Efficacy of Phytotherapy for Cancer-Related Fatigue: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Silvio Matsas, Ursula Medeiros Araujo de Matos, Carolina Molina Llata, Auro del Giglio

TL;DR
This study reviews whether plant-based treatments can help reduce cancer-related fatigue, finding only modest effects and calling for better research.
Contribution
The study provides a meta-analysis of randomized trials on phytotherapy for cancer-related fatigue, highlighting the need for precision herbal oncology.
Findings
Phytotherapy showed a modest improvement in cancer-related fatigue (SMD = 0.31).
Subgroup analyses found only 'other formulations' showed significant benefit.
Most trials had high or unclear risk of bias, and evidence certainty was very low.
Abstract
Background: Cancer-related fatigue (CRF) is one of the most common and burdensome symptoms faced by patients with cancer, yet effective drug-based treatments remain limited. In recent years, phytotherapeutic agents have drawn attention as complementary options, supported by plausible anti-inflammatory, antioxidant, and immunomodulatory mechanisms. Methods: We performed a systematic review and meta-analysis to quantitatively synthesize randomized controlled trial evidence on the efficacy of phytotherapeutic interventions for cancer-related fatigue and to assess the certainty of evidence. Databases were searched from inception, with the final search update completed in October 2025. Eligible studies included adults with CRF and compared herbal interventions with placebo controls. Standardized mean differences (SMDs) were pooled using a DerSimonian–Laird random-effects model. We also…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1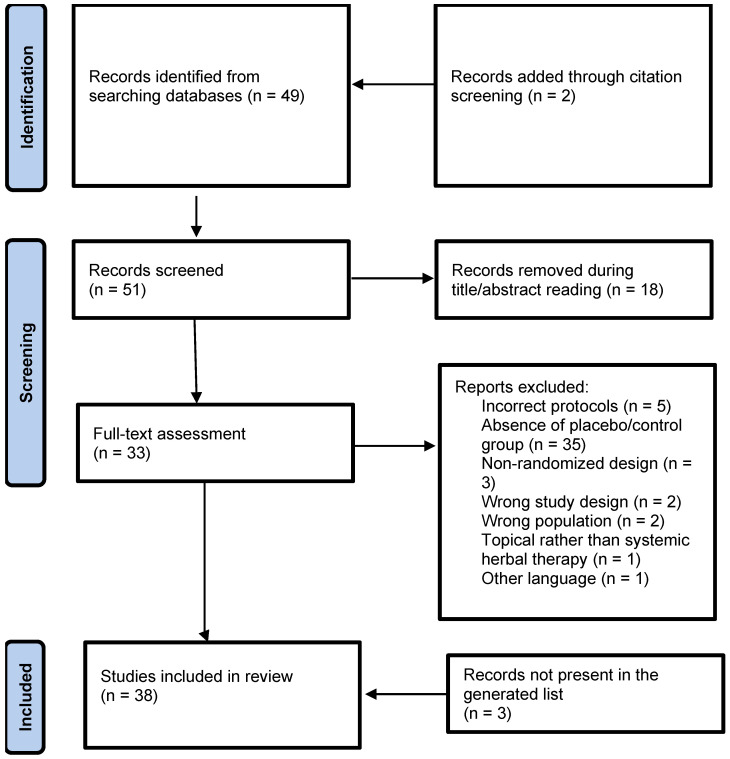 Figure 2
Figure 2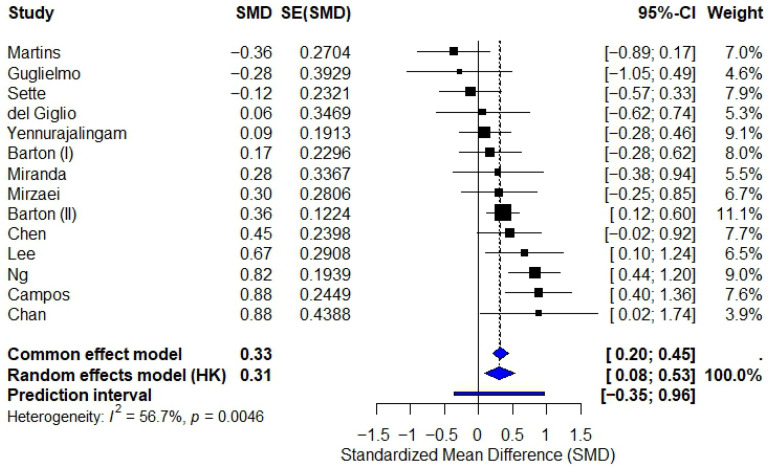 Figure 3
Figure 3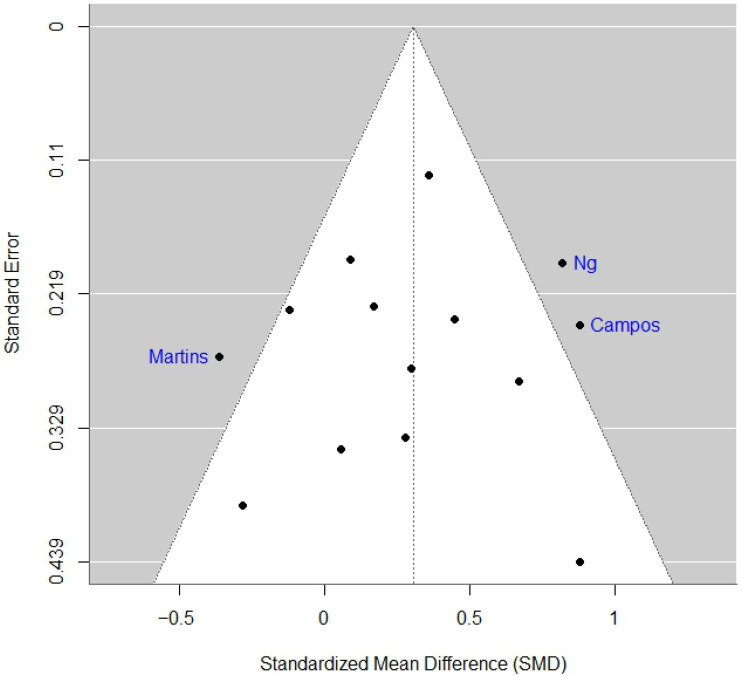 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Oral health in cancer treatment · Ginseng Biological Effects and Applications
1. Introduction
