Assessing the Inclusion of Music Therapy and Music Interventions in National Dementia Strategies and Clinical Practice Guidelines: A Scoping Review
Victoria McArthur, Martyn Patel

TL;DR
This review finds that music therapy is rarely included in dementia care guidelines despite its potential benefits.
Contribution
The study is the first to systematically assess the inclusion of music therapy in national dementia strategies and guidelines.
Findings
Only seven of 19 dementia guidelines included music therapy or music interventions.
Music therapy was less frequently acknowledged than other non-pharmacological approaches like occupational therapy.
There is a gap between evidence supporting music interventions and their inclusion in policy.
Abstract
Objectives: Dementia prevalence continues to rise, predicted to reach 150 million by 2050, making development of effective, person-centred, non-pharmacological interventions an urgent healthcare priority. Music therapy and music (MTAM) are increasingly recognised as low-cost options to alleviate behavioural and psychological symptoms of dementia (BPSD), particularly in acute hospital environments. This scoping review evaluates national dementia strategies and clinical practice guidelines (CPGs) to determine how far MTAM are acknowledged as formal components of dementia care. Methods: A scoping review of databases identified the most recent national clinical strategies or CPGs for people with dementia (PWD), published between 2015 and 2025. Using the PRISMA guidelines in June 2025, with pre-determined inclusion and exclusion criteria we examined four databases, supplemented with an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
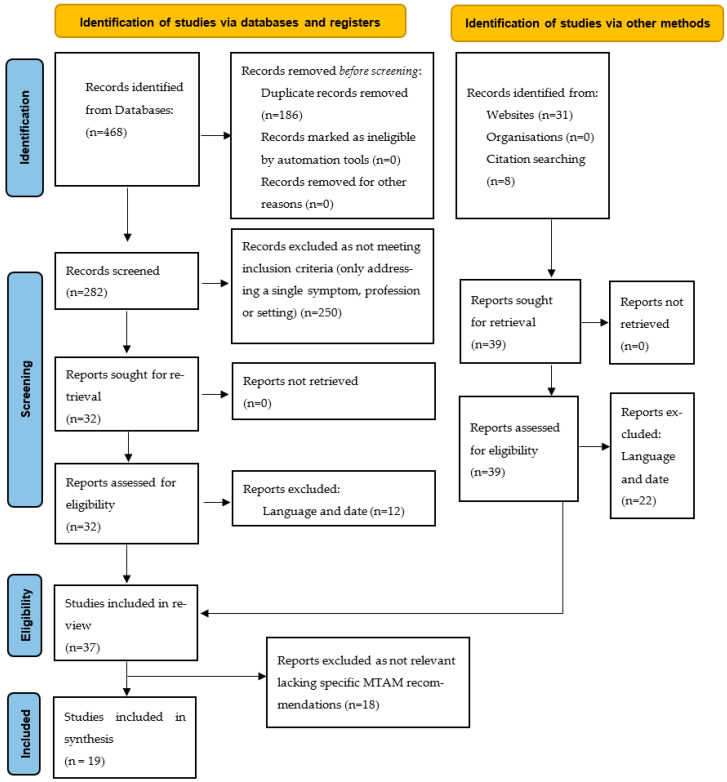 Figure 1
Figure 1- —Health Education England and NIHR Bridging Post-doctoral Award
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusic Therapy and Health · Dementia and Cognitive Impairment Research · Intensive Care Unit Cognitive Disorders
1. Introduction
Dementia prevalence is rapidly rising; currently it is estimated that over 55 million people have dementia, and this is predicted to increase to over 130 million cases by 2050 [1]. Dementia is a leading cause of impairment and loss of dependence in adults, affecting cognitive function, mood, ability to perform activities of daily living and independence. Despite advances in research and optimistic future treatments, there is no cure, making strategies to support quality of life, person-centred care and symptom management a global healthcare priority.
