPoint presentations (version 16.105.2). Sessions were hosted in a classroom on campus. The vegan lunches were purchased from local restaurants by Chickpea and Bean and included Mexican sopes, Mediterranean rice bowls with falafel and hummus, pizza with vegan cheese and pepperoni, and vegetable wraps. Recipes for these meals were not provided.
The seminar content was structured around progressive educational goals. Week 1 introduced the program and included patient narratives from individuals who had reversed chronic disease through a WFPB lifestyle. Week 2 covered nutrition label literacy, grocery shopping strategies, and common food misconceptions. Week 3 addressed social and environmental barriers to plant-based eating, including cost, dining out, and peer influence, and included example recipe. Week 4 featured a board-certified internist trained in integrative and lifestyle medicine, who presented on the clinical applications of WFPB nutrition and led an open Q&A discussion.
Key outcomes were nutrition knowledge measured using pre- and post-Plant Plunge knowledge assessments, attitudes toward plant-based eating and the Plant Plunge using semi-structured interviews, and intention to change diets using a post-intervention survey. Demographic information was not collected. Participation in the interviews, pre-and post- assessments, and survey was not required and was open to any attendees who chose to participate. Participants were encouraged but not required to attend all four seminars.
2.2. Participant Recruitment
Participants were recruited through student listservs, class announcements, and student-led interest groups. All medical students were eligible to participate regardless of year or prior nutrition experience. Participation was voluntary and not incentivized. Students who enrolled provided verbal informed consent. De-identified data were stored in a secure Google Drive folder accessible only to the research team.
2.3. Interview-Based Data Collection
To further explore student perceptions of the program, participants were invited to participate in brief, semi-structured interviews (Appendix A). Because the Plant Plunge represented a relatively novel educational and dietary intervention, qualitative interviews allowed us to explore unanticipated themes and better understand the factors influencing its impact. Semi-structured interviews were used to capture nuanced, open-ended responses that could not be fully assessed through quantitative measures, providing insight into participants’ experiences and perceptions. The interview guide was developed by the study authors in collaboration with expert faculty and the Plant Plunge coordinators. We asked participants about their experiences with the Plant Plunge, attitudes toward the 4-week program, the educational content of the seminars, changes in their pre- and post- intervention measures (weight, blood pressure, glucose, and cholesterol concentrations), perceptions of medical school nutrition education, lifestyle medicine, personal attitudes toward plant-based eating, and dietary habits. Interviews were conducted by trained student researchers, recorded with consent, and transcribed verbatim. Two independent reviewers used thematic analysis to code transcripts. Interviews were analyzed for themes in an iterative process until percent agreement between reviewers reached 80%. Coding continued until thematic saturation was reached, defined as the point at which no new concepts or themes emerged.
2.4. Pre- and Post-Program Knowledge Assessment
To assess the educational impact of the seminar series, participants completed a 10-question knowledge assessment before and after the four-week intervention. The assessment was created by the authors of the study and reviewed by expert faculty and the Plant Plunge hosts to ensure validity. The questions evaluated students’ understanding of WFPB nutrition, interpretation of food labels, and knowledge of dietary risk factors for chronic disease. The same instrument was administered pre- and post-intervention using anonymous codes. Data were analyzed using a two-tailed t-test to determine whether the observed differences in mean scores were statistically significant. The knowledge assessment can be found in Appendix B.
The pre- and post-intervention knowledge assessment was a purpose-built instrument developed to evaluate learning objectives specific to the Plant Plunge curriculum, including whole food, plant-based (WFPB) nutrition principles, food label interpretation, and dietary risk factors for chronic disease. Because no existing validated questionnaire fully captured these targeted domains in medical trainees, the assessment was developed using a content-validity–driven approach [25,26]. Initial items were drafted based on seminar objectives and the nutrition education literature, then reviewed and refined through expert evaluation by faculty with experience in nutrition education and lifestyle medicine, as well as program educators, to ensure relevance, clarity, and alignment with evidence-based concepts. Face validity was supported by the direct correspondence between assessment items and instructional content. Preliminary construct validity is suggested by the improvement in scores following the intervention, indicating sensitivity to educational change consistent with established methods for evaluating short-term educational interventions [25,26].
2.5. Post-Intervention Survey on Attitudes and Perceptions
At the end of the program, all participants were asked to complete an anonymous post-intervention survey. The short survey assessed student attitudes toward the Plant Plunge program and plant-based eating. Responses were collected using a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree) and analyzed descriptively.
