ADHD and Moral Development in Childhood and Adolescence: A Systematic Review of Attachment, Temperament, and Socio-Emotional Mechanisms
Ilaria Notaristefano, Federica Gigliotti, Benedetta Altomonte, Ilaria Graziani, Beatrice Piunti, Maria Romani

TL;DR
Children and adolescents with ADHD often struggle with moral development due to issues like emotional dysregulation and poor social skills, not just ADHD symptoms alone.
Contribution
This systematic review identifies how attachment, temperament, and socio-emotional factors interact to affect moral development in ADHD, beyond core ADHD symptoms.
Findings
ADHD is linked to emotional reactivity, aggression, and poor decision-making, which impair moral reasoning and prosocial behavior.
Attachment insecurity and emotional dysregulation are key developmental risk factors for moral development difficulties in ADHD.
Peer rejection and bullying are common in children with ADHD, contributing to long-term socio-emotional risks.
Abstract
What are the main findings? Moral development impairments in children and adolescents with ADHD emerge from the interaction of multiple developmental domains, including early attachment insecurity, difficult temperament, emotional dysregulation, altered reward processing, and social dysfunction, rather than from ADHD symptoms alone.Across studies, ADHD was consistently associated with delay aversion, reduced fairness and future-oriented decision-making, heightened emotional reactivity and aggression (especially in the presence of CU traits), and increased peer rejection and bullying involvement, all of which compromise moral reasoning, empathy, and prosocial behavior. Moral development impairments in children and adolescents with ADHD emerge from the interaction of multiple developmental domains, including early attachment insecurity, difficult temperament, emotional dysregulation,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
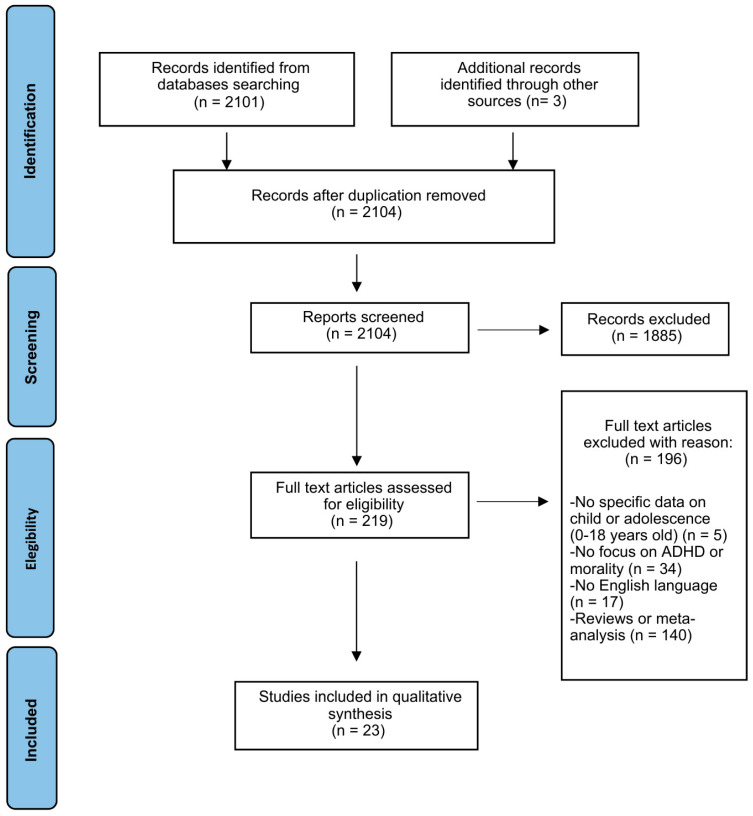 Figure 1
Figure 1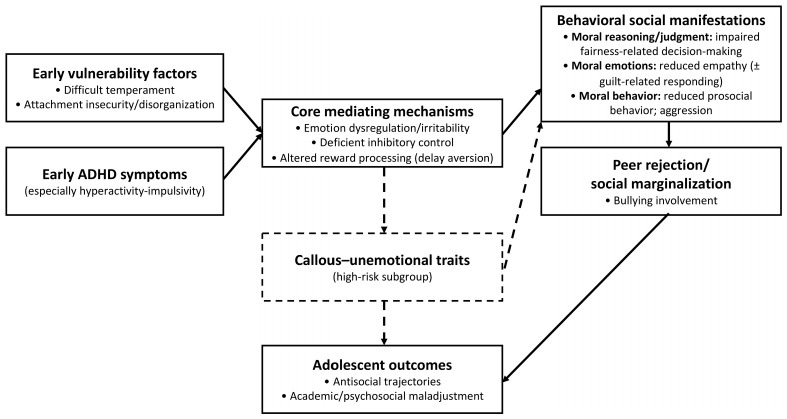 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAttention Deficit Hyperactivity Disorder · Personality Disorders and Psychopathology · Child and Adolescent Psychosocial and Emotional Development
1. Introduction
The relationship between moral development (MD) and Attention-Deficit/Hyperactivity Disorder (ADHD) is complex and multidimensional, with significant implications for understanding socio-emotional trajectories in childhood and adolescence. MD begins early in life and is shaped by several interacting factors, including attachment quality, temperament, emotion regulation abilities, and decision-making processes [1,2]. In developmental science, MD is not a unitary construct but a set of partially dissociable processes unfolding across childhood and adolescence. For clarity, we distinguish three complementary domains: (i) moral reasoning/judgment, referring to cognitive evaluations of right–wrong, fairness, intentions, and norm understanding; (ii) moral emotions, including affective dispositions that support concern for others (e.g., empathic concern) and self-evaluative responses (e.g., guilt/shame) that promote reparative behavior; and (iii) moral behavior, namely observable conduct in social contexts, including prosocial actions (helping, sharing, cooperation) and the regulation of aggression, bullying, and rule-breaking. Importantly, constructs such as emotion regulation, reward sensitivity/decision-making, and broader social functioning are discussed in this review primarily as mechanisms and