The World Health Organization recognizes that dementia is not a single diagnosis or disease but a conceptual term for a syndrome that accompanies a range of neurodegenerative diseases that over time destroys nerve cells, damages the brain, leads to cognitive impairment and affects activities of daily living [2]. Alzheimer’s Disease (AD) is the most common subtype [3], followed by vascular dementia, with Lewy Body dementia (LBD) and Frontal Temporal Dementia (FTD) accounting for a smaller proportion of cases [3,4]. People with dementia (PWD) frequently require hospital care, where unfamiliar environments can exacerbate confusion, anxiety and collectively known as behavioural and psychosocial symptoms of dementia (BPSD) [5]. These behaviours complicate treatment, extend hospital stays and increase healthcare costs [5,6,7,8].
Over the past two decades, there has been a shift away from pharmacological management of BPSD due to limited efficacy and well-documented risks, including increased falls, stroke and mortality [9,10,11,12]. Consequently, clinical guidance now emphasises person-centred, non-pharmacological interventions as first-line approaches [13,14,15,16]. Among these, music therapy and music-based interventions (MTAMs) have gained increasing attention. Music therapy is a recognised clinical intervention delivered by trained professionals, while structured and informal music interventions may also be implemented by caregivers following appropriate training [17,18].
Evidence suggests that MTAM can reduce anxiety and distress, enhance engagement, and support emotional and cognitive functioning in PWD [19,20,21,22]. Although much of the literature focuses on community and residential care settings, there is growing interest in the potential role of MTAM within acute and hospital-based care environments. National dementia strategies and clinical practice guidelines (CPGs) play a critical role in translating such evidence into policy and practice, shaping care delivery and resource allocation.
However, it remains unclear to what extent MTAM are explicitly recognised or recommended within national dementia strategies and dementia CPGs, particularly in relation to acute care. The purpose of this scoping review was therefore to map the inclusion of MTAM within current national dementia strategies and clinical practice guidelines, with a specific focus on their role in supporting person-centred care for people with dementia in acute healthcare settings.
We chose to conduct a scoping review because the available evidence, guidelines and national strategies had not previously been delineated with reference to MTAM. This follows a systematic approach to delineate the extent of the evidence in the literature with the aim of identifying the primary concepts and disparities in knowledge. This review seeks to determine how prominently MTAM features within current national dementia strategies and dementia CPGs, in particular in acute care. This is with a view to raising awareness for those working with PWD in acute healthcare settings of the benefits of using MTAM to alleviate distress and anxiety.
2. Materials and Methods
The reporting of this scoping review was guided by the standards of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement [23] and followed the PRISMA ScR guidelines [24]. A protocol for this scoping review is available on Open Science Framework, https://osf.io/4upj7/ (accessed on 1 July2025).
This scoping review of national dementia strategies and CPGs was carried out in June 2025. We used a triple search approach. Firstly, four databases were searched (CINHAL, EMBASE, Medline, PsychINFO) with the search terms (see below). To identify further material, an internet search engine, Google, performed targeted searches using specific country names paired with key search terms from the database search list. Thirdly, “reference snowballing” was used; guidelines and frameworks mentioned in other reports, such as those found via Alzheimer’s Europe and other government health ministries, were followed.
The terms used for the database search were as follows:
“Dementia”
“Guideline*”
“Clinical practice guideline”
“Strategy”
“National strategy”
“Action plan”
Inclusion criteria for guidelines were as follows:
- Worldwide national-level guidelines or strategies applicable to dementia care (including guidelines that span multiple neighbouring countries and ones for independently governed Overseas Territories).
- Published or updated since 2015.
- Addressed dementia care comprehensively (not limited to a single symptom, profession or setting).
- Endorsed by a national government, professional body or healthcare authority.
- Legally able to be translated into practice.
Guidelines were excluded under the following criteria:
- Focused only on mild cognitive impairment.
- Exclusive recommendations for one issue (e.g., pain, wandering, diagnosis).
