Factors Influencing Patient Preference for Surgical Intervention Versus Medical Therapy Among Cambodian Adults With Advanced Glaucoma: A Health Belief Model-Based Analysis
Channdarith Kith, Amarin Mar, Piseth Kong, Bunseng Sea, Kossama Chukmol, Ratneary Hav, Saly Saint

TL;DR
This study explores why Cambodian adults with advanced glaucoma prefer surgery or medical treatment, using a psychological model to identify key influencing factors.
Contribution
The study applies the Health Belief Model to understand treatment preferences for glaucoma in a low-resource setting like Cambodia.
Findings
Only 28.13% of participants preferred surgical intervention over medical therapy.
Perceived benefits, severity, and self-efficacy were strong predictors of surgical preference.
Low perceived barriers and higher knowledge scores were associated with a preference for surgery.
Abstract
Objectives Glaucoma is the major cause of irreversible blindness globally and ranks as the sixth leading cause of avoidable blindness in Cambodia. Recent advancements in glaucoma treatment techniques have emerged; yet, patient treatment preferences, particularly within low-resource environments, remain poorly understood. We are using the Health Belief Model (HBM) to identify factors that influence the preference for surgical versus medical therapy in adults with advanced glaucoma in Cambodia. Methods A hospital-based cross-sectional study was conducted at Preah Ang Duong Hospital, Phnom Penh, Cambodia, between January and June 2024. A structured, validated questionnaire evaluated sociodemographic characteristics, clinical data, glaucoma awareness, and HBM constructs (susceptibility, severity, benefits, barriers, self-efficacy, and cues to action). Logistic regression was used to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
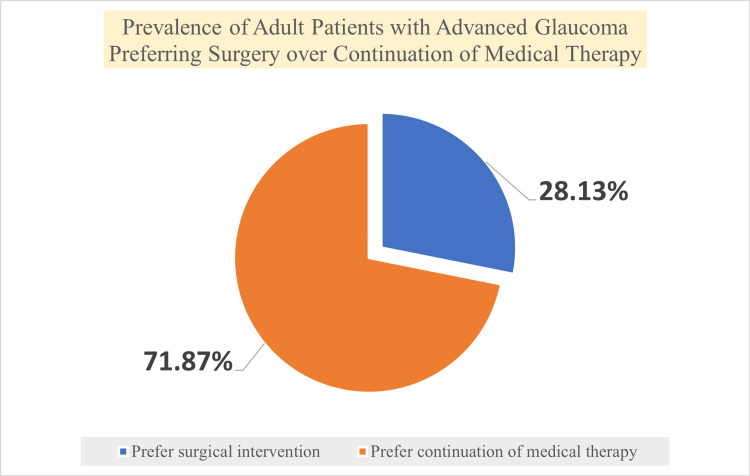 Figure 1
Figure 1| Demographic data | Description | |
| n | Percentage | |
| Gender | ||
| Male | 248 | 50.92% |
| Female | 239 | 49.08% |
| Age (mean±SD) | ||
| ≤40 | 106 | 21.77% |
| 41-50 | 76 | 15.61% |
| 51-60 | 131 | 26.90% |
| 61-70 | 125 | 25.67% |
| 70+ | 49 | 10.06% |
| Education level | ||
| University graduate | 72 | 14.78% |
| High school | 277 | 56.88% |
| Secondary school | 79 | 16.22% |
| Primary school | 51 | 10.47% |
| Illiterate | 8 | 1.64% |
| Job status | ||
| Employed | 316 | 64.89% |
| Unemployed | 60 | 12.32% |
| Retired | 99 | 20.33% |
| Others | 12 | 2.46% |
| Residence | ||
| Urban | 212 | 43.53% |
| Rural | 275 | 56.47% |
| Type of payment | ||
| Indigent | 23 | 4.72% |
| Paying | 126 | 25.87% |
| Health Equity Fund | 109 | 22.38% |
| National Social Security Fund | 229 | 47.02% |
| Clinical data | Description | |
| n | Percentage | |
| Type of glaucoma | ||
| Open-angle glaucoma | 185 | 37.99% |
| Angle-closure glaucoma | 153 | 31.42% |
| Uveitic or inflammatory glaucoma | 67 | 13.76% |
| Others (neovascular glaucoma, etc.) | 50 | 10.27% |
| Angle recession or post-trauma glaucoma | 14 | 2.87% |
| Pseudo-exfoliative glaucoma | 10 | 2.05% |
| Lens-related glaucoma | 8 | 1.64% |
