Seminal Interleukin-6 as a Biomarker of Inflammation, Oxidative Stress, and Sperm Dysfunction in Infertile Men
Loïc Koumba, Mariame Kabbour, Salma Ed-doumy, Mariem Norredine, Ahlam Zarhouti, Modou Mamoune Mbaye, Bouchra Ghazi, Noureddine Louanjli, Moncef Benkhalifa, Rajaa Ait Mhand, Ouafaa Aniq Filali

TL;DR
This study shows that high levels of IL-6 in semen are linked to poor sperm quality and inflammation in infertile men, suggesting it could be a useful biomarker.
Contribution
The study identifies seminal IL-6 as a novel biomarker for inflammation, oxidative stress, and sperm dysfunction in male infertility.
Findings
Higher seminal IL-6 levels correlate with reduced sperm motility, vitality, and increased DNA fragmentation.
IL-6 independently predicts elevated leukocyte counts and bacteriospermia in infertile men.
Seminal IL-6 is detectable in all samples and shows strong associations with oxidative stress markers.
Abstract
Background/Objectives: Interleukin-6 (IL-6), a pleiotropic cytokine involved in immune regulation, is consistently detected in human semen, even in the absence of overt infection. Its contribution to sperm dysfunction, oxidative stress, and inflammation remains incompletely understood. This study evaluated the associations between seminal IL-6 concentrations and markers of semen quality, oxidative stress, nuclear integrity, and genital tract inflammation in infertile