- Directed solely at one healthcare practitioner (e.g., radiographers, medics or nurses).
The search was limited to guidelines published in English (or with an official translation available, no AI technology was used). Both authors screened the identified strategies and guidelines for inclusion. No disagreements occurred, strategies not meeting criteria (symptom profession or setting) were easily identifiable. An assessment of quality was not within the scope of this review due to the nature of the material not being primary research. Results were tabulated on the basis on inclusion of MTAM and acute care, it was also noted if other non-pharmacological therapies were included. Studies meeting the inclusion criteria were examined further by author one, and data extracted and tabulated based on the details of inclusion of MTAM and the key findings of each were checked by the second author.
3. Results
A total of 37 national dementia strategies and/or dementia clinical practice guidelines from 31 countries were identified. Twelve were excluded because they were not available in English, four excluded because they did not meet the date criteria and two excluded as not deemed relevant. The 19 meeting the inclusion criteria came from 16 countries. The process of study identification is illustrated in a modified PRISMA flow diagram (Figure 1). PRISMA checklist is shown in [25].
As of June 2025, the following countries do not have publicly accessible National Dementia strategies or plans freely accessible: Belgium-Wallonia, Bosnia and Herzegovina, Bulgaria, Cyprus, Estonia, Hungary, Jersey, Latvia, Lithuania, Montenegro, North Macedonia, Poland, Romania, Serbia, Slovakia, Turkey, Ukraine (Alzheimer Europe [26]).
Many guidelines were excluded as they did not describe multifaceted approaches, focusing instead on narrow domains or single issues within dementia care, for example, palliative care or pain management. Some did not relate to dementia care, hence the limited number of accessed and included strategies. The included CPG and strategies are shown in Table 1.
The details of the seven strategies/guidelines from six countries are shown in Table 2.
4. Discussion
This review demonstrates that despite the strong shared commitment of national dementia strategies to person-centred, ethical and non-pharmacological care, there is limited recognition of MTAM within these policy frameworks. Of the nineteen meeting the inclusion criteria only seven strategies promoted MTAM for PWD. Despite robust alignment on principles such as dignity, autonomy, empowerment and holistic care for PWD, MTAM remain under-represented in national strategies and CPGs compared with other non-pharmacological approaches.
The findings of this review should be considered in the context of the broader evidence base for MTAM across neurological populations. Music engages preserved neural networks involved in emotion, memory and attention, which may explain its capacity to reduce anxiety, agitation and distress even in advanced neurodegenerative conditions [46]. These mechanisms are particularly relevant to people with dementia, for whom familiar sensory stimuli can support communication, emotional regulation and person-centred care in environments that are otherwise disorientating, such as acute hospital settings.
4.1. Areas of Consensus
Within the included documents there was overall consensus on maintaining the dignity and empowerment of PWD, promoting equality and human rights. PWD should be involved in decisions about their care with the best information and advocacy. Emphasis was universally placed on the need for education to reduce stigma and improve public awareness, to inform of risks and possible prevention strategies. Most guidelines promoted dementia-friendly communities where individuals with dementia and their families can participate in a dementia-friendly society, living active and meaningful lives.
Living well with dementia needs person-centred, holistic and coordinated care; this takes work force development and training. Specific support for individuals with dementia and their carers, who are taking most of the burden, should be a routine part of a dementia diagnosis. Many guidelines promoted living at home for as long as possible, reducing burden on residential care. To support carers in this, strategies agreed that community engagement and continuous assessment were critical.
All plans noted the need for training and workforce development. Capacity should be built into health and social care for the future challenges of increasing numbers of PWD. Recognition that dementia is individual and unpredictable, both at a daily level and in its trajectory, requires training in the changing nature of support and care needed. Most guidelines and CPGs supported the need for gathering dementia data and increased research and innovation.