Cancer-related fatigue (CRF) is one of the most common and distressing symptoms experienced by patients with cancer, impacting up to 90% of individuals during active treatment and persisting in a substantial proportion of survivors [1]. CRF is highly prevalent in cancer populations, with some data indicating prevalences of 45.5% and 56.8% in Europe and North America, respectively [2]. Unlike ordinary tiredness, CRF is characterized by a pervasive sense of exhaustion that is disproportionate to activity and not relieved by rest [1]. Its multifactorial pathogenesis encompasses inflammatory activation, neuroendocrine dysregulation, metabolic alterations, mitochondrial dysfunction, sleep disturbance, anemia, and psychological distress [1,3,4].
Pharmacologic management of CRF remains challenging. Agents such as psychostimulants, corticosteroids, and erythropoiesis-stimulating agents provide limited benefit and may result in adverse effects [1,3]. Consequently, interest has grown in complementary and integrative approaches, including phytotherapeutic agents derived from medicinal plants such as Panax ginseng (C.A. Mey.), Paullinia cupana (Kunth), Uncaria tomentosa (Willd. ex Schult.) DC., and Zingiber zerumbet (L.) Roscoe ex Sm. [5,6]. Preclinical evidence suggests antioxidant, anti-inflammatory, and immunomodulatory effects through multiple mechanisms of action such as, respectively, direct free-radical scavenging, suppression of pro-inflammatory cytokines, and liver xenobiotic responses [7,8,9,10]. Taken together, these pieces of evidence may plausibly explain the target mechanisms underlying CRF.
Despite the biological plausibility of phytotherapeutic agents, their clinical role in the management of cancer-related fatigue remains uncertain. Most published trials are small, single-center studies with heterogeneous patient populations, variable herbal formulations, inconsistent dosing regimens, and differing fatigue assessment instruments. Moreover, the lack of standardized phytochemical characterization and limited methodological rigor across studies have contributed to inconsistent findings and imprecise effect estimates (a visual representation of the components contributing to insufficient evidence for herbal drug use in CRF can be seen in Figure 1). As a result, the available literature does not currently allow firm conclusions regarding the efficacy of phytotherapy for CRF, underscoring the need for a rigorous quantitative synthesis and critical appraisal of existing randomized evidence.