men. Methods: A cohort of 204 infertile men was assessed. Seminal IL-6 was quantified by electrochemiluminescence immunoassay. Semen parameters, malondialdehyde (MDA), catalase (CAT) activity, sperm DNA fragmentation index (DFI), sperm chromatin decondensation index (SDI), leukocytospermia, and bacteriospermia were measured. Analyses included correlation testing, IL-6 threshold stratification (<30, 30–60, 60–100, ≥100…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
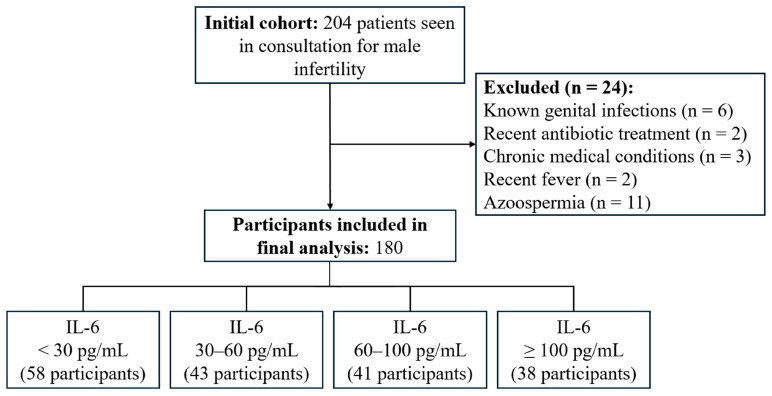 Figure 1
Figure 1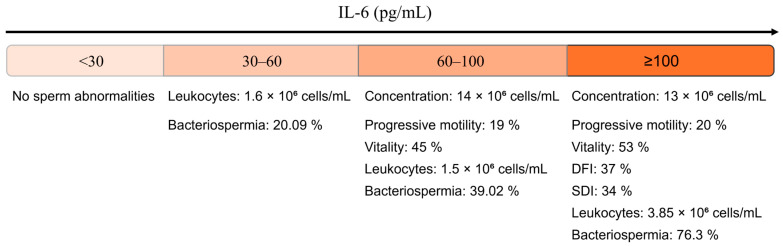 Figure 2
Figure 2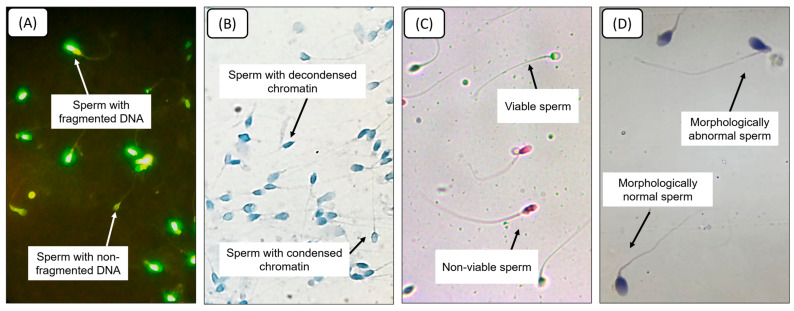 Figure 3
Figure 3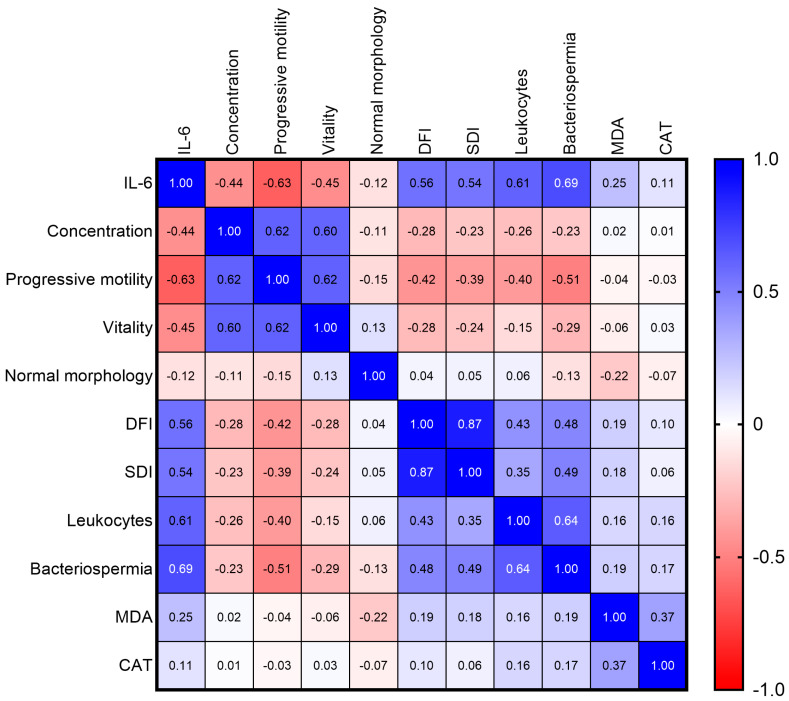 Figure 4
Figure 4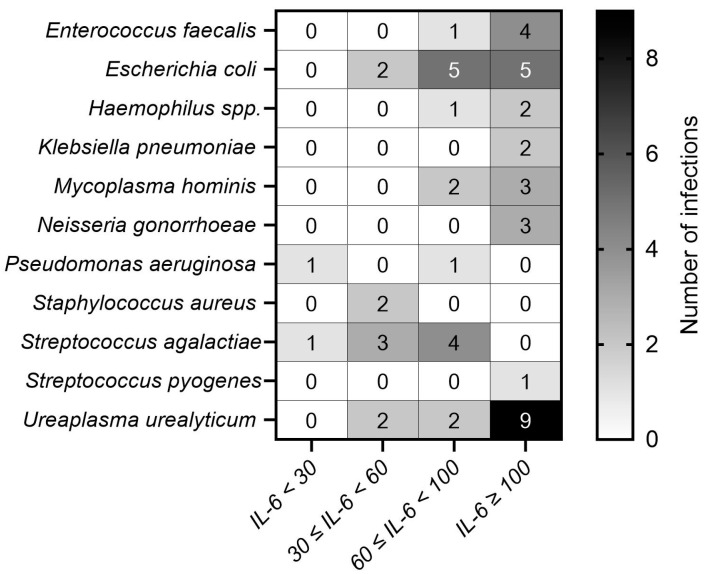 Figure 5
Figure 5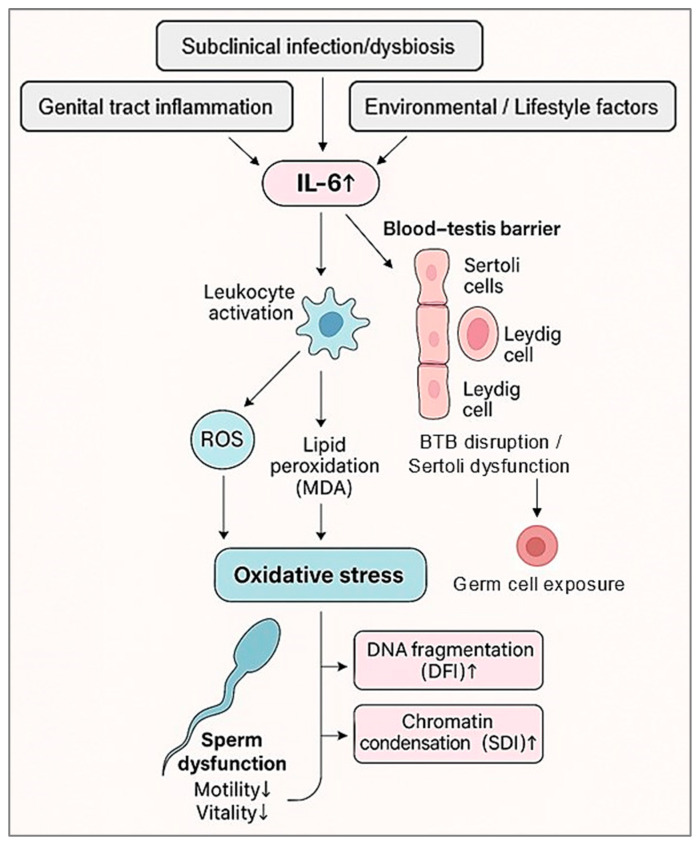 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSperm and Testicular Function · Reproductive System and Pregnancy · Preterm Birth and Chorioamnionitis
1. Introduction
Infertility is defined as the inability of a couple to conceive after 12 months of regular, unprotected intercourse and affects approximately 15% of reproductive-age couples worldwide [1,2]. A purely male factor is identified in 20–30% of cases, and male involvement is present in nearly half, either as an isolated or combined contributor [3,4,5]. Among male etiologies, inflammation of the genital tract is recognized as a major determinant.