| Years of treatment | ||
| <5 | 455 | 93.43% |
| ≥5 | 32 | 6.57% |
| No. of drugs used | ||
| 1 | 130 | 26.69% |
| 2 | 110 | 22.59% |
| 3 | 106 | 21.77% |
| More than 3 | 141 | 28.95% |
| Type of surgical procedures | ||
| Glaucoma tube implant | 3 | 0.62% |
| Others (phaco-goniosynechialysis, etc.) | 35 | 7.19% |
| Trabeculectomy +/- mitomycin-C | 91 | 18.69% |
| None | 358 | 73.51% |
| Other comorbidities | ||
| Hypertension | 259 | 53.18% |
| Cataract | 154 | 31.62% |
| Diabetes | 102 | 20.94% |
| Dyslipidemia | 38 | 7.80% |
| Ischemic heart disease | 36 | 7.39% |
| Obesity | 31 | 6.37% |
| Hypothyroidism | 10 | 2.05% |
| Asthma | 3 | 0.62% |
| Renal disease | 2 | 0.41% |
| Others | 2 | 0.41% |
| Do you prefer surgical treatment over continuation of medical therapy? | ||||
| Yes (n=137; 28.13%) | No (n=350; 71.87%) | |||
| Patient's knowledge | U | P-value | ||
| Total score: mean±SD | 5.80±1.61 | 5.41±1.72 | 21221 | 0.048 |
| %score: mean±SD | 58.03±16.13 | 54.09±17.17 | ||
| Do you prefer surgical treatment over continuation of medical therapy? | ||||
| Yes (n=137; 28.13%) | No (n=350; 71.87%) | |||
| Health Belief Model | U | P-value | ||
| (1) Perceived seriousness | ||||
| Total score: mean±SD | 8.42±1.73 | 3.20±0.85 | 2457 | <0.00001 |
| %score: mean±SD | 93.59±19.23 | 35.56±9.44 | ||
| (2) Perceived susceptibility | ||||
| Total score: mean±SD | 8.45±1.54 | 3.43±1.10 | 2118 | <0.00001 |
| %score: mean±SD | 93.84±17.15 | 38.13±12.27 | ||
| (3) Perceived benefits | ||||
| Total score: mean±SD | 11.07±1.69 | 6.16±2.28 | 3216 | <0.00001 |
| %score: mean±SD | 92.21±14.05 | 51.33±19.01 | ||
| (4) Perceived barriers | ||||
| Total score: mean±SD | 9.61±3.23 | 13.23±2.27 | 9241 | <0.00001 |
| %score: mean±SD | 19.01±21.53 | 88.23±15.13 | ||
| (5) Self-efficacy | ||||
| Total score: mean±SD | 7.99±1.79 | 4.07±1.53 | 4149 | <0.00001 |
| %score: mean±SD | 88.73±19.94 | 45.27±17.01 | ||
| Preferring surgery | Not preferring surgery | Total | Chi-square | P-value | ||
| Do you have a family member or a friend who lost vision from glaucoma in spite of the use of medication? | Yes | 89 | 180 | 269 | 7.2949 | 0.007 |
| No | 48 | 170 | 218 | |||
| Do you have family members or friends who went for successful glaucoma surgery? | Yes | 89 | 196 | 285 | 3.2589 | 0.071 |
| No | 48 | 154 | 202 | |||
| Does your doctor prompt surgery than medication? | Yes | 107 | 270 | 377 | 0.0518 | 0.821 |
| No | 30 | 80 | 110 | |||
| Did you get any information from media or social contacts that encourage surgery? | Yes | 77 | 169 | 246 | 2.4698 | 0.116 |
| No | 60 | 181 | 241 | |||
| Demographic and clinical characteristics | Preferring surgery (n=137; 28.13%) | Not preferring surgery (n=350; 71.87%) | Chi-square | P-value | ||
| n | Percentage | n | Percentage | |||
| Gender | ||||||
| Male | 63 | 45.99% | 176 | 50.29% | 0.7286 | 0.393 |
| Female | 74 | 54.01% | 174 | 49.71% | ||
| Education level | ||||||
| University graduate | 20 | 14.60% | 52 | 14.86% | 6.5875 | 0.159 |
| High school | 89 | 64.96% | 188 | 53.71% | ||
