The Landscape of Clinical Trials in Never-Smoker Non-Small-Cell Lung Cancer: Registered Evidence and Persistent Gaps
Raquel Ramos, Carlos Sousa, Nuno Vale

TL;DR
This paper reviews clinical trials focused on lung cancer in never-smokers, highlighting treatment differences and gaps in research.
Contribution
The study provides a comprehensive analysis of clinical trial landscapes and identifies specific gaps in research for never-smoker lung cancer patients.
Findings
Many trials for never-smoker lung cancer lack molecular stratification and biomarker-guided designs.
Therapeutic evidence for never-smokers is often extrapolated from trials primarily involving smokers.
There is a need for more contemporary platform trials tailored to the unique biology of never-smoker lung cancer.
Abstract
An increasing number of people are developing lung cancer despite never having smoked. These tumours often behave differently and may carry specific molecular changes that can potentially guide treatment. Yet, much treatment evidence has historically been derived from trials that mainly include smokers, which may not fully represent never-smokers. In this review, we examine registered clinical trials that were specifically designed for never-smokers with lung cancer. We summarize what types of treatments were tested, how patients were selected, whether molecular testing was used to guide enrolment, and how trial activity has evolved over time. We also identify key gaps and propose priorities for future studies so that never-smokers with lung cancer can benefit from evidence generated in trials tailored to their condition. Addressing these gaps is essential to ensure that never-smoker…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
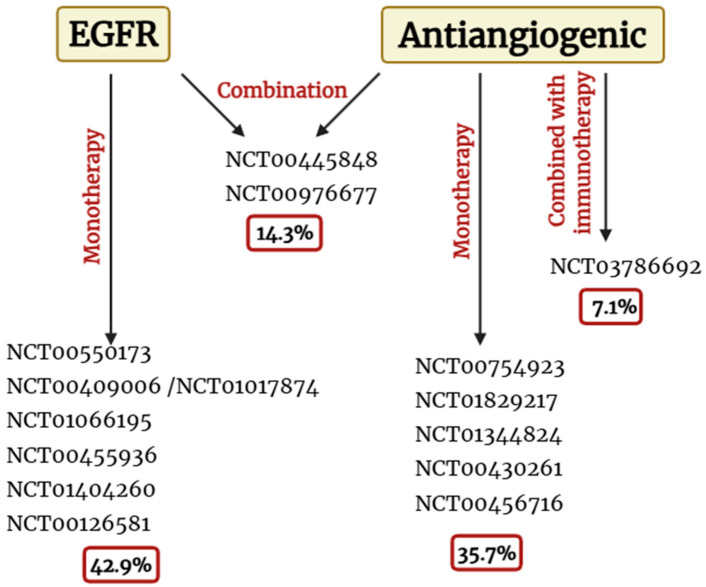 Figure 1
Figure 1- —FEDER—Fundo Europeu de Desenvolimento Regional
- —Portuguese funds
- —FCT and FEDER (European Union)
- —Chair of Onco-Innovation at the FMUP
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Research Studies · Lung Cancer Diagnosis and Treatment
1. Lung Cancer in Never-Smokers: An Emerging Entity
Lung cancer (LC) is the most prevalent cancer worldwide, with 2022 estimates reporting approximately 2.5 million new cases and 1.8 million deaths [1]. It remains one of the most complex cancers, being characterized by a late diagnosis and poor outcomes due to its non-specific symptoms—cough, dyspnea, fatigue, chest pain, and weight loss [2]. As is already known, tobacco smoking is the strongest risk factor for LC development, accounting for nearly 80% of cases. Nonetheless, there are other causes for LC development not related to tobacco [3].
Histologically, LC is a heterogeneous disease that can be divided into two major groups: non-small-cell lung cancer (NSCLC) and small-cell lung cancer (SCLC) [4]. Within these groups, SCLC is strongly associated with tobacco smoking, comprising 10–15% of all lung cancers. Otherwise, NSCLC is the most common lung cancer type, representing about 85% of cases. Among its subtypes, adenocarcinoma is the most common, occurring frequently among non-smoking females [5,6].
These histological and molecular differences have major therapeutic implications, supporting the shift toward biomarker-driven decision-making and, consequently, distinct patient outcomes and therapeutic approaches. In particular, once NSCLC is histologically classified, it should be further evaluated through multiple molecular methods, such as fluorescence in situ hybridization (FISH), immunohistochemistry (IHC), next-generation sequencing (NGS), and real-time polymerase chain reaction (RT-PCR) to detect genetic alterations with known targeted therapies [7,8]. Over the past decade, traditional chemotherapy and radiotherapy have been increasingly complemented and, in many cases, replaced by immunotherapy and targeted therapies directed at specific molecular alterations. These agents target identifiable oncogenic drivers or biomarkers, enabling more precise and effective treatment strategies while reducing the toxicity associated with conventional approaches [9]. Moreover, these genetic alterations are different between smokers and never-smokers, which suggests different mechanisms of tumour development in these patients (Table 1) [10,11]. Specifically, tumours arising in never-smokers commonly harbour EGFR mutations, mainly L858R in the exon 21 mutation. Also, gene fusions involving ALK, ROS, or PIK3CA were identified as being more common in never-smokers. Conversely, KRAS mutations occur less frequently in this population compared with tumours from smokers [11,12,13,14].