Therefore, a pooled study of published randomized controlled trials (RCTs) is needed. The primary objectives of this systematic review and meta-analysis were to quantitatively synthesize data from available RCTs, assess their methodological quality, and ultimately determine the strength of evidence concerning the efficacy of phytotherapy for CRF.
2. Methodology
2.1. Protocol and Registration
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11]. The study protocol was registered prospectively in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251235154. Study identification, screening, eligibility assessment, and inclusion were performed following PRISMA guidance, and the selection process is summarized using a PRISMA 2020 flow diagram. Data extraction, risk-of-bias assessment, and synthesis methods were implemented in line with PRISMA recommendations for transparency and reproducibility. The PRISMA checklist can be found in the Supplementary Materials.
2.2. Eligibility Criteria
Population, Intervention, Comparison, Outcomes, Study design (PICOS) criteria was adopted as follows:
- (a)Population (P)
Adult patients (≥18 years) with cancer-related fatigue, regardless of cancer type, stage, or treatment status.
(b)Intervention (I)
Any herbal intervention administered for fatigue management, including but not limited to the following:
-
-Ginseng (Panax ginseng, American ginseng);
-
-Guaraná (Paullinia cupana);
-
-Traditional Chinese Medicine formulations;
-
-Other plant-derived interventions.
-
(c)Comparison (C)
Placebo or standard of care control groups. Active comparator studies were excluded to maintain homogeneity.
(d)Outcomes (O)
Primary outcome: Fatigue severity measured by validated scales (BFI, FACIT-F, MFI, etc.)
Secondary outcomes: Quality of life measures, adverse events, dropout rates
(e)Study Design (S)
Randomized controlled trials (RCTs) published in peer-reviewed journals
2.3. Exclusion Criteria
(a)Studies without use of systemic phytotherapeutic agents;(b)Studies comparing a not-placebo group to phytotherapy;(c)Studies using a design other than RCT;(d)Studies written in other language than English.
2.4. Information Sources and Search Strategy
(a)Electronic Databases
The following databases were systematically searched from inception, with the final search update completed in October 2025: PubMed/MEDLINE, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar. We also consulted reference lists of included studies and relevant reviews for additional references.
(b)Search Strategy
Sample PubMed Search Strategy:
(“Fatigue”[Mesh] OR “Cancer Fatigue”[Mesh] OR fatigue[tiab] OR tiredness[tiab]) AND (“Neoplasms”[Mesh] OR cancer[tiab] OR oncology[tiab]) AND (“Plant Extracts”[Mesh] OR “Drugs, Chinese Herbal”[Mesh] OR herb*[tiab] OR ginseng[tiab] OR guarana[tiab] OR “traditional Chinese medicine”[tiab]) AND (randomized controlled trial[pt] OR randomized[tiab] OR placebo[tiab] OR randomly[tiab])
2.5. Study Selection Process
Two independent reviewers screened titles and abstracts using Rayyan software [12]. Prior to screening, eligibility criteria were predefined and piloted to ensure consistency in study selection. Each reviewer conducted the screening process blinded to the other’s decisions, and articles clearly not meeting inclusion criteria were excluded at this stage. Full-text articles of potentially eligible studies were then retrieved and assessed independently by the same reviewers to determine final eligibility. Discrepancies at either screening stage were resolved through discussion and consensus; when agreement could not be reached, a third reviewer adjudicated the decision.
2.6. Data Extraction and Management
Data were extracted independently by two reviewers using a standardized electronic data collection form developed in Microsoft Excel. The extraction form was piloted on a subset of included studies to ensure clarity, completeness, and consistency across reviewers. Extracted variables included study characteristics (design, setting, sample size), patient demographics, cancer type and treatment phase, details of the phytotherapeutic intervention, fatigue assessment instruments, outcome measures, and safety data. Following independent extraction, the datasets were cross-checked for accuracy and completeness. Any discrepancies between reviewers were resolved through discussion and consensus, with involvement of a third reviewer when necessary. When required, study authors were consulted for clarification of missing or unclear information.
2.7. Data Synthesis and Statistical Methods
Effect Measures, quality of evidence, and publication bias assessments:
For continuous outcomes, the Standardized Mean Difference (SMD) with 95% confidence intervals was calculated using Hedges’ g to account for small sample sizes [13]. The DerSimonian–Laird random-effects model was employed due to anticipated clinical and methodological heterogeneity among studies [14]. We assessed publication bias through Funnel plot analysis and we tested funnel plot asymmetry with Egger’s regression test. We conducted a Risk of Bias assessment using the Cochrane Risk of Bias 2 (RoB 2) tool [15].
