Global Disparities in Teletherapy Adoption: A Cross-Income Analysis of Mental Health Access
Gloria Nnadwa Alhassan, Arda Ozturkcan, Seyma Caliskan Cavdar

TL;DR
Teletherapy adoption varies globally, with high-income countries leading due to better infrastructure and policies, while low-income countries struggle with limited access and resources.
Contribution
This study quantifies teletherapy adoption disparities across income levels and identifies infrastructure, regulation, and workforce as key factors.
Findings
High-income countries achieved >70% teletherapy adoption due to broadband, regulation, and reimbursement.
Low-income countries had <5% adoption, hindered by poor internet, workforce shortages, and sociocultural barriers.
Digital infrastructure, regulation, and workforce density explained 78% of adoption variance across countries.
Abstract
Mental health disorders affect nearly one billion people worldwide, yet treatment gaps exceed 75% in low- and middle-income countries. Teletherapy has emerged as a scalable solution, but its adoption differs sharply by economic context. This comparative ecological policy analysis used secondary aggregate data from WHO, World Bank, ITU, and national reports to examine teletherapy adoption in low-income (Nigeria, Kenya), middle-income (South Africa, India), and high-income countries (Norway, Canada). Descriptive statistics and simple linear regression were applied, with findings interpreted through the Consolidated Framework for Implementation Research (CFIR), Technology Acceptance Model (TAM), and Diffusion of Innovations theory. High-income countries achieved widespread adoption (>70%), enabled by universal broadband, comprehensive regulation, and strong reimbursement. Middle-income…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
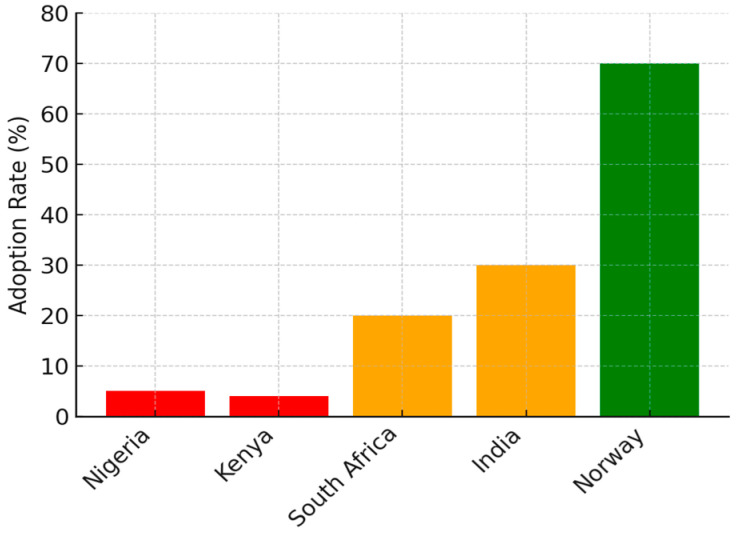 Figure 1
Figure 1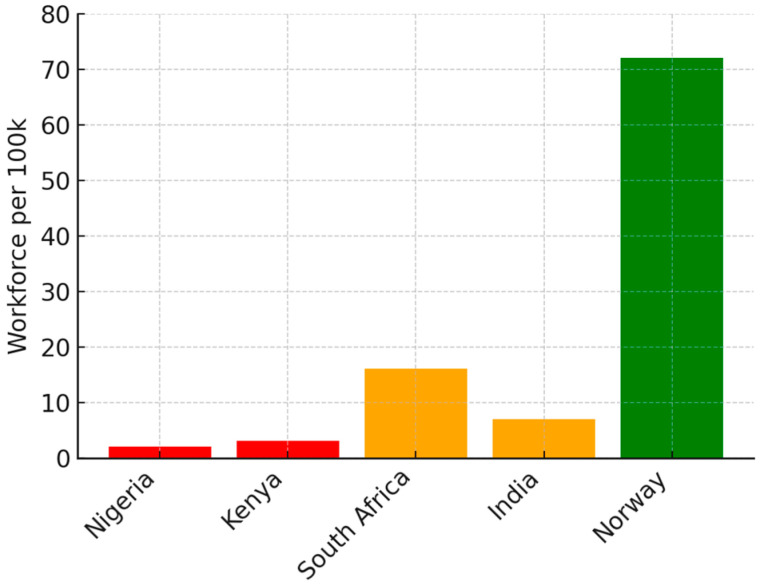 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Mental Health Interventions · Telemedicine and Telehealth Implementation · Mental Health Treatment and Access
1. Introduction
Mental health disorders constitute a significant global burden, affecting approximately 970 million people and accounting for 14.6% of total disability-adjusted life years (DALYs) [1]. Despite their high prevalence, access to mental health services remains starkly inequitable, with treatment gaps exceeding 75% in low- and middle-income countries (LMICs) compared to 40% in high-income countries (HICs) [2]. Workforce shortages further exacerbate these disparities, with LMICs averaging fewer than two mental health workers per 100,000 people, compared to over 70 per 100,000 in HICs [3].