| Secondary school | 15 | 10.95% | 64 | 18.29% | ||
| Primary school | 11 | 8.03% | 40 | 11.43% | ||
| Illiterate | 2 | 1.46% | 6 | 1.71% | ||
| Job status | ||||||
| Employed | 87 | 63.50% | 229 | 65.43% | 1.1709 | 0.761 |
| Unemployed | 18 | 13.14% | 42 | 12% | ||
| Retired | 30 | 21.90% | 69 | 19.71% | ||
| Others | 2 | 1.46% | 10 | 2.86% | ||
| Residence | ||||||
| Urban | 52 | 37.96% | 160 | 45.71% | 2.4108 | 0.121 |
| Rural | 85 | 62.04% | 190 | 54.29% | ||
| Type of payment | ||||||
| Indigent | 6 | 4.38% | 17 | 4.86% | 2.4456 | 0.485 |
| Paying | 35 | 25.55% | 91 | 26% | ||
| Health Equity Fund | 25 | 18.25% | 84 | 24% | ||
| National Social Security Fund | 71 | 51.82% | 158 | 45.14% | ||
| Type of glaucoma | ||||||
| Open-angle glaucoma | 49 | 35.77% | 136 | 38.86% | 17.0882 | 0.009 |
| Angle-closure glaucoma | 59 | 43.07% | 94 | 26.86% | ||
| Uveitic or inflammatory glaucoma | 17 | 12.41% | 50 | 14.29% | ||
| Others (neovascular glaucoma, etc.) | 7 | 5.11% | 43 | 12.29% | ||
| Angle recession or post-trauma glaucoma | 1 | 0.73% | 13 | 3.71% | ||
| Pseudo-exfoliative glaucoma | 2 | 1.46% | 8 | 2.29% | ||
| Lens-related glaucoma | 2 | 1.46% | 6 | 1.71% | ||
| Type of surgical procedures | ||||||
| Glaucoma tube implant | 3 | 2.19% | 0 | 0% | 0.5072 | 0.776 |
| Others (phaco-goniosynechialysis, etc.) | 32 | 23.36% | 3 | 0.86% | ||
| Trabeculectomy +/- mitomycin-C | 81 | 59.12% | 10 | 2.86% | ||
| None | 21 | 15.33% | 237 | 67.71% | ||
| Univariate | Multivariate | |||
| OR (95% CI) | P-value | OR (95% CI) | P-value | |
| Health Belief Model domains | ||||
| Perceived seriousness | 1.64 (1.15 to 2.33) | 0.006 | 1.71 (1.17 to 2.51) | 0.008 |
| Perceived susceptibility | 1.38 (0.95 to 2.01) | 0.082 | 1.34 (0.91 to 1.99) | 0.129 |
| Perceived benefits | 1.50 (1.17 to 1.92) | 0.001 | 1.51 (1.16 to 1.94) | 0.001 |
| Perceived barriers | 0.64 (0.52 to0.79) | <0.001 | 0.61 (0.49 to 0.77) | <0.0001 |
| Self-efficacy | 1.45 (1.10 to 1.89) | 0.007 | 1.46 (1.11 to 1.93) | 0.006 |
| Gender | ||||
| Male | 1* | 1* | ||
| Female | 1.19 (0.79 to 1.76) | 0.394 | 1.81 (0.54 to 6.16) | 0.337 |
| No. of drugs | 1.05 (0.90 to 1.23) | 0.515 | 0.78 (0.48 to 1.26) | 0.313 |
| Level of knowledge | 1.15 (1.02 to 1.29) | 0.022 | 1.36 (0.91 to 2.01) | 0.135 |
| Age | 1.02 (1.00 to 1.02) | 0.038 | 1.01 (0.97 to 1.05) | 0.484 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Impairment Studies · Glaucoma and retinal disorders · Intraocular Surgery and Lenses
Introduction
Glaucoma is the leading cause of irreversible blindness globally, and it is becoming a major public health concern, particularly among the elderly population. In 2020, glaucoma accounted for over 11% of worldwide blindness in those aged 50 and above, with an estimated 3.6 million individuals becoming blind from the condition [1,2]. In Cambodia, national data from the Rapid Assessment of Avoidable Blindness (RAAB) reveal that glaucoma is one of the primary causes of irreversible blindness [3], but its actual prevalence is probably underestimated due to underdiagnosis [4,5].