We employed the R system for statistical computing (version 4.4.2; R Core Team, Vienna, Austria), using random effects model p value and heterogeneity calculations.
2.8. Ethical Considerations
As this study involved analysis of previously published aggregated data, no individual patient information was accessed or collected. Consequently, the study did not require approval from an institutional Ethics Committee. In addition, all included studies had obtained appropriate ethical approval and informed consent, as reported in their original publications.
3. Results
3.1. Study Selection
A total of 49 records were identified through database searches, with an additional 2 records identified through citation searching. After removal of 18 duplicates, 33 unique records proceeded to screening. All records were screened at the title and abstract level, and 33 reports were sought for full-text retrieval. Full texts were successfully obtained for 31 records, of which 17 were excluded for clearly predefined reasons: protocols (n = 5), absence of a placebo or control group (n = 5), non-randomized design (n = 3), wrong study design (n = 2), wrong population (n = 2), topical rather than systemic herbal therapy (n = 1), and foreign-language publication not translatable (n = 1).
Ultimately, 14 randomized controlled trials met eligibility criteria and were included in the review and meta-analysis [16,17,18,19,20,21,22,23,24,25,26,27,28,29]. The PRISMA 2020 flow diagram summarizing the study selection process is shown in Figure 2.
3.2. Characteristics of Included Studies
The 14 included trials (Table 1) evaluated a range of phytotherapeutic agents—most commonly guaraná, ginseng, ginger, and multi-herbal formulations—administered to patients with cancer-related fatigue (CRF) across various cancer types and treatment phases. Fatigue severity was measured using validated patient-reported instruments including FACIT-F, BFI, MFSI-SF, and SF-36 Vitality. The majority of trials were parallel-group, placebo-controlled RCTs, with sample sizes ranging from 34 to 310 participants.
3.3. Risk of Bias Assessment
Risk-of-bias assessment using the Cochrane RoB 2 tool revealed substantial methodological concerns. A total of 14 randomized controlled trials were evaluated using the Cochrane RoB 2 tool. Two studies were judged at low risk of bias, five showed some concerns, and six were classified as high risk. The primary domains contributing to downgraded judgments included issues in randomization procedures, lack of blinding, deviations from intended interventions, and risk of measurement bias in patient-reported fatigue outcomes. High-risk studies frequently involved open-label designs or unclear allocation concealment (Table 2).
3.4. Meta-Analysis of the Effect of Phytotherapy on Cancer-Related Fatigue
(a)Overall Effect
Across all 14 trials, the random-effects model demonstrated a significant effect of phytotherapy on CRF: Standardized Mean Difference (SMD): 0.31 (95% CI: 0.08 to 0.53; p = 0.0046; Heterogeneity: I^2^ = 56.7%). The corresponding forest plot is shown in Figure 3.
This finding indicates substantial inconsistency across trials, with individual effects ranging from large improvements to moderate worsening of fatigue.
The two most commonly studied herbal subgroups did not demonstrate a statistically significant or clinically meaningful benefit (Table 3). A more general subgroup—named as “Other herbal formulations”—which included diverse formulations had a statistically significant benefit.
3.5. Publication Bias
Funnel Plot and Statistical Tests
Visual inspection of the funnel plot (Figure 4) revealed moderate asymmetry, suggesting missing small-scale negative studies. Egger’s regression test showed no evidence of small-study effects (intercept = 0.41; 95% CI, −0.30 to 1.13; z = −0.31; p = 0.75), suggesting no strong evidence of publication bias, although interpretation should consider the substantial heterogeneity across trials.
3.6. Certainty of Evidence (GRADE)
Using the GRADE framework, the overall certainty of evidence for the effect of phytotherapy on cancer-related fatigue was rated as very low. Although all included studies were randomized controlled trials (RCTs), the evidence was downgraded across several domains. Risk of bias was a major concern, as only two trials were judged at low risk, while the remaining studies showed either some concerns or high risk—particularly regarding randomization procedures, blinding, and outcome measurement. Inconsistency was substantial (I^2^ = 56.7%), reflecting wide variation in effect estimates and non-overlapping confidence intervals that could not be fully explained by clinical or methodological differences. The overall results, however, point toward a significant improvement of CRF (SMD = 0.31; 95% CI 0.08 to 0.53). Although a significant Egger test (p = 0.75) was generated, suggesting low risk of publication bias, this type of bias cannot be excluded due to heterogeneity and the presence of small single-center studies; asymmetry remained plausible due to the predominance of small single-center trials. Subgroup analysis by herbal formulation had no significant results in all three subgroups. Taken together, these limitations resulted in a very low certainty rating, indicating that the true effect of phytotherapy on fatigue may be substantially different from the observed overall estimate.