The post-intervention survey assessing attitudes and perceptions toward the Plant Plunge and plant-based eating was developed using expert-informed content validation [25,26]. Survey items were designed to capture key attitudinal constructs addressed during the program, including perceived nutrition knowledge, intention to choose plant-based foods, and feasibility of adopting WFPB dietary patterns. Draft items were reviewed by the study team and faculty experts to ensure conceptual clarity, appropriateness for medical students, and alignment with program goals consistent with survey best practices in medical education developed by International Association for Health Professions Education (AMEE) [27]. Face validity was supported by the use of clear, behaviorally anchored Likert-scale statements directly reflecting participant experiences during the intervention. Construct validity was further supported through triangulation with qualitative interview findings, which demonstrated thematic consistency between survey responses and in-depth participant narratives. Given the exploratory nature of this pilot study, the survey was intended to assess perceived impact rather than serve as a fully standardized psychometric instrument with formal reliability testing and factor analysis in which a larger sample is needed.
3. Results
3.1. Interviews
A total of 64 students participated in the plant plunge (26% of the total student body), and 30 had biometric data obtained. A total of 14 interviews were conducted. The interviews revealed seven recurring themes about the participants’ personal and professional growth (Table 1). Nine students emphasized how the program deepened their understanding of nutrition and introduced them to the health benefits of a WFPB diet. Participants described learning new and practical information about food labels, plant-based substitutions, and the role of diet in managing and preventing chronic conditions. For some, the experience corrected misconceptions about plant-based nutrition and empowered them to take greater ownership of their health. This was particularly impactful for students who reported improvements in objective health markers such as weight loss, cholesterol reduction, or improved digestion. According to six interviewees, these outcomes not only reinforced the value of dietary change but also motivated ongoing behavioral adjustments beyond the four-week program.
Students frequently highlighted the gap between their nutrition education during medical school and the real-world applicability of what they learned during the Plant Plunge. Six participants reflected that they had not previously been exposed to this type of information in their medical curriculum, despite its clear relevance to patient care. The program was viewed as a much-needed supplement to traditional medical training, with students calling attention to the lack of structured nutrition instruction and the missed opportunity this presents for future physicians. Seven participants expressed a newfound commitment to integrating dietary counseling into their future clinical practice, acknowledging that current medical education often prioritizes pharmacologic treatment over preventive, lifestyle-based strategies. The seminar series provided by Chickpea and Bean was praised for being understandable, evidence-based, and immediately applicable—qualities that students said were rarely found in formal coursework.
Despite the overall positive feedback, participants acknowledged several challenges in adopting and maintaining a WFPB lifestyle. While seven participants found the vegan meals surprisingly enjoyable, four noted initial concerns about the effort and accessibility required to make dietary changes, particularly around cost, convenience, and finding suitable substitutes for familiar foods. Nevertheless, five students reported that these barriers were easier to overcome than expected, especially with the help of peer support and increased exposure to plant-based options.
3.2. Nutrition Knowledge Assessment
There were a total of 25 completed pre- and post-assessments of nutritional knowledge. We found a statistically significant increase in scores on the assessment from 73.3% to 87.0% following the Plant Plunge (p = 0.045).
3.3. Survey
There were a total of 49 survey participants (summarized in Figure 2). 65% agreed or strongly agreed with the statement “After attending the Plant Plunge lunch seminars, I know more about the ingredients in my food than I did before.” 54% agreed or strongly agreed with the statement “After attending the Plant Plunge lunch seminars, I plan to choose plant-based options that I would not have chosen before.” Only 1 student disagreed with the statement, and the rest were neutral. 43% agreed with the statement “Finding plant-based food options was easy for me.” 16% disagreed or strongly disagreed, with the rest being neutral.
4. Discussion
This study evaluated the impact of a four-week whole food, plant-based (WFPB) intervention—the Plant Plunge—on medical students’ nutrition knowledge, perceptions of medical education, and dietary attitudes. While previous research has shown the beneficial health effects of WFPB, our study provides new findings regarding the impact of an experiential WFPB educational program for medical students. Interviews highlighted a range of physical improvements, including better digestion, weight loss, reduced low-density lipoprotein (LDL) cholesterol, and enhanced energy levels. Students expressed surprise at how accessible and enjoyable WFPB eating could be, often commenting on the variety and taste of the plant-based meals. Many also reported behavioral shifts, such as continued interest in WFPB eating after the program’s conclusion. Post-intervention assessments revealed a statistically significant increase in nutrition knowledge. Survey results showed increased awareness of food ingredients, greater likelihood of choosing plant-based options, and mixed attitudes towards feasibility of implementing a plant-based diet.
Beyond personal health outcomes, the intervention also appeared to fill a notable gap in formal medical education. Interviewees consistently emphasized how the Plant Plunge offered practical, evidence-based nutrition education that was largely absent from their existing curriculum. Students valued the seminar content for its clarity and clinical relevance, and several stated that it improved their confidence in counseling patients on lifestyle changes. These findings align with earlier research by Coppoolse et al., who found that short-term nutrition interventions improved both knowledge and intent to counsel among medical students in the Netherlands [14]. Similarly, Bassin et al. described the widespread inadequacy of nutrition training in U.S. medical schools, noting that most programs fail to meet recommended minimums for nutrition instruction [17].