This inflammatory process involves a complex network of cytokines and immunomodulatory mediators capable of disrupting spermatogenesis, altering the testicular microenvironment, and impairing sperm function, including motility, acrosome reaction, and DNA integrity [5,6,7,8,9]. Among these mediators, interleukin-6 (IL-6) plays a central regulatory role in inflammatory and immune responses. Unlike TNF-α or IL-1β, which are primarily implicated in acute-phase reactions, or IL-8, which governs neutrophil recruitment, IL-6 contributes to both the initiation and the chronic maintenance of inflammation, thereby bridging acute and sustained immune activation [6,10,11,12,13].
Multiple studies have reported the frequent detection of IL-6 in human semen, even in the absence of clinical signs of infection [12,14,15]. However, the evidence remains highly variable due to differences in study populations, methodological approaches, and diagnostic thresholds, which range widely from about 15 pg/mL [16] to more than 200 pg/mL [17]. Although several case–control studies comparing fertile and infertile men have reported higher seminal IL-6 levels in infertile individuals [18,19,20,21], these findings remain heterogeneous and rarely explore the internal biological gradients that may exist within infertile populations. Such gradients could provide important insight into disease severity, prognostic stratification, and potential therapeutic monitoring.
To address these gaps, the present study adopts an intra-cohort analytical design in a homogeneous population of infertile men to characterize dose–response relationships between seminal IL-6 concentrations and key markers of sperm dysfunction. Specifically, this approach aims to: (i) identify clinically meaningful IL-6 thresholds associated with progressive impairment of standard semen parameters (concentration, progressive motility, vitality), inflammatory markers (leukocytospermia, bacteriospermia), and oxidative/nuclear damage indicators (MDA, catalase, DFI, SDI); and (ii) compare the predictive performance of IL-6 with that of conventional biomarkers within the inflammatory–oxidative spectrum observed in infertile men.
2. Materials and Methods
2.1. Study Population
A total of 204 infertile men aged 24–56 years who consulted the LABOMAC laboratory (Casablanca, Morocco) for semen analysis were enrolled in this study.
2.2. Inclusion and Exclusion Criteria
Inclusion criteria were the absence of antibiotic treatment within the previous three months, provision of a complete ejaculate, and signed informed consent. Exclusion criteria included azoospermia, cryptozoospermia, documented genital tract infection, chronic illness, or a recent febrile episode.
2.3. Semen Collection
Participants observed 3–5 days of sexual abstinence prior to sample collection. To minimize contamination, they were instructed to void urine, wash their hands and genital area with antimicrobial soap, and rinse with sterile saline solution. Semen samples were obtained by masturbation in a dedicated laboratory room and collected in sterile, non-cytotoxic containers.
2.4. Semen Analysis
Semen analyses were performed according to World Health Organization guidelines [2]. After liquefaction at 37 °C for 30 min, sperm concentration and motility were assessed using computer-assisted semen analysis (CASA; Spermolyzer^TM^, Mira Lab, Cairo, Egypt).
Sperm morphology was evaluated on Schorr’s hematoxylin-stained smears according to the modified David classification. Vitality was assessed using 2% eosin staining, with a minimum of 200 cells manually counted.
Leukocyte concentration was determined using either peroxidase staining or CD45 immunolabeling, depending on reagent availability at the time of analysis. Systematic bacteriological cultures were performed on selective media to identify urogenital pathogens.
2.5. Definition of Leukocytospermia
Leukocytospermia was defined as ≥1 × 10^6^ leukocytes/mL [2] and assessed using the LeucoScreen^®^ test (Fertipro, Beernem, Belgium). Briefly, 10 µL of semen was mixed with 10 µL of a working solution prepared by diluting 30 µL of 3% hydrogen peroxide in LeucoScreen reagent to a final volume of 1 mL. After 2 min of incubation, preparations were examined under light microscopy (×40 objective). Leukocytes, identified by their brown coloration, were manually counted and expressed as cells per milliliter.
2.6. Bacteriological Analysis
Semen aliquots were diluted 1:10 (v/v) in sterile isotonic saline (0.15 M NaCl) and plated on enriched chocolate agar (Polyvitex^®^, bioMérieux, Marcy-l’Étoile, France). Cultures were incubated at 37 °C under 5% CO_2_ for 24–72 h.