socio-developmental correlates that shape moral outcomes, rather than as synonymous with MD itself [3]. Conceptually, MD can be understood as emerging from the interplay between self-regulatory capacities (e.g., inhibitory control, affect regulation, sensitivity to reward and punishment), social cognitive processes (e.g., interpreting intentions and evaluating fairness), and relational contexts (e.g., caregiver co-regulation and peer inclusion/exclusion) [3,4]. Within this integrative perspective, ADHD-related vulnerabilities may contribute to differentiated moral trajectories not only through core symptoms, but also through associated difficulties in emotion regulation, reward-based decision-making [5,6], and social functioning [4] that shape everyday opportunities for moral learning [1,3]. Among these, early attachment experiences represent a foundational dimension. Attachment refers to a deep and enduring emotional bond connecting individuals across time and space [7]. Classic work by Ainsworth [8] identified four attachment styles—secure, insecure-avoidant, insecure-ambivalent, and disorganized—each associated with different socio-emotional outcomes. Bowlby’s theory posits that early caregiver-child relationships directly influence emotional regulation, social competence, and the development of moral understanding [7]. Wilson [9] further emphasized that a secure attachment base facilitates the natural progression of MD, as children increasingly rely on moral reasoning to navigate social groups and relationships.
Empirical research has consistently documented associations between insecure or disorganized attachment and externalizing behaviors [10,11]. More broadly, insecure attachments are linked to hostility, avoidance, aggression, emotional instability, and anxiety [12]. Difficulties in emotion regulation—a core challenge for many children with ADHD—further amplify these risks. Estimates indicate that 55–75% of children with ADHD exhibit marked emotional dysregulation [13,14]. Conversely, secure attachment promotes emotional regulation, perspective-taking, and the development of a coherent moral framework [3]. Children with disorganized attachment often struggle to implement consistent behavioral strategies in high-stress situations, undermining adaptive moral decision-making [15]. A longitudinal empirical study by Bohlin et al. [16] highlighted strong associations between ADHD symptoms and insecure, particularly disorganized, attachment, partly mediated by deficits in self-regulatory and temperamental functioning. These children may elicit suboptimal caregiving responses, particularly when caregivers have limited tolerance for ADHD-related behaviors [17].
Temperamental self-regulatory capacities emerge early and remain relatively stable across development, shaping the child’s ability to manage emotions and behaviors [18]. Difficult temperament—marked by low adaptability and high negative emotionality—is a well-established risk factor for ADHD symptoms [13]. When combined with deficits in behavioral inhibition, emotional dysregulation may fuel impulsive and aggressive behaviors, particularly under stress. Aggression in children with ADHD can manifest in reactive, emotionally driven responses or in proactive, goal-directed behaviors with minimal emotional involvement, often reinforced through external rewards within peer or familial contexts [19,20]. Such deficits in self-control impede moral and social development and predict adverse academic and occupational outcomes across the lifespan [21,22].