Moreover, recent research indicates that lung adenocarcinoma (LUAD) arising in never-smokers is characterized by a higher frequency of clinically actionable driver mutations than LUAD associated with smoking (78–92% versus 49.5%). Furthermore, RNA-sequencing analyses have identified distinct immune-related transcriptional subtypes in never-smoker LUADs, which differ in both the expression of therapeutically relevant immune checkpoint molecules and the composition of infiltrating immune cell populations [15]. At the same time, epigenetic mechanisms are increasingly recognized as key factors in differentiating NSCLC in smokers and never-smokers. A recent investigation provided an in-depth comparison of the epigenomic landscapes of these two patient groups, focusing on the role of DNA methylation alterations in shaping tumour phenotypes. The study identified recurrent promoter methylation changes associated with smoking status. Notably, tumours from never-smokers exhibited a higher prevalence of hypomethylated differentially methylated regions (hypoDMRs) and a greater number of consistently hypomethylated gene promoters, including ASPSCR1, TOP2A, DPP9, and USP39, previously implicated in cancer development [16].
As stated before, tobacco smoking is not the single determinant of lung cancer development, as multiple environmental and genetic factors also contribute. In reality, other risk factors are associated with this disease, namely environmental and occupational exposure, family history of lung cancer (genetic susceptibility), hormonal factors, and previous lung diseases [17,18,19]. In fact, the incidence of LC in never-smokers is around 20% and is increasing. Recent data indicate that the proportion of cases occurring in never-smokers has increased to approximately 17% in men and 24% in women [11,13].
Therefore, considering this increase in LC cases in never-smokers and the biological differences between smokers and never-smokers, it is obvious that the traditional focus on smoking is no longer enough. Accordingly, this article focuses on LC in people who have never smoked, investigating its unique characteristics, available therapies, and the respective current status of clinical trials in order to identify gaps and future directions for these patients.
2. Evolution of Therapeutic Clinical Trials in Never-Smokers
As with other diseases, several clinical trials have been conducted in LC to evaluate novel therapeutic strategies and improve patient outcomes. Over the past years, more attention has been given to the distinct clinical and biological characteristics of LC arising in never-smokers. Consequently, various clinical trials have been specifically designed to investigate therapeutic options in the never-smoker population, recognizing this group as a distinct clinical entity. Table 2 summarizes all the therapeutic clinical trials conducted in the past years that exclusively enrolled never-smokers with LC. The search was conducted in ClinicalTrials.gov without date restrictions. Only interventional studies were included in the analysis to examine the evolution of therapeutic strategies in this patient population, while observational and epidemiological studies were excluded. The search strategy used a combination of terms including “lung cancer”, “non-smoker”, and “never-smoker”.
All the studies presented before evaluated a range of therapeutic agents and molecular targets for a specific population of LC patients, carefully selected according to rigorous eligibility criteria. According to ClinicalTrials.gov, those criteria are similar among the studies and mainly include a confirmed diagnosis of NSCLC (locally advanced or metastatic disease), 18 years and older, and never-smokers (≤100 cigarettes in lifetime) or former light smokers (who smoked between >100 cigarettes and ≤10 pack-years and quit ≥1 year ago). Nonetheless, each trial presents some specific criteria, especially related to genetic characteristics and drug sensitivity. Specifically, some trials testing tyrosine kinase inhibitors (TKIs), namely erlotinib and gefitinib, in combination with other drugs (such as pemetrexed and bevacizumab) took into account EGFR mutations and/or tumour sensitivity to TKIs [20,25]. Another clinical trial (NCT01829217) selectively enrolled patients whose tumours were wild-type for EGFR, KRAS, and ALK or harboured a RET rearrangement, given sunitinib’s inhibitory activity against RET [24].