Bacteria were identified using biochemical methods and automated systems (Vitek 2 Compact^®^ and API 10S^®^, bioMérieux, France). Pathogenicity thresholds were interpreted in accordance with the French Référentiel en Microbiologie Médicale [22], and only bacterial species exceeding their species-specific pathogenicity thresholds were included in the analysis. Commensal flora and non-pathogenic isolates were excluded.
2.7. Sperm DNA Fragmentation and Chromatin Decondensation
2.7.1. Sample Preparation
All semen samples were processed within one hour after collection. After centrifugation (1000× g, 15 min), seminal plasma was stored at −20 °C for biochemical analyses. The sperm pellet was washed in phosphate-buffered saline (PBS, pH 7.4), centrifuged (400× g, 10 min), and smeared onto two separate slides: one for the TUNEL assay (DNA fragmentation) and another for aniline blue staining (chromatin condensation).
Slides were air-dried, fixed in PBS–formaldehyde (90/10, v/v) at 37 °C for 30 min, rinsed, and permeabilized for 1 min in a solution containing distilled water (98%), sodium citrate (1%), and Triton X-100 (1%).
2.7.2. DNA Fragmentation Index (DFI)
DNA fragmentation was quantified using the TUNEL assay (In Situ Cell Death Detection Fluorescein Kit, Roche Diagnostics GmbH, Mannheim, Germany), strictly following the manufacturer’s instructions. Slides were analyzed under a fluorescence microscope (Nikon Eclipse 80i, Nikon Corporation, Tokyo, Japan) using a ×100 oil-immersion objective. For each sample, a minimum of 200 spermatozoa were evaluated. Fluorescent nuclei were classified as fragmented, and the DFI was calculated as the percentage of TUNEL-positive spermatozoa.
Consistent with established thresholds, a DFI ≥ 30% was considered abnormal and indicative of impaired sperm nuclear integrity [23].
2.7.3. Sperm Chromatin Decondensation Index (SDI)
Chromatin condensation was assessed using aniline blue staining, according to the protocol described by Belloc et al. [24]. Slides were stained for 15 min, rinsed, air-dried, and examined by bright-field microscopy (×100 objective). For each sample, 200 spermatozoa were counted.
Spermatozoa exhibiting dark-blue staining, reflecting excessive histone retention, were classified as abnormal. An SDI ≥ 30% was considered pathological.
2.8. Seminal IL-6 Measurement
Interleukin-6 concentrations were quantified in seminal plasma using a sandwich electrochemiluminescence immunoassay (ECLIA; Elecsys^®^ IL-6 kit, Roche Diagnostics GmbH, Mannheim, Germany) following the manufacturer’s recommendations.
The analytical range was 1.5–5000 pg/mL, enabling sensitive detection of subclinical inflammation and accurate measurement under moderate to severe inflammatory conditions. To account for the heterogeneity of thresholds reported in the literature (≈15–200 pg/mL), seminal IL-6 concentrations were further categorized into four groups: <30, 30–60, 60–100, and ≥100 pg/mL. These cut-off values were derived from the empirical distribution of IL-6 in our cohort, approximately corresponding to the 25th, 50th, and 75th percentiles and rounded to the nearest integer to facilitate clinical interpretation. Because of the right-skewed distribution of IL-6, the resulting groups are not numerically equivalent in size but reflect the underlying biological heterogeneity of the population.
2.9. Catalase Activity
Catalase activity was measured spectrophotometrically according to the method of Aebi [25], by monitoring hydrogen peroxide (H_2_O_2_) degradation at 240 nm. The reaction mixture (1 mL) contained 7.5 mM H_2_O_2_ in 50 mM potassium phosphate buffer (pH 7.4), with 10 µL of seminal plasma added. Catalase activity was calculated using the molar extinction coefficient of H_2_O_2_ (ε = 0.0394 mM^−1^·cm^−1^) and expressed as µmol of H_2_O_2_ degraded per minute per milligram of protein.
2.10. Malondialdehyde (MDA) Measurement
Lipid peroxidation was assessed using the thiobarbituric acid reactive substances (TBARS) assay [26]. Briefly, 100 µL of seminal plasma was mixed with 900 µL of a solution containing 0.375% thiobarbiturbituric acid (TBA), 15% trichloroacetic acid (TCA), and 0.25 M hydrochloric acid (HCl). Samples were incubated at 100 °C for 20 min, cooled on ice, and centrifuged at 1000× g for 10 min at 4 °C. Absorbance of the supernatant was measured at 535 nm. MDA concentration was calculated using an extinction coefficient of 1.56 × 10^5^ M^−1^·cm^−1^ and expressed as nmol per mg of protein.
2.11. Statistical Analysis
Statistical analyses were performed using GraphPad Prism (version 10.4.1, GraphPad Software, Boston, MA, USA). As the data did not follow a normal distribution (Kolmogorov–Smirnov test), results are presented as medians with interquartile ranges (IQR).