The ability to delay gratification and prioritize long-term benefits represents another key component of MD. From a neurodevelopmental perspective, aberrant reward sensitivity and altered motivational processes have long been implicated in ADHD [5,6]. These alterations contribute to maladaptive decision-making, including risk-taking behaviors, increased accidents, and difficulties in negotiating social interactions [23]. Social dysfunction—characterized by reduced prosocial behaviors and unstable relationships—is a major negative consequence of ADHD and predicts long-term difficulties such as delinquency, anxiety, and broader psychosocial impairments [4].
MD also depends on the accurate perception and interpretation of social cues and on the ability to enact appropriate interpersonal responses. Deficits in these capacities increase the likelihood of confrontational or provocative behaviors, including involvement in bullying. Bullying, defined as repeated intentional aggression toward a weaker individual [24,25], is associated with academic underachievement, substance misuse, aggression, and adverse developmental outcomes [26].
Despite these converging strands of evidence, no systematic review to date has integrated attachment, temperament, emotional dysregulation, reward sensitivity, aggression, and social functioning to clarify how these domains intersect with MD among children and adolescents with ADHD. In particular, prior work has often examined these domains in isolation, leaving unclear how they jointly map onto distinct components of MD (moral reasoning/judgment, moral emotions, and moral behavior) across development in youth with ADHD, and which moderators (e.g., comorbid ODD/CD and family adversity) may account for heterogeneity in outcomes. Clarifying these links is clinically and educationally relevant because “moral difficulties” in ADHD may reflect different underlying pathways that call for different assessment priorities and intervention targets.
The present systematic review therefore aims to (1) synthesize evidence on how ADHD relates to distinct components of MD (moral reasoning/judgment, moral emotions, and moral behavior) across childhood and adolescence; (2) examine how key developmental mechanisms and contexts—attachment, temperament, emotion regulation/irritability, and reward processing/delay-related decision-making—may shape these moral trajectories; and (3) describe behavioral and social correlates (e.g., aggression, bullying involvement, peer difficulties) and major moderators (e.g., comorbid ODD/CD and family adversity) relevant to clinical and educational practice.
2. Materials and Methods
2.1. Study Design and Reporting
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [27]. The PRISMA flowchart summarizing the selection process is presented in Figure 1, and the PRISMA 2020 checklists are provided in the Supplementary Materials (Files S1 and S2). The review protocol was not registered.
2.2. Eligibility Criteria
Studies were included if they met the following criteria: (a) original empirical research published in English or with an available English translation; (b) participants aged 0–18 years diagnosed with ADHD or presenting subclinical ADHD symptoms; (c) assessment of MD-related constructs, including moral reasoning, fairness, aggression, bullying, callous–unemotional (CU) traits, decision-making, reward sensitivity, emotion regulation, or social functioning; and (d) quantitative or qualitative empirical designs. Exclusion criteria were (a) studies in which child/adolescent data were not distinguishable from adult samples; (b) studies focusing exclusively on adult populations; (c) studies focusing exclusively on ADHD comorbidities with no MD-related outcomes; and (d) case reports/series, editorials, book chapters, letters, commentaries, and review articles.
2.3. Information Sources
A systematic search was performed using the PubMed database to identify studies published between January 2014 and November 2024. Reference lists of previous reviews were also screened. The last search was conducted on 5 November 2024.
2.4. Search Strategy
The PubMed search used the following Boolean algorithm: ((ADHD OR attention deficit* hyperactivity disorder*) AND (moral* development* OR fairness OR moral deficit* OR behaviour*) AND (child* OR pediatric* OR kids OR scholar OR adolescence OR adolescent* OR teenager*)). Keywords and MeSH terms were combined to maximize sensitivity. An additional manual search of citations in eligible articles was performed.
2.5. Selection Process
Three reviewers independently screened all records in two phases: (1) title and abstract screening and (2) full-text evaluation based on predefined eligibility criteria. Reasons for exclusion at the full-text stage were systematically documented. Discrepancies were resolved through discussion and, when necessary, consultation with a fourth reviewer until consensus was reached. A total of 2104 records were identified; after screening, 23 studies were included.
2.6. Data Collection Process and Data Items
Data were extracted independently by three reviewers using a standardized Excel spreadsheet designed according to the PICO framework (Population, Intervention/Exposure, Comparison, Outcome). A fourth reviewer verified all extracted data for accuracy. Extracted variables included: study design, socioeconomic context, sample characteristics (age, gender, size, controls), ADHD diagnostic criteria or measures, constructs related to MD, methods and instruments used, key findings, quality assessment score. Additional information included first author’s name, year of publication, and country of origin.