Our findings also support existing literature on the clinical efficacy of WFPB interventions. Bansal et al. demonstrated that group-based WFPB diet programs can significantly improve health outcomes in underserved patient populations, reinforcing the importance of dietary counseling as a public health strategy to combat chronic diseases [28]. This aligns with participants’ recognition of diet as a modifiable risk factor for chronic disease, and their expressed desire to integrate nutrition into their future clinical practice. Additional studies further validate these findings. For instance, Crowley et al. emphasized the role of practical, skill-based nutrition education in bridging the gap between knowledge and behavior [11], while a recent intervention by Amoore et al. showed that even short curricula can boost medical students’ dietary habits and counseling self-efficacy [24]. Moreover, medical students’ firsthand experiences with dietary change may serve as a catalyst for enhancing empathy and credibility in future patient counseling. By personally navigating facilitators and barriers to adopting a WFPB diet, such as feasibility concerns, social influences, food access, and perceived health changes, students gain practical insight into the lived challenges patients face when modifying dietary habits. This experiential understanding may translate into more nuanced, patient-centered counseling strategies, greater appreciation for structural determinants of nutrition, and a stronger commitment to advocating for accessible, culturally adaptable dietary interventions in clinical settings.
Despite these promising results, our study has several limitations. First, it was conducted at a single institution with a relatively small, self-selecting sample of medical students, which may limit generalizability. Participation was voluntary and may have attracted students with preexisting interest in nutrition or preventive medicine. While it is difficult to generalize the results to the general population, we believe it is useful to show the impact of this program on students who are already open to learning more about nutrition. There was also no control group and demographic data was not collected, making it difficult to ensure that effects were due to solely to the Plant Plunge. Additionally, biometric outcomes, such as weight loss, were self-reported, and long-term adherence to dietary changes was not assessed. These factors introduce potential biases and limit conclusions about sustained impact.
Future research should aim to replicate these findings in larger, more diverse medical student populations and evaluate long-term effects on dietary behavior and clinical application. Randomized controlled trials comparing different formats and durations of nutrition education could help identify optimal approaches. Additionally, integrating standardized nutrition competencies into the core curriculum—beyond elective or co-curricular offerings—may yield broader and more consistent improvements in preparedness to deliver nutrition care.
5. Conclusions
Ultimately, the Plant Plunge served as an effective experiential education model, equipping future physicians with practical skills and reinforcing the clinical importance of nutrition. Participants not only reported improved health and increased knowledge but also developed greater confidence in their ability to apply nutrition in patient care. As the burden of diet-related chronic disease continues to grow, these findings underscore an urgent need to incorporate lifestyle-focused, WFPB-centered education into mainstream medical training. Doing so may help cultivate a generation of physicians better prepared to address the root causes of chronic illness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Key T.J. Papier K. Tong T.Y.N. Plant-based diets and long-term health: Findings from the EPIC-Oxford study Proc. Nutr. Soc.20228119019810.1017/S 002966512100374835934687 PMC 7613518 · doi ↗ · pubmed ↗
- 2Grotto D. Zied E. The Standard American Diet and its relationship to the health status of Americans Nutr. Clin. Pract.20102560361210.1177/088453361038623421139124 · doi ↗ · pubmed ↗
- 3Jayedi A. Soltani S. Abdolshahi A. Shab-Bidar S. Healthy and unhealthy dietary patterns and the risk of chronic disease: An umbrella review of meta-analyses of prospective cohort studies Br. J. Nutr.20201241133114410.1017/S 000711452000233032600500 · doi ↗ · pubmed ↗
- 4Boutari C. Mantzoros C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on Metabolism 202213315521710.1016/j.metabol.2022.15521735584732 PMC 9107388 · doi ↗ · pubmed ↗
- 5Chareonrungrueangchai K. Wongkawinwoot K. Anothaisintawee T. Reutrakul S. Dietary Factors and Risks of Cardiovascular Diseases: An Umbrella Review Nutrients 202012108810.3390/nu 1204108832326404 PMC 7231110 · doi ↗ · pubmed ↗
- 6Bassin S.R. Ferreira De Carvalho J. Gulati M. A Review of Plant-Based Diets for Obesity Management Endocr. Pract.20243077978910.1016/j.eprac.2024.04.02038729570 · doi ↗ · pubmed ↗
- 7Wang Y. Liu B. Han H. Hu Y. Zhu L. Rimm E.B. Hu F.B. Sun Q. Associations between plant-based dietary patterns and risks of type 2 diabetes, cardiovascular disease, cancer, and mortality—a systematic review and meta-analysis Nutr. J.2023224610.1186/s 12937-023-00877-237789346 PMC 10548756 · doi ↗ · pubmed ↗
- 8Jafari S. Hezaveh E. Jalilpiran Y. Plant-based diets and risk of disease mortality: A systematic review and meta-analysis of cohort studies Crit. Rev. Food Sci. Nutr.2022627760777210.1080/10408398.2021.191862833951994 · doi ↗ · pubmed ↗