4. Discussion
Use of herbal drugs and integrative approaches in cancer care has increased over time in various regions of the world, with herbal medicine representing the most frequently used form of complementary and alternative medicine among patients with cancer [30,31,32]. A large systematic review and meta-analysis including more than 800,000 patients from 44 countries estimated a global pooled prevalence of herbal medicine use of approximately 22%, with substantially higher rates reported in Africa (≈40%) and Asia (≈28%), and in low- and middle-income countries compared with high-income settings [30]. This underscores the need for structured investigations on the efficacy of these interventions.
This systematic review and meta-analysis synthesizes the most up-to-date evidence on phytotherapeutic interventions for cancer-related fatigue (CRF), incorporating 14 RCTs. The updated pooled analysis demonstrated a statistically significant effect favoring phytotherapy, although heterogeneity was substantial. Ginseng and Paullinia cupana were the most commonly investigated herbal drugs. Their subgroup analyses did not reveal statistically significant CRF benefit. The subgroup analysis for a composite of diverse other herbal formulations revealed a significant benefit. Taken together, these results cast significant discrepancies with the overall results and warrant careful interpretation.
Several factors likely contributed to the absence of statistically robust effects on individual herbal classes. First, many included trials were modest in sample size, reducing precision and increasing susceptibility to random variation. Second, methodological limitations were common, including unclear or high-risk randomization procedures, inadequate blinding, and issues related to outcome assessment. Third, heterogeneity in herbal composition, preparation, phytochemical standardization, dosing schedules, and patient populations made it challenging to compare results across studies. These issues reflect broader challenges in botanical research, where variability in extraction methods and phytochemical content may obscure true therapeutic effects [33].
Further challenges stem from limited funding availability for phytotherapy research [34]. Because many botanical agents cannot be patented in their natural or crude extract forms, traditional pharmaceutical funding mechanisms are less accessible [35]. This limitation results in underpowered single-center studies, inconsistent methodological quality, and limited long-term safety follow-up. These structural barriers restrict the development of robust clinical evidence and slow progress in understanding potential mechanisms of action, toxicity profiles, and interactions between phytotherapeutic agents and standard anticancer treatments.
Despite these limitations, phytotherapy remains biologically plausible. Many botanical compounds exhibit anti-inflammatory, antioxidant, immunomodulatory, neuroprotective, and mitochondrial-regulating effects, all of which align with proposed mechanisms underlying CRF pathophysiology [36,37,38,39,40]. Given CRF’s multifactorial nature, therapies composed of diverse bioactive phytochemicals may theoretically offer therapeutic advantages. However, biological plausibility does not substitute for high-certainty clinical evidence, and at present, results remain preliminary.
Our findings are also in opposition to some of the already published data. A meta-analysis with different inclusion criteria investigated the use of Guaraná for treatment CRF and found a significant benefit with the use of this component [41]. This underscores the significant imprecision of phytotherapeutic cancer studies evaluating CRF. Recent ASCO and ESMO studies were also partially discrepant on the use of herbal formulations for CRF [42,43]. While ASCO guideline states that American ginseng may be considered for patients with CRF > 4 weeks during active treatment, some ESMO panel members discourage any use of herbal formulations.
From a broader supportive oncology perspective, phytotherapy and rehabilitation-based interventions have been explored not only for cancer-related fatigue but also for other prevalent symptoms that substantially affect quality of life, including constipation, pain and sleep disturbance [44,45,46]. Integrative approaches combining lifestyle modification, physical rehabilitation, and selected phytotherapeutic agents have shown potential benefits across multiple symptom domains, particularly in supportive and survivorship settings, as highlighted in the recent supportive care literature [47]. Within this context, the findings of the present meta-analysis—characterized by substantial heterogeneity and variable treatment effects—suggest that a uniform, non-stratified application of phytotherapy for fatigue is unlikely to be optimal. Rather than undermining future research, the observed variability in outcomes may reflect underlying differences in patient characteristics, disease stage, treatment context, and phytochemical composition, thereby supporting the rationale for future stratified or precision-guided approaches. Current ASCO and ESMO guidelines do not recommend phytotherapeutic agents for cancer-related fatigue, prioritizing non-pharmacologic interventions due to insufficient high-quality evidence [42,43]. This position is consistent with the low certainty and substantial heterogeneity observed in the present analysis.