2.7. Quality Assessment
Methodological quality was evaluated using a quality index derived from the Newcastle–Ottawa Scale (NOS) adapted to cross-sectional and longitudinal designs [28]. Each study was assigned a score based on selection, comparability, and outcome domains. Full details are provided in Supplementary Tables S1 and S2.
2.8. Synthesis Methods
Due to substantial heterogeneity across study designs, populations, and outcome measures, a qualitative thematic synthesis was performed. Studies were grouped into conceptual domains relevant to MD processes: (1) attachment and temperament; (2) emotion regulation and aggression; (3) CU traits; (4) reward sensitivity and decision-making; and (5) social functioning and bullying. Patterns were summarized, and explanatory mechanisms were explored.
3. Results
Figure 1 presents the PRISMA flow diagram. A total of 23 studies met the inclusion criteria and were included in the final synthesis. To facilitate interpretation, findings are discussed in relation to the three MD components (moral reasoning/judgment, moral emotions, moral behavior), while results are organized into thematic developmental domains (attachment/temperament, reward-based decision-making, emotion dysregulation/CU traits, and social functioning/bullying) hypothesized to shape moral outcomes, which are discussed in this review as developmental mechanisms/correlates rather than MD components per se. Table 1 summarizes the characteristics of the included studies, while Supplementary Tables S1 and S2 report the quality assessment.
3.1. General Characteristics of the Studies
Quality scores ranged from 4 to 7 out of 9 on the adapted Newcastle–Ottawa Scale, with a mean of 6.21 and a median of 6, indicating moderate methodological quality [52]. Twelve studies adopted a longitudinal design, while eleven were cross-sectional; among these, five used a case–control approach. Sample sizes ranged from 57 to 125,621 participants, with ages spanning 2–18 years. In total, the review included data from 146,314 individuals across fifteen countries. Most studies were conducted in Europe (17 studies; Netherlands, United Kingdom, Finland, Sweden, Portugal, Switzerland, Belgium). Others were carried out in the United States (3), China (1), Thailand (1), Malaysia (1), and Canada (1). Socioeconomic context was assessed in only five studies, and inconsistently across them. Studies were grouped according to the main constructs examined and the measures employed (see Table 1).
3.2. Attachment and Temperament as Early Foundations of Moral Development
Two studies examined early relational and temperamental precursors of MD. Forslund et al. [32] and Morales et al. [37] found that disorganized attachment was associated with conduct problems, but not directly with ADHD symptoms. Building on this developmental perspective, Wu et al. [50] examined the long-term influence of early temperament. Difficult temperament at age 2 predicted a higher likelihood of becoming NEET (Not in Education, Employment, or Training) in adulthood. Hyperactivity-impulsivity symptoms mediated the pathway from difficult temperament to NEET status, whereas inattention did not. Adolescent antisocial behaviors further contributed to this developmental trajectory [50]. In adolescence, temperament profiles have also been associated with socio-emotional functioning relevant to moral behavior. In a cross-sectional study, Deotto et al. [31] reported that high harm avoidance and low self-directedness were associated with internalizing symptoms in adolescents with ADHD, whereas low cooperativeness was linked to externalizing behaviors, independently of ADHD severity and working memory performance.
3.3. Reward Anticipation and Decision-Making in ADHD
Five studies focused on reward processing and decision-making. Across all studies, children and adolescents with ADHD consistently preferred immediate, smaller rewards over delayed, larger ones. Using the Ultimatum and Dictator Games, Ma et al. [34] found that individuals with ADHD made lower and more self-serving offers than typically developing peers, prioritizing personal gain over fairness. Northover et al. [38] reported that youth with ADHD and comorbid Conduct Disorder were more likely to reject moderately unfair or ambiguous offers, reflecting heightened emotional reactivity. Mies et al. [36] observed increased impatience and lower tolerance for delay in gain-related conditions among children with ADHD. Van Dessel et al. [47] expanded on these findings at the neural level using functional MRI: although overall activation during monetary loss processing did not differ between groups, controls showed greater ventral striatum activity during loss avoidance. By contrast, ADHD participants exhibited reduced sensitivity to positive feedback and increased anterior insula activation to negative feedback. Kostyrka-Allchorne et al. [33] demonstrated that heightened preference for immediacy co-occurred with reduced capacity for future-oriented thinking. Importantly, impaired simulation of future rewards did not mitigate delay aversion. These deficits remained significant after adjusting for aggression [33].