Digital health innovations, particularly teletherapy, have emerged as potential solutions to expand mental health access by enabling remote service delivery [4]. The COVID-19 pandemic accelerated the adoption of digital mental health interventions globally, demonstrating their feasibility while exposing critical digital and structural inequities [5]. While HICs rapidly integrated teletherapy into healthcare systems—facilitated by robust infrastructure and policy frameworks—LMICs have faced substantial implementation challenges, including technological deficits, regulatory constraints, and socio-cultural resistance [6].
Although studies have explored the efficacy of teletherapy in high-resource settings, limited research has systematically compared teletherapy adoption across different economic contexts [7]. The absence of such comparative analyses restricts the development of scalable, context-specific strategies for mental health service expansion in LMICs. Furthermore, concerns persist regarding digital health inequities, where socioeconomically disadvantaged populations who bear the highest mental health burden face disproportionate barriers to digital service access [8].
Teletherapy is distinguished from general telehealth by its emphasis on therapeutic applications, emotional presence, and cultural adaptation of psychotherapeutic protocols [9]. These dimensions are uniquely sensitive to digital divides, making income-level comparisons particularly revealing.
Given the plethora of extant literature on the theme under review, this study seeks to address these gaps by conducting a cross-income comparative analysis of teletherapy adoption across low-income (Nigeria, Kenya), middle-income (South Africa, India), and high-income (Norway and Canada) countries. Specifically, it examines the adoption rates, implementation models, and policy frameworks governing teletherapy in different economic settings, secondly the technological, regulatory, and socio-economic factors influencing teletherapy adoption and the context-appropriate strategies to optimize digital mental health service delivery in resource-limited settings. Additionally, by generating evidence-based recommendations, this study seeks to inform equitable digital health policy development, ensuring that teletherapy implementation mitigates rather than exacerbates global mental health disparities.
The reminder of this study proceeds with data and method, and theoretical justification in Section 2. Subsequently, Section 3 presents the empirical results followed by the discussion section in Section 4. Finally, Section 5 renders the concluding remarks and policy implications driven from the study.
2. Methods
This study employs a comparative ecological policy analysis using secondary aggregate data to examine teletherapy adoption across low-income (Nigeria, Kenya), middle-income (South Africa, India), and high-income countries (Norway, Canada). Countries were purposively selected based on World Bank income classification, variation in digital infrastructure, and availability of national-level teletherapy indicators and policy documents.
2.1. Data Sources and Sources
Publicly available national-level indicators and policy documents (2015–October 2024) were retrieved from WHO Mental Health Atlas, World Bank Development Indicators, ITU World Telecommunication/ICT Indicators, national health ministry reports, and peer-reviewed literature identified through targeted searches in PubMed, Scopus, Web of Science, Google Scholar, and WHO IRIS using terms combining “teletherapy”, “telemental health”, country names, and “adoption/policy/implementation”. Only sources providing quantitative estimates of adoption rates, workforce density, broadband penetration, or regulatory status for the six selected countries were used. No formal risk-of-bias assessment was applied, as the analysis relies on official aggregate statistics rather than individual studies. Further insights are rendered in Table 1.
2.2. Analytical Approach
Data were organised in a structured matrix by country and income group. Key indicators were tabulated for descriptive comparison. Simple linear regression was performed on the seven country-level observations (six countries + pooled HIC average) to identify predictors of adoption.
2.3. Theoretical Frameworks
The study is grounded in three key theoretical models:
- Consolidated Framework for Implementation Research (CFIR)—domains used: Outer Setting (national policies, financing), Inner Setting (organisational culture, workforce readiness), Innovation Characteristics (relative advantage, compatibility, cost) [10].