While most of the included studies had methodological limitations and a moderate or high risk of bias, a small number of high-quality randomized trials illustrate feasible methodological standards. Notably, the phase III study by Barton et al. [28] employed rigorous randomization, double-blind placebo control, and an almost standardized ginseng dosing. Similarly, the trial by Yennurajalingam et al. [16] demonstrated strong internal validity through careful patient selection, robust blinding, and comprehensive safety reporting. These studies highlight that well-designed phytotherapy trials in CRF are achievable and provide a framework to guide future research.
Our study has a number of limitations. The main limitation of this study is the inclusion of trials encompassing heterogeneous cancer types, diverse herbal formulations with varying compositions, dosages, and titration schedules, and interventions administered at different disease timepoints. This clinical and methodological heterogeneity substantially limits the ability to draw definitive conclusions regarding efficacy. Another limitation is wide subgroup confidence intervals, underscoring small subgroup sizes and imprecision. Therefore, the overall results should be interpreted carefully.
5. Conclusions
In conclusion, the current body of randomized evidence does not conclusively support phytotherapeutic agents for reducing CRF. The certainty of evidence is very low, driven by methodological limitations, substantial heterogeneity, and imprecision in effect estimates. This underscores the need for well-designed, adequately powered, multicenter RCTs using standardized herbal preparations. Such studies are essential to clarify the therapeutic potential of phytotherapy for CRF and determine whether specific agents or patient subgroups may truly benefit. Moreover, the perspective for future research include the compared analysis of original scientific publications. Such efforts will be crucial to translating the growing body of observational evidence into clinically actionable, evidence-based phytotherapeutic oncology recommendations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Campos M.P.O. Hassan B.J. Riechelmann R. Del Giglio A. Cancer-related fatigue: A practical review Ann. Oncol.2011221273127910.1093/annonc/mdq 45821325448 · doi ↗ · pubmed ↗
- 2Al Maqbali M. Al Sinani M. Al Naamani Z. Al Badi K. Tanash M.I. Prevalence of Fatigue in Patients With Cancer: A Systematic Review and Meta-Analysis J. Pain Symptom Manag.202161167189.e 1410.1016/j.jpainsymman.2020.07.03732768552 · doi ↗ · pubmed ↗
- 3Bower J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments Nat. Rev. Clin. Oncol.20141159760910.1038/nrclinonc.2014.12725113839 PMC 4664449 · doi ↗ · pubmed ↗
- 4Bower J.E. The role of neuro-immune interactions in cancer-related fatigue: Biobehavioral risk factors and mechanisms Cancer 201912535336410.1002/cncr.3179030602059 PMC 6502236 · doi ↗ · pubmed ↗
- 5Kwon C.Y. Lee B. Kong M. Lee S.H. Jung H.J. Kim K.I. Lee B. Effectiveness and safety of herbal medicine for cancer-related fatigue in lung cancer survivors: A systematic review and meta-analysis Phytother. Res.20213575177010.1002/ptr.686032929824 · doi ↗ · pubmed ↗
- 6Finnegan-John J. Molassiotis A. Richardson A. Ream E. A systematic review of complementary and alternative medicine interventions for the management of cancer-related fatigue Integr. Cancer Ther.20131227629010.1177/153473541348581623632236 · doi ↗ · pubmed ↗
- 7Anand K. Kaur Massaon H. Prabhakar P.K. Herbal Therapies in Cancer Patients: Managing Side Effects and Improving Quality of Life Sumat. Med. J.20247283710.32734/sumej.v 7i 1.14603 · doi ↗
- 8Yin S.Y. Wei W.C. Jian F.Y. Yang N.S. Therapeutic applications of herbal medicines for cancer patients Evid. Based Complement. Altern. Med.2013201330242610.1155/2013/302426 PMC 372718123956768 · doi ↗ · pubmed ↗