Comparisons of semen quality, inflammatory markers, and oxidative stress parameters across IL-6 groups were performed using the Kruskal–Wallis test, followed by Dunn’s post hoc test with Bonferroni correction when appropriate. Spearman’s rank coefficient (ρ) was used to assess correlations.
Multivariate regression models (linear or logistic, depending on the outcome variable) were applied to identify independent associations between IL-6 levels and biological parameters. Age, smoking status, and alcohol consumption were systematically included as covariates in all regression models to account for their potential confounding effects. Results are expressed as β coefficients (linear regression) or odds ratios (OR, logistic regression), with 95% confidence intervals (CI).
To evaluate the diagnostic performance of seminal IL-6, receiver operating characteristic (ROC) analyses were conducted for the prediction of (i) DFI ≥ 30%, (ii) SDI ≥ 30%, and (iii) bacteriospermia. For comparison, ROC analyses were also performed for leukocyte concentration, malondialdehyde (MDA), and catalase (CAT). For each marker and outcome, the area under the curve (AUC), optimal cut-off value (Youden index), sensitivity, and specificity were calculated. Only the numerical results of these ROC analyses are reported in the manuscript; ROC curve plots were not included.
A p-value < 0.05 was considered statistically significant.
2.12. Quality Control
All semen analyses and biochemical assays were performed in duplicate, and results were independently validated by two blinded analysts. In case of discrepancy, a senior biologist reviewed the data or repeated the assay to ensure reliability.
2.13. Ethical Considerations
The study protocol was approved by the Biomedical Research Ethics Committee of UM6SS (reference: CE/UM6SS/09/23; 25 July 2023). Written informed consent was obtained from all participants prior to inclusion. All data were anonymized and analyzed in accordance with the principles of the Declaration of Helsinki (2013 revision).
3. Results
3.1. Description of the Study Population
Of the 204 patients initially recruited, 24 were excluded due to non-eligibility (Figure 1). The final analysis included 180 participants. IL-6 was detectable in all seminal plasma samples, with a median concentration of 31.52 pg/mL (Q1 = 12.39 pg/mL; Q3 = 70.11 pg/mL; IQR = 57.72 pg/mL; range: 1.5–5000 pg/mL).
To investigate potential dose–response relationships, participants were stratified into four IL-6 concentration groups (<30, 30–60, 60–100, and ≥100 pg/mL). These categories reflect the empirical distribution of IL-6 in the cohort and correspond approximately to the 25th, 50th, and 75th percentiles, rounded to the nearest integer to facilitate clinical interpretation.
3.2. Sociodemographic Characteristics
Table 1 summarizes the distribution of age, smoking status, and alcohol consumption across IL-6 groups. The mean age of participants was 36.06 ± 8.01 years. Among them, 37 (20.6%) reported smoking and 25 (13.9%) reported regular alcohol consumption. No statistically significant differences were observed between IL-6 groups for any sociodemographic or behavioral variable.
3.3. Semen Parameters, Inflammatory and Oxidative Markers
Figure 2 provides a descriptive overview of seminal characteristics across the four IL-6 concentration groups, using WHO reference thresholds for classifying semen parameters [2]. In the <30 pg/mL group, no semen abnormalities were detected according to WHO criteria. In the 30–60 pg/mL group, leukocytospermia (1.6 × 10^6^ cells/mL) and bacteriospermia (20.09%) were observed.
From 60 to 100 pg/mL, alterations included reduced sperm concentration, progressive motility, and vitality, together with increased leukocyte counts and a higher proportion of bacteriospermia (39.02%). The ≥100 pg/mL group exhibited the most marked abnormalities, including low semen parameters, elevated DFI (37%) and SDI (34%), leukocytospermia (3.85 × 10^6^ cells/mL), and the highest rate of bacteriospermia (76.3%).
This figure provides a descriptive summary without statistical inference and visually complements the analytical findings reported later in Section 3.
Semen quality varied significantly across IL-6 groups (Table 2). Participants with IL-6 concentrations < 30 pg/mL exhibited the most favorable seminal profile, with a median sperm concentration of 35 × 10^6^/mL, progressive motility of 45.4%, and vitality of 70%. These parameters declined progressively with increasing IL-6 levels, reaching their lowest values in the ≥100 pg/mL group (p < 0.001). No significant differences were observed for normal sperm morphology (p = 0.378).
Conversely, DFI, SDI, leukocyte counts, bacteriospermia, and MDA concentrations increased with rising IL-6 levels, with significant differences emerging from the 60–100 pg/mL group. Catalase activity did not differ significantly between groups (p = 0.326).
Post hoc analyses (Dunn’s test with Bonferroni correction) confirmed that IL-6 ≥ 60 pg/mL was significantly associated with reduced sperm concentration, progressive motility, and vitality, as well as increased DFI, SDI, leukocytospermia, and bacteriospermia compared with the <30 pg/mL group (p < 0.05). These differences were most pronounced in the ≥100 pg/mL group (p ≤ 0.0086). MDA levels were significantly elevated only in the ≥100 pg/mL group (p = 0.0325).