Reducing intraocular pressure is the main objective of glaucoma treatment to stop further optic nerve damage and loss of visual field [6,7]. Although medical therapy is usually used as the first-line treatment, surgical intervention is often recommended for advanced cases to attain long-term pressure control and decrease reliance on medication [8,9]. In our clinical setting, even at advanced stages, many patients still prefer lifetime medical therapy despite evidence that surgical management is effective.
Patient treatment preference is widely acknowledged as a vital factor influencing adherence, satisfaction, and long-term outcomes. The Health Belief Model (HBM) offers a theoretical framework for comprehending health-related decision-making through the analysis of perceived susceptibility, severity, benefits, barriers, cues to action, and self-efficacy [10]. The HBM has been extensively used to analyze the behaviors of chronic diseases, but it has not been generally applied to glaucoma treatment preferences, especially in settings with limited resources such as Cambodia.
Thus, this study aimed to examine both clinical and psychosocial factors associated with patient preference for surgical intervention compared with medical therapy among Cambodian adults with advanced glaucoma, guided by the HBM.
Materials and methods
Study design and setting
This cross-sectional analytical study was conducted in the Department of Ophthalmology, Preah Ang Duong Hospital, Phnom Penh, Cambodia. As the national tertiary referral center for ophthalmology, Preah Ang Duong Hospital serves patients from all provinces via direct self-referral, non-governmental eye care programs, and public hospitals. The study was conducted over a six-month duration, spanning from January 1 to June 30, 2024.
Study population and eligibility criteria
Participants included adult patients aged 18 years or older who had a confirmed diagnosis of advanced glaucoma in at least one eye. Advanced glaucoma was characterized in accordance with the European Glaucoma Society criteria as the presence of glaucomatous optic neuropathy accompanied by corresponding visual field defects affecting both hemifields or having loss within 5 degrees of fixation on standard automated perimetry.
Exclusion criteria for patients were the presence of secondary glaucoma (neovascular, uveitic, steroid-induced, or traumatic), previous bilateral glaucoma surgery, complete blindness due to glaucoma, significant ocular comorbidities impacting visual function (e.g., advanced diabetic retinopathy or macular degeneration), cognitive impairment that impaired reliable interview responses, and refusal to provide informed consent.
Sample size determination
The required sample size was calculated using Cochran's formula for cross-sectional studies. Based on an estimated proportion of 45.9% preference for surgical intervention, which represents the primary outcome of interest in this study, a 95% confidence level, and a margin of error of 5%, the minimum required sample size is determined to be 381 participants. A target sample size of at least 419 participants was established after accounting for an expected non-response rate of 10%. Eligible patients attending the glaucoma clinic were consecutively recruited during the study period until the necessary sample size was reached.
Although the primary objective of this study was to identify the association with treatment preference, the sample size was calculated based on the estimated prevalence of preference for surgical intervention, as this was the key outcome variable in this cross-sectional analytical study. This approach is consistent with sample size estimation for studies examining associations with a binary outcome in similar settings.