The strong emphasis across national strategies on dignity, autonomy, empowerment and person-centred care aligns closely with the proposed mechanisms of MTAM. By facilitating emotional expression, social connection and meaningful engagement, MTAM practically places these ethical principles in everyday care. The limited explicit reference to MTAM within guidelines represents a missed opportunity to translate widely endorsed values into practical, evidence-informed interventions.
4.2. Music Therapy and Music
The focus of this review was to assess the inclusion of MTAM in national guidelines and CPGs as a method of supporting management and person-centred care of PWD. Despite the shared values and consensus, this review found there were significant gaps in how national plans incorporate MTAM. Nearly all of the included guidelines recognised the need for non-pharmacological interventions, and many other therapies were supported as alternative practice in social and health care environments. However, MTAM were rarely acknowledged in detail; seven out of the nineteen included strategies referred briefly to music. Playlist for Life [47] was mentioned in two plans (Belgium and Scotland [30,44]); however, in one case this was more in the context of raising the profile of the individual with dementia rather than as a therapy to aid care.
Further evidence to support the inclusion of MTAM in national strategies comes from other neurological populations. MT has demonstrated beneficial effects across a range of neurological disorders, including improvements in emotional wellbeing, anxiety, sleep, cognitive function and quality of life [48,49]. There are emerging delivery models, such as telecoaching and teletherapy which support adherence, physical functioning and engagement in care, that could be transferable to acute care situations [50]. This cross-condition applicability and feasibility of music-based interventions in complex neurological populations strengthens their case for inclusion in dementia strategies and CPGs, particularly given the shared challenges related the cognitions mental health and functional decline.
Few strategies linked MTAM to acute care, and hospital-based care was covered in only half the included plans. This highlights the need for national strategies to recognise that given the age demographic of PWD, they are more likely to present at acute and emergency care and need support. Research is also clear on the effects of hospitalisation on PWD: increased anxiety, non-compliance and poorer outcomes, with longer hospital stays or mortality often the consequence.
Evidence from both dementia and wider neurological populations suggests that MTAM can support emotional well-being, reduce anxiety and enhance engagement through activation of preserved musical memory and affective processing pathways [21,51,52]. While much of the dementia literature has focused on residential and community settings, emerging evidence from acute care indicates that MTAM may also improve care processes, including reduced resistance to care and enhanced patient–staff interaction [53]. These mechanisms are particularly relevant in hospital environments, where sensory overload and unfamiliar routines commonly exacerbate behavioural and psychological symptoms of dementia.
The distinction between formal music therapy delivered by registered professionals and informal music-based interventions facilitated by trained staff or caregivers has important implications for policy and implementation [17]. A tiered approach, in which professional music therapy is available for individuals with complex needs alongside structured, staff-led music interventions embedded in routine care, may enhance feasibility and equity. However, national strategies and CPGs rarely provide guidance on how such models could be implemented, contributing to variability in practice.
4.3. Dementia Subtypes
Whilst there is much research on “AD only” and “all dementia” cohorts, there is relatively less specifically for LBD or FTD. These subtypes present with distinct cognitive, behavioural and sensory features that may influence how individuals respond to interventions such a MTAM. The under-representation of rarer subtypes in MTAM research reflects well-recognised methodological and ethical challenges, including small population sizes and difficulties in recruitment [54,55,56]. This may partly explain the reluctance of policymakers to include MTAM in national guidelines intended to be broadly applicable. Importantly, interventions aimed at reducing distress and supporting emotional well-being may be relevant across dementia subtypes, despite differences in cognitive or behavioural presentation.
This review highlights the importance of recognizing and reporting dementia sub-type when designing and conducting research. Ensuring adequate representation across the dementia subtypes will allow findings to be more inclusive, applicable and evidence-based to support the care of all PWD.