To illustrate the microscopic alterations underlying the quantitative measurements, Figure 3 presents representative images of spermatozoa with fragmented versus non-fragmented DNA (TUNEL assay), condensed versus decondensed chromatin (aniline blue staining), live versus dead cells (eosin vitality test), and morphologically normal versus abnormal forms (H&E staining). These examples visually complement the quantitative data by showing the corresponding structural and functional changes.
3.4. Correlation Analyses
To provide an integrated overview of the interrelationships among the seminal parameters investigated, a Spearman correlation matrix was generated (Figure 4). This visualization highlights several strong associations within the cohort.
IL-6 exhibited the most pronounced correlations, showing strong positive associations with bacteriospermia (ρ = 0.694), leukocyte concentration (ρ = 0.614), DFI (ρ = 0.560), and SDI (ρ = 0.543). In contrast, the strongest negative correlations were observed with progressive motility (ρ = −0.628), vitality (ρ = −0.452), and sperm concentration (ρ = −0.443).
Beyond the central role of IL-6, the matrix revealed additional biologically relevant relationships, including a very strong correlation between DFI and SDI (ρ = 0.867), as well as inverse associations between classical semen parameters (concentration, motility, vitality) and markers of inflammation or nuclear integrity.
3.5. Bacterial Profile
Bacterial infection was identified in 56 cases (31.1%), with 11 distinct species isolated (Figure 5). Each infected sample harbored only one bacterial species. In accordance with the microbiological criteria used in the study, only organisms exceeding their species-specific pathogenicity thresholds were considered; commensal flora and non-pathogenic isolates were systematically excluded from the analysis.
Bacterial diversity increased progressively with IL-6 concentration. In the <30 pg/mL group, only Pseudomonas aeruginosa and Streptococcus agalactiae were detected. In the 30–60 pg/mL group, isolates included Escherichia coli (n = 2), Staphylococcus aureus (n = 2), Ureaplasma urealyticum (n = 2), and S. agalactiae (n = 3). The 60–100 pg/mL group showed 16 infections, predominantly E. coli (n = 5) and S. agalactiae (n = 4). In the ≥100 pg/mL group, 29 infections were recorded, with U. urealyticum (n = 9) and E. coli (n = 5) being most frequent, followed by Enterococcus faecalis (n = 4), Mycoplasma hominis (n = 3), and Neisseria gonorrhoeae (n = 3).
3.6. Diagnostic Performance of IL-6 and Related Biomarkers
To assess the potential value of seminal IL-6 as a biomarker of sperm impairment, ROC analyses were performed for the prediction of DFI ≥ 30%, SDI ≥ 30%, and bacteriospermia. For comparison, ROC analyses were also conducted for leukocyte concentration, MDA, and catalase (CAT).
As summarized in Table 3, IL-6 exhibited good to excellent diagnostic performance for all three outcomes, with AUC values of 0.859 and 0.855 for DFI ≥ 30% and SDI ≥ 30%, respectively, and 0.927 for bacteriospermia. Leukocyte concentration also showed high performance, particularly for bacteriospermia (AUC = 0.904), whereas MDA and CAT displayed more modest diagnostic accuracies.
3.7. Multivariate Analyses
Multivariate linear regression, adjusted for age, smoking status, and alcohol consumption, identified IL-6 as an independent predictor of reduced progressive motility (β = −0.005; p = 0.032) and elevated leukocyte count (β = 0.0018; p < 0.0001). After adjustment for these covariates, no independently significant associations were found between IL-6 and sperm concentration, vitality, morphology, MDA, or catalase activity (Table 4).
Logistic regression analysis, likewise adjusted for age, smoking status, and alcohol consumption, showed that IL-6 significantly increased the odds of DFI ≥ 30% (OR = 1.0007; p = 0.032), SDI ≥ 30% (OR = 1.0006; p = 0.027), and bacteriospermia (OR = 1.0325; p < 0.001).
4. Discussion
This study examined the relationship between seminal IL-6 concentrations and key indicators of sperm dysfunction, oxidative stress, and inflammation in infertile men. IL-6 was detected in all samples, confirming its near-ubiquitous presence in the male reproductive tract [27,28]. Concentrations varied markedly (median: 31.52 pg/mL; IQR: 57.72 pg/mL), reflecting substantial interindividual variability in inflammatory activation, a finding consistent with evidence that IL-6 participates in the immunoregulatory milieu of the male genital tract and may reflect subclinical inflammation, asymptomatic infection, or environmental exposures [13,29].