3.4. Emotional Dysregulation, Aggression, and Moral Challenges
Nine studies examined emotional dysregulation and its association with aggressive and disruptive behaviors. Waller et al. [48] and Speyer et al. [43] emphasized that aggression in ADHD is heterogeneous, with distinct reactive and proactive components associated with divergent developmental risks, including academic failure, peer rejection, and involvement in the juvenile justice system. Marques et al. [35] identified inhibitory control deficits as contributors to emotional dysregulation, which mediated the link between ADHD symptoms and aggression. Colonna et al. [30] reported strong associations between irritability—a core component of emotional dysregulation—and executive dysfunction. Several studies investigated CU traits. Zhang et al. [51] found that CU traits in Chinese preschoolers with ADHD predicted more severe behavioral problems. Similarly, Waller et al. [48] identified CU traits and oppositional behaviors as markers of early risk for conduct problems in ADHD. Thorell et al. [45] showed that both emotional dysregulation and ADHD symptoms predicted peer rejection and difficulties with cooperative interactions over time. Tengsujaritkul et al. [46] highlighted the broader academic and social impairments associated with emotional and behavioral difficulties in ADHD.
3.5. Social Functioning and Bullying
Three studies reported clear associations between ADHD and increased aggression. Bartels et al. [29] showed age-dependent patterns, with ADHD more strongly associated with physical aggression in childhood and rule-breaking behaviors in adolescence. Studies from the Swiss Z-proso project found developmental continuity: Speyer et al. [44] reported that ADHD symptoms at age 7 predicted externalizing behaviors at age 9, which in turn predicted a resurgence of ADHD symptoms at age 11. Ribeaud et al. [41] documented persistent ADHD symptoms from ages 7–17 predicting long-term externalizing behaviors. However, not all findings were consistent. Ramsey et al. [40] observed only a marginal association between ADHD symptoms and rule-breaking, and no significant link with aggression; instead, aggression was more strongly associated with anger. Broader social outcomes were addressed by Savolainen et al. [42], who reported links between ADHD, academic difficulties, peer marginalization, and alcohol use. Notably, ADHD—but not Conduct Disorder—was uniquely related to peer marginalization. Wan Ismail et al. [49] found that social isolation associated with ADHD reduced opportunities for bullying perpetration. In contrast, hyperactive and inattentive symptoms individually increased the likelihood of bullying behaviors, whereas the combined presence of inattention and hyperactivity showed a protective association. The authors also identified oppositional defiant disorder (ODD) and conduct disorder (CD) as mediating and moderating factors in the persistence of aggressive and bullying behaviors. Rajendran et al. [39] similarly reported higher bullying involvement among children with ADHD, both with and without ODD, and identified parenting practices—specifically negative affectivity and promotion of excessive autonomy—as predictors of bullying.
3.6. Overall Synthesis
Taken together, findings across the 23 included studies indicate that children and adolescents with ADHD present multidimensional vulnerabilities in MD. Early attachment and temperament contribute to later socio-emotional outcomes; impairments in reward processing and future-oriented thinking affect fairness and decision-making; emotional dysregulation and CU traits shape aggressive behavior; and social dysfunction influences involvement in bullying and long-term maladaptive trajectories.
4. Discussion
This systematic review synthesizes evidence from 23 studies investigating how core developmental domains—attachment, temperament, emotion regulation, reward processing, and social functioning—intersect with MD in children and adolescents with ADHD. Across the included studies, diverse patterns emerged that point to multiple potential mechanisms connecting ADHD-related characteristics with aspects of MD. These findings offer a foundation for interpreting how developmental and socio-relational processes may influence moral reasoning, fairness, empathy, and prosocial behavior in youth with ADHD. Given the heterogeneity of study designs and the predominance of cross-sectional evidence, the associations discussed below should not be interpreted as causal pathways. Rather, we integrate findings across domains as a qualitative framework to highlight converging mechanisms and sources of heterogeneity in socio-moral outcomes among youth with ADHD.