- Rogers’ Diffusion of Innovation Theory: This theory explains how new ideas and technologies spread within a society. Rogers [11] posits that adoption occurs in stages: knowledge, persuasion, decision, implementation, and confirmation. Key factors influencing adoption include relative advantage, compatibility, complexity, trialability, and observability [11]. Given the disparities in teletherapy uptake between LICs, MICs, and HICs, this framework helps elucidate why certain regions experience faster diffusion of digital mental health services than others.
- Technology Acceptance Model (TAM): TAM, developed by Davis, ref. [12] explains how users come to accept and use a technology. It highlights two primary determinants: perceived usefulness (PU) and perceived ease of use (PEOU). This model is particularly relevant in evaluating the willingness of healthcare providers and patients to adopt teletherapy services, especially in settings with limited digital literacy or infrastructural challenges. The integration of CFIR, TAM, and Diffusion of Innovation theory has been made explicit, detailing which constructs guided coding, comparison, and interpretation.
The integration of CFIR, TAM, and Diffusion of Innovation theory has been made explicit, detailing which constructs guided comparison and interpretation. By integrating these theoretical perspectives, the study provides a multi-faceted analysis of teletherapy adoption across individual, organisational, and systemic levels [9,10,13,14].
3. Results
Substantial disparities exist in teletherapy adoption across economic settings. High-income countries (HICs), such as Norway, report integration rates exceeding 70%, while Canada similarly reports 68% adoption in 2023–2024 [15] supported by strong digital health policies, high provider capacity, and strong public trust in telehealth services [14,15]. In contrast, middle-income countries (MICs), including South Africa and India, exhibit moderate adoption (15–30%) due to emerging digital strategies and urban–rural disparities in accessibility [16]. Low-income countries (LICs), such as Nigeria and Kenya, report adoption rates below 5%, constrained by inadequate infrastructure, policy fragmentation, and workforce shortages [16,17].
The feasibility of teletherapy implementation is shaped by significant disparities in digital infrastructure. HICs benefit from universal broadband coverage and government-backed digital health initiatives, ensuring widespread service availability [5]. MICs show moderate connectivity, with rural–urban gaps in access. LICs face severe constraints, including unreliable networks, high data costs, and limited digital literacy, restricting teletherapy accessibility to small-scale initiatives.
HICs exhibit strong provider networks, enabling seamless teletherapy integration. MICs demonstrate variable adoption, with urban areas leveraging teletherapy while rural regions remain underserved. LICs experience critical shortages in trained mental health professionals, exacerbating access disparities [3,18].
The charts and table below summarize the disparities in teletherapy adoption across economic settings, highlighting variations in implementation levels, infrastructure barriers, and regulatory frameworks.
Figure 1 shows the teletherapy adoption rates by economic context—adoption is lowest in LICs—Nigeria and Kenya, (~5%), moderate in MICs—South Africa and India (~30%), and highest in HICs—Norway (~70%).
Figure 2 shows the mental health workforce per 100,000 people—LICs—Nigeria and Kenya, have a severe shortage (~2.5 per 100 k), MICs—South Africa and India, have moderate numbers (~15 per 100 k), while HICs—Norway, have robust staffing (~72 per 100 k).
Table 2 presents further disparities, showing that high-income countries (HICs) have advanced teletherapy strategies, MICs demonstrate emerging but inconsistent adoption, and LICs struggle with infrastructure challenges.
Simple linear regression on aggregate country-level data showed that log GDP per capita, broadband penetration, and mental health workforce density together explained 78% of the variance in reported teletherapy adoption rates (R^2^ = 0.78, p < 0.01; Table 3).
Results from this study show that technology, policy and regulation and equity considerations play a major role in facilitating or limiting teletherapy adoption.
Technological Barriers: Limited broadband coverage, high device costs, and low digital literacy hinder adoption, particularly in LICs and rural MICs. The lack of culturally and linguistically appropriate teletherapy platforms further reduces engagement, disproportionately affecting marginalized populations [8].Policy and Regulatory Challenges: Fragmented or absent regulatory frameworks in LICs limit teletherapy scale-up, while MICs show emerging but inconsistent policies. HICs have well-established digital health laws, facilitating reimbursement mechanisms and data privacy protections that support teletherapy expansion [19].Equity Considerations: The risk of digital exclusion remains a significant concern. Without targeted interventions, existing socioeconomic and geographic disparities may be exacerbated, reinforcing health inequities rather than addressing them [8,20].