This work provides three novel and complementary contributions to the understanding of seminal inflammation in male infertility. First, we established four clinically interpretable IL-6 thresholds (<30, 30–60, 60–100, and ≥100 pg/mL), revealing a coherent dose–response gradient across functional, inflammatory, and oxidative parameters. Second, IL-6 emerged as an independent predictor of nuclear instability (DFI, SDI ≥ 30%) and bacteriospermia, even after adjustment for age, smoking, and alcohol consumption. Third, IL-6 demonstrated superior diagnostic performance compared with leukocyte count, MDA, and catalase for predicting bacteriospermia, DFI ≥ 30%, and SDI ≥ 30%, reinforcing its relevance as a quantitative biomarker of seminal immuno-oxidative stress.
Unlike case–control studies that rely on a binary “normal vs. elevated” interpretation, an intra-cohort analytical design enables the characterization of continuous biological associations within infertile men. While this approach does not replace fertile–infertile comparisons nor establish physiological reference values, it provides complementary insights into internal dose–response patterns and potential risk stratification. This design rationale is essential to understand the added value of identifying IL-6 gradients within a clinically homogeneous infertile population.
A key methodological strength is the intra-cohort analytical design. Unlike case–control studies contrasting fertile and infertile populations, this approach characterizes continuous biological associations within infertile men and identifies clinically meaningful internal gradients. Although this design does not establish physiological reference values, it provides complementary insight into dose-dependent inflammatory and oxidative alterations. The IL-6 stratification approach revealed consistent patterns across semen quality, inflammation, and oxidative stress. Alterations appeared above 30 pg/mL, including reduced progressive motility, leukocytospermia (1.60 × 10^6^ cells/mL), and bacteriospermia in approximately 20% of participants. Above 60 pg/mL, abnormalities intensified, with reduced vitality and higher DFI/SDI, while concentrations ≥ 100 pg/mL were associated with the most severe impairments and significantly elevated MDA, indicating established oxidative injury. However, although IL-6 levels were significantly associated with nuclear damage markers (DFI, SDI), the present study does not provide direct experimental evidence demonstrating that IL-6–induced oxidative stress is causally responsible for these alterations. These associations should therefore be interpreted as reflective of a broader inflammatory–oxidative environment rather than proof of mechanistic causation.
Several biological mechanisms described in previous studies may contextualize these findings. IL-6 can compromise Sertoli cell function by disrupting the blood–testis barrier (BTB) via MAPK/ERK signaling, altering tight-junction proteins such as occludin and claudins, and impairing junctional turnover [30]. These changes may expose developing germ cells to inflammatory and oxidative mediators. IL-6 may also impair Leydig cell steroidogenesis by downregulating key enzymes (CYP11A1, 3β-HSD, StAR), reducing intratesticular testosterone and weakening endocrine support for spermatogenesis [31]. Furthermore, IL-6–driven inflammation promotes excess ROS production through leukocyte activation and mitochondrial dysregulation, contributing to lipid peroxidation (MDA) and nuclear instability (DFI, SDI). Taken together, these mechanistic insights provide a coherent interpretative framework for understanding how IL-6–driven inflammatory and oxidative processes may converge to affect sperm function and nuclear integrity. To synthesize these interactions, Figure 6 presents a conceptual model integrating our observed associations with established biological pathways.
Oxidative imbalance emerged as a central feature of this IL-6 gradient. IL-6 was positively correlated with MDA but showed no significant association with catalase activity, suggesting disproportionate ROS generation relative to antioxidant capacity. This profile is consistent with prior studies linking IL-6 to oxidative stress and impaired sperm function [29]. In the <30 pg/mL group, both MDA (423.3 nmol/mg) and catalase (467.8 µmol/min/mg) remained relatively elevated, an arrangement compatible with an early compensated redox state. As IL-6 concentrations increased, MDA rose markedly while catalase did not increase proportionally, indicating a shift toward net oxidative imbalance accompanied by declining motility and vitality and increasing DFI and SDI, in accordance with evidence on ROS-mediated sperm damage [32,33,34,35].
The inflammatory component was reinforced by the strong association between IL-6 and leukocytospermia (ρ = 0.64). Leukocyte concentration was directly quantified in all samples using the WHO-recommended peroxidase test, confirming the presence and/or magnitude of inflammatory cell recruitment within the seminal milieu. Leukocytes are major sources of cytokines and ROS and may sustain an IL-6–dependent inflammatory loop [3,36]. Building on this inflammatory profile, the concomitant increase in bacteriospermia and leukocytospermia suggests a potential interaction between microbial colonization/infection and inflammatory activation within the male genital tract. While bacterial presence can initiate leukocyte recruitment, inflammation-induced alterations of the seminal microenvironment may, in turn, promote dysbiosis and facilitate microbial persistence. However, the causal direction cannot be established in a cross-sectional observational design [5,37]. In continuity with this pattern, although no specific microorganism corresponded to any particular IL-6 category, higher IL-6 levels coincided with greater microbial diversity, consistent with broad immune activation through PRR–NF-κB or MAPK pathways [38,39]. The <30 pg/mL group represents the lowest inflammatory burden with-in infertile men and should not be considered a physiological control.