4.1. Attachment, Temperament, and Early Relational Foundations of Moral Development
Across the included studies, insecure or disorganized attachment emerged as an early relational risk factor for socio-behavioral outcomes relevant to MD. Although disorganized attachment was associated with both ADHD symptoms and conduct problems, findings consistently showed that its independent association was stronger for conduct-related outcomes than for ADHD symptoms per se. In this regard, the authors suggested that the apparent association between disorganized attachment and ADHD may be partly explained by the high comorbidity between ADHD and conduct disorders. In those studies, conduct problems were reported to be more closely related to negative emotionality and inconsistent stress responses typically observed in disorganized attachment, whereas ADHD symptoms were more closely related to inhibitory control difficulties and regulation of positive emotions [32,37]. These results also align with broader literature suggesting that apparent attachment disorganization in ADHD may reflect difficulties in behavioral and emotional self-regulation—sometimes described as “pseudo-disorganization”—rather than true attachment system disruption [32]. From a clinical standpoint, these findings are consistent with the possibility of differentiated pathways to moral difficulties among youth with ADHD. In a relational-adversity pathway, disorganized attachment may index early caregiving stress and inconsistent co-regulation and appears more proximally linked to conduct-related/externalizing outcomes than to ADHD symptoms per se [32,37]. In parallel, a neurodevelopmental self-regulatory pathway—involving inhibitory control, reward-based learning/delay-related decision-making, and emotion regulation—may shape day-to-day moral decision-making and behavior in ADHD without necessarily implying attachment system disruption [5,6,14]. Importantly, these pathways may co-occur and interact in clinical presentations, underscoring the need to interpret moral difficulties in ADHD as potentially arising from distinct—yet converging—relational and self-regulatory mechanisms. Secure attachment, conversely, supports emotional regulation and perspective-taking [3], capacities essential to the development of empathy and moral reasoning. Temperamental factors added an additional layer of early vulnerability. Difficult temperament in toddlerhood predicted long-term negative outcomes [50], with hyperactivity-impulsivity mediating pathways from early negative emotionality to adolescent antisocial behavior. These findings complement theoretical models that conceptualize temperament as an early-developing regulatory system shaping emotional reactivity and self-control [18]. In this context, high reactivity and low effortful control may undermine early moral learning by increasing frustration, reducing compliance, and heightening conflictual interactions with caregivers.
4.2. Reward Processing, Delay Aversion, and Fairness-Related Decision-Making
A consistent theme across studies was altered reward processing in ADHD. Children with ADHD demonstrated a pronounced preference for smaller immediate rewards over larger delayed ones [33,36], particularly in gain- oriented contexts. These preferences mirror well-established motivational alterations in ADHD, including heightened reward sensitivity and difficulty sustaining motivation across delays [5,6]. Neuroimaging findings further showed reduced ventral striatum activation during reward anticipation and heightened anterior insula activation to negative feedback [47], suggesting altered integration of reward value and feedback valence. Such abnormalities have direct implications for MD. In fairness-related tasks, including the Ultimatum and Dictator Games, children with ADHD made more self-serving offers or showed heightened rejection of ambiguous offers [34,38]. Reduced responsiveness to social rewards compared to monetary ones [53] may undermine cooperative behaviors and limit opportunities to internalize social norms. Ultimately, difficulties evaluating future consequences and balancing self-interest with fairness can compromise moral judgment and prosocial decision-making.
4.3. Emotional Dysregulation, Irritability, and Moral Competence
Emotional dysregulation emerged as a central mechanism linking ADHD to aggression, irritability, and interpersonal difficulties. Several studies highlighted associations between inhibitory control deficits, frustration intolerance, and aggressive behavior [30,35]. These findings converge with broader evidence that 55–75% of children with ADHD experience significant emotional dysregulation [14], and that irritability represents a critical affective dimension contributing to reactive aggression [54]. Such emotional vulnerabilities can disrupt moral learning by impairing children’s ability to consider others’ perspectives, regulate anger, or resolve conflicts constructively. Social consequences of emotional dysregulation were also evident. Studies consistently showed that ADHD symptoms and emotional difficulties predicted peer rejection, unstable friendships, and challenges in cooperative play [43,45,48]. These relational difficulties reduce access to positive peer models and prosocial feedback, potentially undermining opportunities to develop empathy reciprocity, and moral understanding. CU traits represented an especially high-risk profile. Children with ADHD and elevated CU traits showed more severe and persistent aggression [48,51]. Reduced guilt, diminished empathic concern, and insensitivity to punishment—features characteristic of CU traits—present additional obstacles for MD and may require more targeted intervention, particularly in cross-cultural contexts.