4. Discussion and Policy Implications
This comprehensive analysis of teletherapy implementation across diverse economic contexts reveals substantial and multifaceted disparities influenced by structural, policy, and sociocultural factors. While high-income countries (HICs) like Norway demonstrate sophisticated teletherapy integration with adoption rates exceeding 70%, and Canada reports 68% teletherapy adoption in 2023–2024, reinforcing HIC patterns, middle-income countries (MICs) such as India and South Africa show moderate but inconsistent integration (15–30%), and low-income countries (LICs) including Nigeria and Kenya remain at marginal implementation levels (<5%) [15,20,21].
These findings extend beyond previous observations of mental health service gaps, ref. [2] uncovering a complex interplay of “digital determinants of health” that fundamentally shape teletherapy accessibility and effectiveness [5,22]. The stark variation in internet infrastructure—nearly universal in HICs versus limited, costly, and unreliable in LICs—directly impacts service delivery capacity, aligning with Crawford and Serhal’s [5,23,24] Digital Health Equity Framework while providing empirical evidence of its manifestation across economic strata. The analysis reveals that these digital determinants operate not merely as technological barriers but as structural inequities embedded within broader socioeconomic systems.
Unlike previous digital health research focused primarily on technological adoption factors [16], this study demonstrates that teletherapy implementation follows complex, context-dependent trajectories rather than the linear diffusion patterns predicted by traditional innovation diffusion theories. Implementation success appears contingent on the convergence of multiple factors: digital infrastructure readiness, healthcare workforce capacity, regulatory frameworks, financial mechanisms, and cultural acceptance—factors that vary significantly across and within economic contexts.
National policy environments critically influence implementation success, with considerable implications for teletherapy integration. Countries with comprehensive digital health strategies and well-articulated teletherapy-specific regulations (predominantly HICs) demonstrate more effective, equitable, and sustainable integration compared to those with fragmented or absent policy frameworks (primarily LICs), consistent with Walt and Gilson’s [19,25,26] policy analysis paradigm. This regulatory disparity manifests tangibly in healthcare workforce capacity, with marked variations in mental health professionals per 100,000 populations (Norway: 72; South Africa: 16; India: 7; Nigeria: 2; Kenya: 3), exceeding differences documented in the WHO Mental Health Atlas [3,15,26,27,28] and suggesting that digital solutions alone cannot overcome fundamental workforce limitations.
Sociocultural factors—including mental health stigma, trust in digital platforms, and preferences for traditional healing approaches—play equally determinative roles in shaping adoption patterns. Unlike assumptions that technology automatically increases service utilization [29,30] the findings suggest that cultural context profoundly mediates teletherapy acceptance and engagement. In settings where mental illness remains highly stigmatized or associated with traditional and supernatural beliefs, digital interventions face resistance beyond technological access barriers, necessitating culturally adapted implementation approaches rarely featured in current teletherapy platforms.
The pronounced urban-rural divide in teletherapy access, particularly evident in MICs, reinforces existing geographical inequities in mental healthcare provision, contradicting technological determinism narratives that suggest digital solutions inherently reduce disparities [5,6,24]. The data indicates that without targeted interventions addressing both technical infrastructure and socioeconomic barriers, teletherapy may paradoxically exacerbate rather than mitigate mental health inequalities a concerning possibility not adequately addressed in previous implementation research [21]. This challenge is particularly salient for marginalized populations who face intersecting barriers of limited connectivity, affordability constraints, and lower digital literacy.
Based on these multidimensional findings, an equity-centered implementation framework emerges, comprising three essential and interdependent policy framework (1) Infrastructure: National broadband funds (e.g., India’s BharatNet model) + zero-rated mental health data [31,32]; (2) Regulation: LIC telemedicine licensure reciprocity with HIC boards (e.g., Norway–Kenya twinning) [15,23]; (3) Workforce: Task-shifting to community health workers with 6-week digital CBT training (WHO Mental Health Gap Action Programme (mhGAP)) [33]. This framework acknowledges that successful teletherapy deployment requires simultaneous attention to both technological and human dimensions within specific socioeconomic contexts, moving beyond technocentric approaches that have characterized much digital health implementation to date.