Sampling technique
A consecutive sampling approach was employed, and all eligible patients attending the glaucoma outpatient clinic throughout the study period were invited to participate. Recruitment occurred daily until the target sample size was achieved.
Data collection procedures
Data were gathered via structured face-to-face interviews and the examination of medical records. Interviews were not audio-recorded; responses were documented in real time using structured questionnaires by trained interviewers in a private room at the outpatient department to guarantee participant comfort and confidentiality. The research team used a standardized data collection form to gather clinical data from patient records.
Study instruments and measurements
Sociodemographic and Clinical Characteristics
Data regarding age, sex, residence, educational level, occupation, health insurance status, duration of glaucoma diagnosis, type of glaucoma, number of prescribed antiglaucoma medications, and history of previous ocular surgery were gathered.
Assessment of Glaucoma Knowledge
A 10-item questionnaire based on previously validated tools was used to measure knowledge of glaucoma. Items measured knowledge of the chronicity of the condition, blindness risk, intraocular pressure control, treatment objectives, and the need for long-term monitoring. Each correct response received one point, and total scores were converted to percentage scores. Higher scores reflect an improved understanding of glaucoma.
HBM Constructs
Health beliefs were evaluated through items derived from the HBM, encompassing perceived susceptibility, perceived severity, perceived benefits of surgery, perceived barriers to surgery, self-efficacy, and cues to action. A five-point Likert scale, spanning from strongly disagree to strongly agree, was used for measuring responses. A composite score was given to each construct, with higher scores meaning more support for the belief in question.
Outcome Variable
The main outcome variable was patient preference regarding glaucoma treatment, classified as preference for surgical intervention or preference for ongoing medical therapy. Preference was measured by asking individuals explicitly which treatment they would select if their ophthalmologist advised it, with the assumption that surgery would primarily try to control disease progression rather than restore lost eyesight.
Data Quality Assurance
To ensure content and face validity, the questionnaire was developed based on previously validated instruments and reviewed by three glaucoma specialists and two public health researchers. The questionnaire was translated into Khmer and back-translated into English by independent bilingual translators to ensure linguistic and conceptual equivalence (Appendices).
A pilot study was conducted to assess clarity, feasibility, and internal consistency. Based on pilot testing, minor wording adjustments were made to improve comprehension. The internal consistency of the HBM constructs demonstrated acceptable reliability (Cronbach's alpha >0.70 for all domains).
Data collectors underwent standardized training prior to the start of the study. Daily reviews of completed questionnaires were conducted to ensure completeness and consistency. Double data entry was carried out to reduce transcription errors. Incomplete or missing responses were handled using listwise deletion or multiple imputation, ensuring that analyses included only complete data for each construct.
Statistical analysis
Data were input into a secure database and analyzed using Stata Version 14.2 (StataCorp LLC, College Station, Texas, United States). Descriptive statistics summarized participant characteristics and study variables. Continuous variables were evaluated for normality and summarized using means with standard deviations or medians with interquartile ranges, as applicable. Categorical variables were presented as frequencies and percentages. Bivariate analyses used chi-squared tests for categorical variables and independent-samples t-tests for continuous variables to compare participants who preferred surgery with those who preferred medical treatment. Variables that had a p-value less than 0.20 in the bivariate analysis were included in more complex models to identify factors that independently influenced the choice of surgical intervention. Adjusted odds ratios (aORs) accompanied by 95% confidence intervals (CIs) were presented. Statistical significance was set at a two-sided p-value of <0.05.
Ethical approval and informed consent
The study protocol received review and approval from the National Ethics Committee for Health Research of the Ministry of Health (MoH) (approval number: 331/23; date: November 2, 2023). The research complied with the tenets of the Declaration of Helsinki. All participants submitted written informed consent prior to enrollment. Participation was voluntary, and patients were informed that declining to participate would not impact their clinical care. Data collected were anonymized before analysis to ensure confidentiality. All data were discarded at the end of the study.