Multivariate analyses further strengthened the independent role of IL-6 in seminal dysfunction. After adjustment for age, smoking, and alcohol consumption, IL-6 remained significantly associated with reduced progressive motility (β = −0.005) and increased leukocyte concentration (β = 0.0018), and independently predicted bacteriospermia (OR = 1.0325), DFI ≥ 30%, and SDI ≥ 30% (OR = 1.0007 and OR = 1.0006). Although per-unit effect sizes appear modest, the cumulative impact across the IL-6 distribution is clinically relevant and reinforces IL-6 as a dose-dependent indicator of immuno-oxidative stress.
ROC analyses further demonstrated that IL-6 outperformed leukocytes, MDA, and catalase in predicting bacteriospermia and nuclear instability. IL-6 exhibited excellent discriminatory ability for bacteriospermia (AUC = 0.927) and strong predictive performance for DFI (AUC = 0.859) and SDI (AUC = 0.855). These results suggest that a single IL-6 measurement may enhance diagnostic workflows and risk stratification in infertile men.
This study has several limitations. Its cross-sectional design precludes causal inference, and its single-center setting may restrict external validity. Importantly, the study was conceived as an intra-cohort investigation aimed at characterizing internal biological relationships rather than establishing physiological reference values. Determining normative thresholds for IL-6, MDA, catalase, or microbiological parameters will require studies including fertile control groups. Future multicenter investigations involving more diverse populations and integrating additional oxidative markers will be needed to validate and extend these findings. Beyond these aspects, our dataset highlights the promising perspective of developing composite indices integrating IL-6, oxidative markers, and microbial profiles for refined assessment of seminal health.
5. Conclusions
This study identifies several novel and clinically relevant insights into seminal inflammation in male infertility. By stratifying IL-6 into threshold-based groups (<30, 30–60, 60–100, and ≥100 pg/mL), we identified distinct and coherent profiles of sperm dysfunction, inflammatory activation, and oxidative imbalance. IL-6 also emerged as an independent predictor of nuclear instability (DFI and SDI ≥ 30%) and bacteriospermia, even after adjustment for age, smoking, and alcohol consumption. Moreover, IL-6 demonstrated superior diagnostic performance compared with leukocyte count, MDA, and catalase for predicting bacteriospermia and nuclear damage.
Taken together, these findings support the potential value of IL-6 as a quantitative biomarker of seminal immuno-oxidative stress and as a candidate tool for refining diagnostic assessment and risk stratification in infertile men. However, these associations remain correlative, and the mechanistic pathways discussed are conceptual rather than experimentally demonstrated within this study.
Future research should include longitudinal and interventional studies, as well as the incorporation of fertile control groups, to establish normative reference values, validate the proposed thresholds, and determine the clinical utility of IL-6 for diagnosis, prognosis, and therapeutic monitoring in male infertility.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Choy J.T. Eisenberg M.L. Male Infertility as a Window to Health Fertil. Steril.201811081081410.1016/j.fertnstert.2018.08.01530316415 · doi ↗ · pubmed ↗
- 2World Health Organization WHO Laboratory Manual for the Examination and Processing of Human Semen 6th ed. World Health Organization Human Reproduction Programme WHO Press Geneva, Switzerland 2021978-92-4-003078-7
- 3Hussain U. Venishetty N. Alkassis M. Raheem O. The Clinical Management of Leukocytospermia in Male Infertility: A Narrative Review Uro 20244364910.3390/uro 4020004 · doi ↗
- 4Agarwal A. Baskaran S. Parekh N. Cho C.L. Henkel R. Vij S. Arafa M. Panner Selvam M.K. Shah R. Male Infertility Lancet 202139731933310.1016/S 0140-6736(20)32667-233308486 · doi ↗ · pubmed ↗
- 5Henkel R. Leukocytospermia and/or Bacteriospermia: Impact on Male Infertility J. Clin. Med.202413284110.3390/jcm 1310284138792382 PMC 11122306 · doi ↗ · pubmed ↗
- 6Leisegang K. Bouic P.J.D. Henkel R.R. Metabolic Syndrome Is Associated with Increased Seminal Inflammatory Cytokines and Reproductive Dysfunction in a Case-Controlled Male Cohort Am. J. Reprod. Immunol.20167615516310.1111/aji.1252927334450 · doi ↗ · pubmed ↗
- 7Azenabor A. Oloruntoba Ekun A. Akinloye O. Impact of Inflammation on Male Reproductive Tract J. Reprod. Infertil.20151612312926913230 PMC 4508350 · pubmed ↗
- 8Hasan H. Bhushan S. Fijak M. Meinhardt A. Mechanism of Inflammatory Associated Impairment of Sperm Function, Spermatogenesis and Steroidogenesis Front. Endocrinol.20221389702910.3389/fendo.2022.897029 PMC 909621435574022 · doi ↗ · pubmed ↗