4.4. Barriers to the Use of Music Therapy and Music Interventions
Encouragingly, most CPG and national strategies acknowledge the limited benefits of drug therapies for the BPSD and the risks associated with using them and ask for more support for non-pharmacological interventions. The Canadian dementia strategy [31,32] calls for more support for non-drug therapies and names MT as a promising approach, yet there are barriers to implementing MTAM in acute care. Staff shortages, time pressures and limited access to training are all routine occurrences in these environments and more generally over all hospitals. The call for increased training in dementia was universal in all the included CPG and national strategies. As dementia is recognized and stigma reduced, there is a need to increase support, skills training and education across all areas caring for PWD.
Although MTAM are relatively low-cost and low-risk interventions, their implementation in acute care settings is constrained by systemic factors, including time pressures, staffing limitations, and limited access to specialist training. The absence of clear policy endorsement may further impede uptake, particularly in settings dominated by biomedical models of care. Without explicit guidance within national strategies and CPGs, MTAM risk being perceived as optional rather than integral to high-quality dementia care.
Increasingly, hospitals are recognizing the value of multi-professional teams; collaborations within these healthcare teams are leading to improvements in standards of care, particularly with vulnerable patient groups like PWD, yet the prevailing medical dominance, the perceived view that physicians’ viewpoints are prioritized over those of allied health professionals, nurses or other health professionals, can result in slow adoption of non-medical interventions. This applies both in hospitals and in government policies. Strengthening interdisciplinary collaboration and recognising the expertise of allied health professionals are critical to advancing the integration of MTAM into routine practice. As healthcare systems increasingly adopt team-based models of care, formal recognition of music therapy and music-based interventions within policy frameworks could support cultural change and facilitate broader implementation.
MTAM and other therapies will continue to build evidence-based results to support the care of PWD, and as parity of clinical expertise recognized, we have confidence that these therapies will be adopted at administrative and policy level. Although the economic benefits of using MTAM and other therapies to reduce BPSD in acute care makes a strong case for its inclusion in national and local guidance, the most powerful argument is the benefit to caring for PWD.
4.5. Limitations and Strengths
This review of the inclusion of MTAM in national dementia guidelines, frameworks and strategies has several limitations which should be considered when interpreting the findings. Guidelines were only selected from those either freely available in English or where a translation existed, and some translations were abbreviated compared to the source document. While this ensured consistency of analysis and transparency, it may have resulted in the exclusion of relevant policy documents published solely in national languages. Consequently, some countries with well-developed dementia frameworks may be underrepresented and the absence of MTAM interventions in certain strategies should not be interpreted as evidence that such approaches are not recognised or used in practice.
National strategies might also be limited in what information they included, and it is possible that sub-national strategies might specifically address the use of music. As a result, this review may underestimate the extent to which non-pharmacological interventions, including MTAM, are embedded in local or service-level practice.
The notable absence of Low- and Middle-Income Countries (LMICs) in this scoping review likely reflects wider structural and systemic barriers in research capacity, health system infrastructure and policy prioritisation in these settings, rather than lack of need. Many LMICs face constrained funding and resources for public health research, making it difficult to generate evidence to drive national dementia strategies and policy development. Nationally representative data on dementia prevalence, costs, and effective interventions can be sparse or methodologically limited. Additionally, competing health priorities can reduce political impetus for formal national plans, particularly when other communicable and non-communicable diseases dominate the policy agenda. These factors contribute to the observed absence of LMIC representation in the dementia strategy literature and to a generally fragmented research base on mental health issues among older adults [57].
The analysis also focused on whether MTAM were mentioned, and it was not within the scope to evaluate the depth, quality or implementation of those recommendations. This approach is consistent with the scoping review objective, mapping the presence or absence of interventions across policy documents, rather than appraising policy quality or effectiveness. Finally, although emergency and acute care were of key interest, many national strategies do not differentiate care settings, and this may limit the specificity of conclusions for hospital-based practice.