4.4. Social Functioning, Peer Dynamics, and Bullying Involvement
Social functioning emerged as a pivotal domain through which ADHD affects MD. Hyperactivity, inattention, and emotional dysregulation predicted increased aggression, rule-breaking, and externalizing behaviors [29,41,44]. Comorbid ODD and CD further heightened risks for bullying involvement [39].
Peer marginalization played a particularly important role. ADHD symptoms—independent of conduct problems—were associated with peer rejection and social exclusion [42], consistent with evidence that ADHD is linked to reduced prosocial behaviors and unstable peer relationships [4]. These experiences may hinder moral learning by limiting exposure to cooperative interactions and opportunities to practice moral reasoning in dyadic and group settings. Bullying involvement followed complex patterns. Children with ADHD were more likely to be perpetrators, victims, or bully victims [49], with gender differences suggesting that boys tend to show more perpetration, while girls are more frequently victimized. Additional risk factors—including emotional dysregulation, academic challenges, and socioeconomic adversity—further contributed to bullying dynamics. Behavioral and social impairments also extended to academic contexts, with emotional and behavioral dysregulation negatively affecting school engagement and performance [46]. These patterns underscore how ADHD-related difficulties in cognition, emotion, and social interaction jointly shape MD-relevant outcomes.
4.5. Integrative Interpretation Across Domains
Overall, findings from the 23 included studies converge on a multidimensional developmental model. Early attachment insecurity and difficult temperament disrupt emotional regulation and behavioral control. Altered reward processing biases children toward immediate gratification and reduces sensitivity to fairness and social incentives. Emotional dysregulation and CU traits intensify aggressive tendencies and diminish empathy. Peer rejection, social exclusion, and bullying involvement limit opportunities for positive social learning. Importantly, across studies, moral behavioral outcomes (e.g., aggression, rule-breaking, bullying involvement) were most consistently amplified in the presence of key moderators such as comorbid ODD/CD and family adversity (e.g., chronic stress and socioeconomic disadvantage), which likely contribute to heterogeneity in “moral difficulties” observed in ADHD. These interconnected domains suggest that socio-moral functioning in ADHD can be understood as emerging from the interplay between self-regulatory capacities (e.g., inhibitory control, affect regulation, delay-related decision-making), social cognitive processes (e.g., intention understanding, fairness evaluation), and relational contexts (e.g., caregiver co-regulation and peer inclusion/exclusion). The empirical evidence synthesized here supports consistent associations across these domains; however, the proposed pathways should be considered a qualitative, hypothesis-generating framework rather than a causal account, and require longitudinal testing to establish temporal ordering and mechanisms.
To summarize the qualitative synthesis and provide an integrative framework for the intertwined pathways linking ADHD to MD difficulties across domains, we present a conceptual flowchart in Figure 2.
4.6. Clinical and Educational Implications
The present synthesis suggests that socio-moral difficulties observed in youth with ADHD should be assessed beyond core symptoms, by systematically considering key moderators and targets such as comorbid ODD/CD and callous–unemotional traits, family adversity and caregiving stress, emotion dysregulation/irritability, reward-based decision-making (delay aversion), and peer functioning (peer rejection and bullying involvement). Clinically, these domains may help differentiate heterogeneous developmental pathways and refine case formulation and intervention priorities. In practice, interventions may be most effective when they integrate established ADHD care (behavioral and educational supports, with pharmacotherapy when indicated) with components targeting emotion regulation and social decision-making in everyday contexts [55]. When peer dynamics and bullying are prominent, coordinated, whole-school preventive approaches may be warranted alongside clinical care [56].