Addressing these challenges aligns with several Sustainable Development Goals (SDGs), including SDG 3 (Good Health and Well-being) by promoting equitable mental health access, SDG 9 (Industry, Innovation, and Infrastructure) through digital health investment, and SDG 10 (Reduced Inequalities) by bridging healthcare access gaps. Additionally, SDG 4 (Quality Education) is relevant, as digital literacy and professional training are critical for scaling teletherapy, while SDG 17 (Partnerships for the Goals) highlights the need for global collaboration in developing sustainable and culturally adapted teletherapy models. Strengthening global collaboration and leveraging lessons from successful implementations can facilitate more inclusive and sustainable digital mental health strategies worldwide.
Several limitations of this study warrant acknowledgment. Despite examining multiple countries across income groups, data availability constrains generalizability to additional regions and healthcare contexts. Additionally, the rapid evolution of digital health technologies means these findings represent a contextual snapshot rather than definitive long-term trends. Also the review included only English-language sources and aggregated national data, masking subnational variation. Causal claims are limited by ecological design. The cross-sectional nature of the analysis also limits causal inferences regarding specific implementation factors and outcomes. Future research should explore artificial intelligence applications in expanding teletherapy accessibility, particularly in resource-constrained settings; examine lived experiences of underrepresented populations using mixed-methods approaches; and investigate sustainable financing models for equitable implementation beyond donor-dependent initiatives.
5. Conclusions
This study reveals profound global disparities in teletherapy adoption that are driven by digital infrastructure, regulatory maturity, and mental health workforce capacity rather than clinical need. High-income countries have successfully integrated teletherapy into routine care, while low- and middle-income countries remain largely excluded despite bearing the greatest burden of mental disorders. Without deliberate, equity-centered policies—including targeted infrastructure investment, regulatory transformation, and task-shifting models—teletherapy risks widening rather than narrowing the global mental health treatment gap. Strengthening cross-income collaboration and aligning digital mental health strategies with SDGs 3, 9, 10, and 17 offer a viable path toward more inclusive and sustainable service delivery worldwide.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization World Mental Health Report: Transforming Mental Health for All World Health Organization Geneva, Switzerland 2022 Available online: https://www.who.int/publications/i/item/9789240049338(accessed on 15 July 2025)
- 2Patel V. Saxena S. Lund C. Thornicroft G. Baingana F. Bolton P. Chisholm D. Collins P.Y. Cooper J.L. Eaton J. The Lancet Commission on global mental health and sustainable development Lancet 20183921553159810.1016/S 0140-6736(18)31612-X 30314863 · doi ↗ · pubmed ↗
- 3World Health Organization Mental Health Atlas 2020 World Health Organization Geneva, Switzerland 2021 Available online: https://www.who.int/publications/i/item/9789240036703(accessed on 8 September 2025)
- 4Torous J. Myrick K.J. Rauseo-Ricupero N. Firth J. Digital mental health and COVID-19: Using technology today to accelerate the curve on access and quality tomorrow JMIR Ment. Health 20207 e 1884810.2196/1884832213476 PMC 7101061 · doi ↗ · pubmed ↗
- 5Crawford A. Serhal E. Digital health equity and COVID-19: The innovation curve cannot reinforce the social gradient of health J. Med. Internet Res.202022 e 1936110.2196/1936132452816 PMC 7268667 · doi ↗ · pubmed ↗
- 6Blandford A. Wesson J. Amalberti R. Al Hazme R. Allwihan R. Opportunities and challenges for telehealth within, and beyond, a pandemic Lancet Glob. Health 20208 e 1364-510.1016/S 2214-109X(20)30362-432791119 PMC 7417162 · doi ↗ · pubmed ↗
- 7Berryhill M.B. Culmer N. Williams N. Halli-Tierney A. Betancourt A. Roberts H. King M. Videoconferencing psychotherapy and depression: A systematic review Telemed. e-Health 20192543544610.1089/tmj.2018.005830048211 · doi ↗ · pubmed ↗
- 8Figueroa C.A. Aguilera A. The need for a mental health technology revolution in the COVID-19 pandemic Front. Psychiatry 20201152310.3389/fpsyt.2020.0052332581891 PMC 7283500 · doi ↗ · pubmed ↗