Alongside these limitations, this a review has several important strengths. The use of a scoping review methodology enabled a systematic and transparent mapping of the presence of MTAM across a diverse range of national dementia strategies and CPGs. This allowed mapping of heterogeneous evidence to clarify key concepts, identify gaps in knowledge and capture policy level patterns that are not accessible through effectiveness-focused reviews. By examining international frameworks and explicitly considering care settings, acknowledging dementia subtypes and non-pharmacological interventions, this review provides a novel, policy-relevant contribution and establishes a robust foundation for future research, implementation studies and guideline development in this emerging area.
4.6. Future Research Directions
Future research should focus on strengthening the evidence base for MTAM across the dementia spectrum, with particular attention to under-represented dementia subtypes and acute hospital settings. Longitudinal and comparative studies are needed to examine clinical, psychosocial and economic outcomes, as well as implementation feasibility within complex care environments. In parallel, policy-focused research exploring how MTAM can be translated into national frameworks, and CPGs will be essential to support equitable, scalable and sustainable integrations into dementia care.
5. Conclusions
MTAM is a promising non-pharmacological intervention for managing BPSD, offering safer alternatives to antipsychotic medications, which carry significant risks in older adults. Despite strong evidence of benefit, MTAM is rarely included in national dementia strategies or clinical guidelines and is especially under-represented in acute care settings where distress, agitation and non-compliance are common. MTAM interventions can support person-centred care, reduce anxiety, improve mood, strengthen identity and help maintain dignity—key ethical priorities across all international dementia care guidelines. Implementation barriers persist in acute environments; staff shortages, time limitations and lack of training often prevent use of MTAM, despite its potential to reduce distress and shorten hospital stays.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization A Blueprint for Dementia Research 2022 Available online: https://www.who.int/publications/i/item/9789240058248(accessed on 1 August 2025)
- 2World Health Organization Dementia Available online: https://www.who.int/news-room/fact-sheets/detail/dementia(accessed on 1 August 2025)
- 3Goodman R.A. Lochner K.A. Thambisetty M. Wingo T.S. Posner S.F. Ling S.M. Prevalence of dementia subtypes in United States Medicare fee-for-service beneficiaries, 2011–2013 Alzheimer’s Dement.201713283710.1016/j.jalz.2016.04.00227172148 PMC 5104686 · doi ↗ · pubmed ↗
- 4Wu Y.T. Beiser A.S. Breteler M. Fratiglioni L. Helmer C. Hendrie H.C. Honda H. Ikram M.A. Langa K.M. Lobo A. The changing prevalence and incidence of dementia over time—Current evidence Nat. Rev. Neurol.201713273910.1038/nrneurol.2017.6328497805 · doi ↗ · pubmed ↗
- 5Sinvani L. Strunk A. Ardito S. Gordon S. Liu Y. Schantz E. Arroon A. Ilyas A. Gromova V. Polokowski A. Reducing Behavioral and Psychological Symptoms of Dementia in Acutely Ill Patients via Patient Engagement Specialists: A Pilot Feasibility Study Gerontol. Geriatr. Med.202392333721423119216210.1177/2333721423119216237601321 PMC 10439723 · doi ↗ · pubmed ↗
- 6Johnston M. Wakeling A. Graham N. Stokes F. Cognitive impairment emotional disorder and length of stay of elderly patients in a district general hospital Br. J. Med. Psychol.20116013313910.1111/j.2044-8341.1987.tb 02723.x 3620390 · doi ↗ · pubmed ↗
- 7Fogg C. Griffiths P. Meredith P. Bridges J. Hospital outcomes of older people with cognitive impairment: An integrative review Int. J. Geriatr. Psychiatry 2018331177119710.1002/gps.491929947150 PMC 6099229 · doi ↗ · pubmed ↗
- 8Sommerlad A. Perera G. Mueller C. Singh-Manoux A. Lewis G. Stewart R. Livingston G. Hospitalisation of people with dementia: Evidence from English electronic health records from 2008 to 2016 Eur. J. Epidemiol.20193456757710.1007/s 10654-019-00481-x 30649705 PMC 6497615 · doi ↗ · pubmed ↗