4.7. Limitations and Future Directions
Several limitations should be considered when interpreting the findings of this review. First, the search strategy was restricted to PubMed and the review protocol was not preregistered (e.g., PROSPERO); therefore, relevant studies indexed primarily in other databases may have been missed, selective reporting cannot be fully excluded, and publication bias cannot be ruled out. Second, the included studies exhibited substantial methodological heterogeneity in terms of design, measures of MD, and assessment of ADHD-related characteristics. This variability limited direct comparisons and precluded the possibility of conducting a quantitative meta-analysis, so conclusions should be interpreted as a qualitative, hypothesis-generating synthesis rather than as precise pooled estimates. Third, we did not conduct a formal assessment of the overall certainty of the body of evidence (e.g., GRADE), which further supports cautious interpretation of the strength of the inferences. Fourth, the geographic distribution of the studies was uneven, with most research conducted in Europe and North America, limiting the cultural generalizability of the findings. Fifth, many studies did not comprehensively address comorbidities such as ODD, CD, or internalizing symptoms, despite their known influence on socio-emotional functioning and MD. Finally, most evidence was cross-sectional or based on short-term longitudinal designs, restricting the ability to draw causal inferences about developmental trajectories. Several avenues for future research emerge from these limitations. Expanding investigations to underrepresented regions and cultural contexts is essential for improving ecological validity and capturing culturally specific pathways to MD. More rigorous attention to comorbidity would allow for a clearer understanding of how overlapping conditions shape MD in ADHD. Longitudinal studies spanning childhood through adolescence are particularly needed to clarify causal mechanisms and identify sensitive developmental periods for intervention. Multidisciplinary approaches integrating developmental psychology, education, and neurobiological methods—including advanced neuroimaging and computational models—may elucidate the neural and cognitive bases of moral reasoning difficulties in ADHD. Additionally, refinement of experimental paradigms assessing reward sensitivity, social decision-making, and moral judgment would deepen our understanding of the specific processes involved. Finally, designing and evaluating targeted interventions that strengthen protective factors—such as secure attachment, emotion regulation skills, and social competence—represents a promising direction for supporting moral and socio-emotional development in children and adolescents with ADHD.
5. Conclusions
This systematic review highlights the multifaceted relationship between ADHD and MD, showing that ADHD extends beyond core neurodevelopmental symptoms to involve significant emotional, cognitive, and socio-relational dimensions relevant to moral functioning. Across the reviewed studies, difficulties in emotion regulation, impulse control, reward processing, and social interactions emerged as central mechanisms that may hinder the acquisition of moral competencies in children and adolescents with ADHD. By identifying key developmental pathways—from early attachment insecurity and difficult temperament to altered decision-making and peer-related challenges—this review provides a conceptual framework for understanding how ADHD intersects with moral reasoning, fairness, empathy, and prosocial behavior. These insights underscore the need for holistic and developmentally sensitive approaches in both clinical and educational settings. Supporting emotional regulation, strengthening caregiver–child relationships, and promoting positive peer experiences may contribute not only to improved behavioral regulation but also to the cultivation of moral growth and social integration in youth with ADHD. Taken together, these findings support assessment and intervention beyond core ADHD symptoms—toward emotion regulation/irritability, attachment security and caregiving stress, sensitivity to social reward and fairness-related decision-making, and broader socio-moral competencies relevant to peer functioning—while underscoring the need for longitudinal, cross-cultural, multi-method studies with rigorous control of key moderators to support causal conclusions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Groman C.M. Barzman D.H. The impact of ADHD on morality development Atten. Deficit Hyperact. Disord.20146677110.1007/s 12402-014-0131-424633571 · doi ↗ · pubmed ↗
- 2Costa Martins M. Santos A.F. Fernandes M. Veríssimo M. Attachment and the Development of Moral Emotions in Children and Adolescents: A Systematic Review Children 2021891510.3390/children 810091534682180 PMC 8534435 · doi ↗ · pubmed ↗
- 3Thompson R.A. Early moral development and attachment theory The Oxford Handbook of Parenting and Moral Development Laible D.J. Carlo G. Padilla-Walker L.M. Oxford University Press New York, NY, USA 2019213910.1093/oxfordhb/9780190638696.001.0001 · doi ↗
- 4Nijmeijer J.S. Minderaa R.B. Buitelaar J.K. Mulligan A. Hartman C.A. Hoekstra P.J. Attention-deficit/hyperactivity disorder and social dysfunctioning Clin. Psychol. Rev.20082869270810.1016/j.cpr.2007.10.00318036711 · doi ↗ · pubmed ↗
- 5Castellanos F.X. Sonuga-Barke E.J. Milham M.P. Tannock R. Characterizing cognition in ADHD: Beyond executive dysfunction Trends Cogn. Sci.20061011712310.1016/j.tics.2006.01.01116460990 · doi ↗ · pubmed ↗
- 6Luman M. Oosterlaan J. Sergeant J.A. The impact of reinforcement contingencies on AD/HD: A review and theoretical appraisal Clin. Psychol. Rev.20052518321310.1016/j.cpr.2004.11.00115642646 · doi ↗ · pubmed ↗
- 7Bowlby J. Attachment and Loss. 1: Attachment 2nd ed.Basic Books New York, NY, USA 2003
- 8Ainsworth M.S. The Development of Infant-Mother Attachment. A Final Report of the Office of Child Development 1974 Available online: https://eric.ed.gov/?id=ED 122924(accessed on 7 January 2025)