Results
Participant enrollment, non-response rate, and baseline characteristics
A total of 512 patients diagnosed with advanced glaucoma were recruited during the study period. Twenty-five patients opted out of participation or provided incomplete responses, resulting in a final analytic sample of 487 participants, which corresponds to a response rate of 95.1%. Participants ranged in age from 18 to 86 years, with a mean age of 52.87±14.94 years. Females comprised 239 (49.08%) of the study population. Two hundred and seventy-five (56.47%) participants resided in rural or semi-rural areas, and 338 out of 487 participants (69.40%) had enrolled in national health insurance schemes. In terms of educational attainment, merely eight of them (1.64%) lacked formal education, whereas 51 (10.47%) had not yet completed primary education (see Table 1).
Clinical characteristics and treatment
The average number of years of treatment is 2.18±1.90, while the median time after glaucoma diagnosis was 1.5 years. During the interview, 357 of the participants (73.31%) were using two or more topical antiglaucoma medications, while 129 (26.49%) had a history of unilateral glaucoma surgery or any glaucoma-related surgical interventions, including combined phacoemulsification, goniosynechialysis, etc. More details are outlined in Table 2.
Primary open-angle glaucoma constituted the predominant diagnosis among 185 patients (37.99%), with primary angle-closure glaucoma following at 153 (31.42%), while other types comprised 149 (21.39%). During the interview, 358 of the patients (73.51%) had not received any surgical treatment for their glaucoma; 91 patients (18.69%) had undergone trabeculectomy with mitomycin-C; 35 patients (7.19%) had other procedures, such as phaco-goniosynechialysis or phaco-trabeculectomy; and only three patients (0.62%) had a glaucoma tube implant.
The patients list hypertension (53.18%; n=259), cataract (31.62%; n=154), and diabetes (20.94%; n=102) as their top three comorbidities. They also list dyslipidemia (7.80%; n=38), ischemic heart disease (7.39%; n=36), obesity (6.37%; n=31), hypothyroidism (2.05%; n=10), asthma (0.62%; n=3), renal disease (0.41%; n=2), and other conditions (0.41%; n=2). The type of glaucoma significantly influenced patient preference. This relationship was statistically significant (χ2=17.088; p=0.009). A significant proportion of patients (79.3%) indicated consistent attendance at clinic follow-ups; however, 41.2% admitted to having missed at least one scheduled appointment in the past year.
Preference for glaucoma treatment modality
Overall, 350 individuals (71.87%) favored ongoing medicinal therapy, while 137 participants (28.13%; 95% CI: 24.1-32.2%) indicated a preference for surgical intervention if advised by their ophthalmologist (Figure 1). Preference for surgery was greater among patients with longer disease duration, increased medication burden, and previous glaucoma surgery exposure, although these associations did not maintain significance after multivariable adjustment.
Prevalence of adult patients preferring surgery over continued medical therapy Source: Authors' own data from the cross-sectional study
Glaucoma knowledge scores
The cohort as a whole had a mean glaucoma knowledge score of 55.2%±12.6%. Participants who favored surgical intervention exhibited notably higher knowledge scores than those who preferred medical therapy (58.03%±16.13% vs. 54.09%±17.17%; p=0.048); see Table 3. Knowledge gaps were particularly evident concerning the irreversibility of vision loss and the long-term objectives of surgical intervention.
HBM constructs
Participants who favored surgical treatment had significantly higher mean scores for perceived severity and susceptibility to glaucoma-related blindness. Additionally, they showed increased self-efficacy in handling postoperative care and higher perceived advantages of surgery. Conversely, perceived barriers, specifically fear of surgery, cost concerns, and fear of postoperative vision loss, were significantly greater among participants who preferred medical therapy (all p<0.01; Table 4). Participants who preferred surgical intervention more frequently reported cues to action, including recommendations from ophthalmologists and testimonials from other patients who had undergone surgery (Table 5).
Bivariate analysis and multivariable logistic regression analysis
In bivariate analysis, significant associations were found between preference for surgical intervention and higher glaucoma knowledge scores, greater perceived severity, greater perceived benefits, higher self-efficacy, and lower perceived barriers (p<0.05 for all). Sociodemographic variables, including age, sex, residence, education level, and insurance status, did not show a significant association with treatment preference (Table 6).
Variables that satisfied the inclusion criteria from the bivariate analysis were incorporated into a multivariable logistic regression model. Following adjustment, four constructs of the HBM were found to be independently associated with the preference for surgical intervention: perceived severity (aOR: 1.71; 95% CI: 1.17-2.51), perceived benefits of surgery (aOR: 1.51; 95% CI: 1.16-1.94), self-efficacy (aOR: 1.46; 95% CI: 1.11-1.93), and perceived barriers (aOR: 0.61; 95% CI: 0.49-0.77). Following adjustment for health belief constructs, the glaucoma knowledge score did not demonstrate an independent association with surgical preference (Table 7).
Discussion
Using the HBM as an explanatory framework, this study offers one of the earliest comprehensive and extensive analyses of glaucoma treatment preference among people with advanced disease, if not in Cambodia, in our resource-constrained clinical setting. The findings indicate that the preference for surgical intervention is low, with less than one-third of patients expressing a willingness to undergo surgery, even in the context of advanced disease severity. Treatment preference was primarily influenced by psychosocial factors rather than demographic or clinical variables, highlighting the significant impact of patient beliefs on glaucoma decision-making.
Interpretation of key findings through the HBM
The strong association between perceived severity and preference for surgical intervention supports the HBM hypothesis that individuals are more likely to adopt health-protective behaviors when they recognize the seriousness of their condition [11]. Patients who understood the irreversible nature of glaucomatous visual loss and the limitations of conventional therapy were more likely to accept surgery. This finding aligns with research from high-income and middle-income contexts, indicating that perceived disease severity significantly influences the acceptance of invasive interventions in chronic eye diseases [8,12].
The perceived benefits of surgery were identified as a significant predictor of surgical preference. Patients who believed that surgery could achieve sustained control of intraocular pressure and decrease long-term reliance on medication demonstrated a significantly higher preference for surgical management [8]. This is consistent with previous studies showing that patients frequently underestimate the long-term advantages of glaucoma surgery, especially when visual acuity is largely maintained [8,13,14]. Ignoring these advantages could delay the acceptance of final therapy in advanced glaucoma, where functional vision loss may occur before vision loss.
Conversely, perceived barriers, such as fear of surgical intervention, financial considerations, and anxiety about postoperative vision impairment, were strongly linked to a preference for ongoing medical treatment. Barriers have been consistently acknowledged in low- and middle-income countries, where restricted access to surgical services, indirect costs, and sociocultural beliefs regarding eye surgery affect how patients choose [15,16]. In Cambodia, significant out-of-pocket health expenditures persist despite the existence of national insurance schemes, suggesting that financial barriers significantly influence treatment preferences.
Additionally, self-efficacy also independently predicted preference for surgical intervention. Patients who felt confident in their ability to undergo surgery, adhere to postoperative care, and attend follow-up visits were more willing to consider surgical treatment. This finding underscores the significance of patient empowerment and education in managing chronic diseases, aligning with evidence from studies on glaucoma and cataract care that indicate a correlation between higher self-efficacy and enhanced treatment uptake and adherence [8,17].
Glaucoma knowledge and its indirect role
Higher glaucoma knowledge scores were initially linked to a preference for surgery; however, this association did not remain significant after adjusting for HBM constructs. This shows that knowledge alone is insufficient to influence treatment decisions in our populations unless it results in significant changes in perceived severity, benefits, and barriers. Information provided without addressing emotional and contextual aspects has been found to have little effect on behavior in other chronic eye disorders [8,17-19]. The findings underscore the necessity for counseling strategies that extend beyond factual education and involve beliefs, fears, and expectations.
Comparison with previous literature
The low surgical preference documented in this study contrasts with findings from high-income countries, where earlier diagnosis, greater confidence in healthcare systems, and more comprehensive insurance coverage led to increased acceptability of glaucoma surgery [19]. The results, however, are in line with research from sub-Saharan Africa and Southeast Asia, where even in cases of severe disease, late presentation and reliance on medical care are typical [15,20]. The HBM's cross-cultural applicability in glaucoma care was further supported by a study conducted among glaucoma patients in Egypt, which found that perceived advantages and barriers were the best indicators of surgical acceptability [8]. This study contributes to the existing literature by offering context-specific evidence from Cambodia, a region where empirical data on glaucoma decision-making is limited.
Clinical and public health implications
These findings are pertinent to the management of glaucoma within our routine care practices and may also be applicable in Cambodia by highlighting the significance of integrating structured, patient-centered counseling into standard glaucoma treatment protocols. Counseling should explicitly address misconceptions related to surgery, emphasize the irreversible nature of glaucomatous damage, and set realistic expectations regarding surgical results. Interventions designed to address perceived barriers, such as financial counseling, peer-support initiatives, and testimonials from patients who have successfully undergone treatment, may improve acceptance of surgical procedures. Third, bolstering self-efficacy through optimized postoperative care pathways and enhanced follow-up support may facilitate prompt surgical intervention. These results endorse the incorporation of behavioral health frameworks into national eye care policies at the policy level. Addressing the psychosocial determinants influencing care-seeking behavior is essential for attaining universal eye health and reducing preventable blindness caused by glaucoma [21].
Limitations
This investigation is characterized by several limitations. The cross-sectional design restricts the ability to establish causality, and expressed treatment preferences may not necessarily reflect actual behavior. Data were collected at a single tertiary center, potentially limiting the generalizability to primary or secondary care settings, as well as during ongoing community-based care. Health belief constructs were evaluated using self-administered questionnaires, which may be subject to social desirability bias. Despite these limitations, the large sample size and the theory-based analytical approach strengthen the validity and relevance of the findings.
Conclusions
Within our clinical practice, the inclination toward surgical treatment among Cambodian patients with advanced glaucoma remains markedly minimal and is predominantly influenced by health-related beliefs rather than exclusively by demographic or clinical considerations. Enhancing glaucoma management outcomes necessitates the implementation of strategies that encompass psychosocial support, patient education, and the mitigation of barriers within the healthcare system.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global estimates of visual impairment: 2010 Br J Ophthalmol Pascolini D Mariotti SP 6146189620122213398810.1136/bjophthalmol-2011-300539 · doi ↗ · pubmed ↗
- 2Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study Lancet Glob Health 0609202110.1016/S 2214-109X(20)30489-7PMC 782039133275949 · doi ↗ · pubmed ↗
- 3Rapid assessment of avoidable blindness report: Cambodia (2019)London School of Hygiene & Tropical Medicine RAAB Repository [Internet 6 2024 2024 https://datacompass.lshtm.ac.uk/id/eprint/4203/
- 4The hub-and-spoke management of glaucoma Front Neurosci Nuzzi R Marolo P Nuzzi A 1801420203225630610.3389/fnins.2020.00180 PMC 7090234 · doi ↗ · pubmed ↗
- 5Patient and provider perspectives on glaucoma treatment adherence: a Delphi study in urban Alabama Optom Vis Sci Poleon S Racette L Fifolt M Schoenberger-Godwin YM Abu SL Twa MD 108510939820213452421310.1097/OPX.0000000000001776 PMC 8505131 · doi ↗ · pubmed ↗
- 6Global eye health and the sustainable development goals: protocol for a scoping review BMJ Open Zhang JH Ramke J Mwangi N 010202010.1136/bmjopen-2019-035789 PMC 720270132193274 · doi ↗ · pubmed ↗
- 7Universal health coverage - there is more to it than meets the eye J Family Med Prim Care Faizi N Kazmi S 169170620172902677710.4103/jfmpc.jfmpc_13_17PMC 5629889 · doi ↗ · pubmed ↗
- 8Applying the Health Belief Model to predict preference for surgical intervention versus medical therapy among patients with open-angle glaucoma BMJ Open Ophthalmol Awad K Awad R Elkazaz H Saleh M Mehanna A 072022