According to Table 2, more than half of the trials test an EGFR inhibitor—gefitinib or erlotinib—in monotherapy or in combination with an antiangiogenic drug (bevacizumab). In fact, most of them test EGFR inhibitors alone, which may reinforce the importance of TKIs in the treatment of LC. On the other hand, targeting angiogenesis also seems to be a promising therapeutic strategy, as approximately half of the studies evaluate antiangiogenic drugs. Among these, four studies investigate sorafenib or sunitinib in monotherapy. Sunitinib is currently approved for renal cell carcinoma (RCC), gastrointestinal stromal tumours (GISTs), and pancreatic neuroendocrine tumours, targeting vascular endothelial growth factor receptor 1 (VEGFR1) 1, VEGFR2, VEGFR3, PDGFR-α, PDGFR-β, fibroblast growth factor receptor 1 (FGFR1), fms-related tyrosine kinase 3 (FLT3), stem cell factor receptor (c-Kit), RET, MET proto-oncogene, and colony-stimulating factor 1 receptor (CSF1R) [32]. Similarly, sorafenib is primarily used to treat renal and liver cancer, and its mechanism of action involves inhibiting tumour angiogenesis and cell proliferation by targeting VEGFR and Raf kinase [33]. Although neither sunitinib nor sorafenib is approved for the treatment of LC, several of the molecular pathways targeted by these agents are known to be active in this cancer, particularly in NSCLC, such as VEGFR and the aberrant activation of RAF/MEK/ERK [34,35]. Therefore, the evaluation of sorafenib and sunitinib in lung cancer can reasonably be considered an example of drug repurposing, as these agents are being investigated outside their original approved indications based on shared oncogenic and angiogenic mechanisms.
Thus, considering the previous analysis, it is understandable that EGFR-targeted and antiangiogenic drugs were the main therapeutic focuses of these clinical trials. This fact may be justified by EGFR’s biological relevance in LC and due to the overall dependence of the tumour on angiogenesis in all molecular subtypes. Consequently, the clinical trials can be divided into the subgroups shown in Figure 1.
Nonetheless, despite the promising research conducted in this area and the generally encouraging results obtained, most of the clinical trials are relatively old, having been conducted between 2010 and 2015. This time window coincides with the early adoption of EGFR testing and the first wave of targeted therapy approvals in NSCLC, which largely shaped research priorities during that decade. A smaller number of studies were carried out between 2017 and 2019. However, the most recent trials are NCT00445848 and NCT03786692, conducted in 2020 and 2025, respectively. This fact, combined with the small number of clinical trials performed in this specific group of patients (only 14), highlights the limited research in this area. The concentration of studies conducted between 2010 and 2015 may be related to the period during which an increasing incidence of LC among non-smokers was first recognized, leading to the understanding that this population represents a distinct clinical and molecular subgroup. Conversely, the low number of trials in other years may be due to the historically small size of this patient group, which makes research more challenging and data more limited. Also, the historical focus of lung cancer research on smoking-associated disease may have reduced prioritization and funding for trials targeting never-smokers. However, in recent years, the incidence of lung cancer among never-smokers has been rising, emphasizing the growing need for targeted research in this population. Beyond smoking status, the integration of biomarker-driven enrollment has become crucial for including never-smokers, who are often enriched for actionable molecular alterations such as EGFR or ALK, allowing for their participation in clinical trials.
3. Perspectives and Future Directions—What Comes Next?
Despite some important steps forward, existing trials in never-smoker lung cancer remain fragmented and outdated, lacking the coherence and innovation seen in broader NSCLC research. The evidence presented in Section 2 showed us that despite some efforts in improving the therapeutic options for never-smoker LC patients, these attempts are older, disorganized, and lacking in a coherent strategy. Even today, most clinical trials in LC are conducted either in smoker populations or without accounting for smoking history, treating all lung cancer patients as a homogeneous group. However, it is well established that LC is a heterogeneous disease, and smoker and never-smoker patients must be treated as different entities. Accordingly, clinical trials should be designed to reflect this distinction.
As mentioned, the number of never-smoker LC patients has increased over the years, as well as the number of deaths, with this disease being the current fifth most common cause of cancer-related deaths worldwide [18]. Consequently, it is urgent to design and conduct new clinical trials specifically targeting never-smokers to better understand their tumour behaviour and discover new possible targeted therapies to improve their outcomes. On the other hand, despite this need, there remains a critical gap in the understanding of tumour genetics and molecular features in this specific population. As stated in Section 1, some genetic alterations are known to be more present in never-smokers than in smokers. However, to fully elucidate these differences and the molecular mechanisms, more translational research is needed, including comprehensive molecular profiling and multi-omics analyses—including genomics, transcriptomics, proteomics, metabolomics, and epigenomics. Such efforts may lead to the identification of novel actionable targets, the validation of predictive biomarkers, and guide biomarker-based clinical trial design. Collaboration between institutions is also crucial for faster results. Ultimately, integrating these insights into clinical trial design could optimize patient selection, improve therapeutic efficacy, evaluate new or repurposed drugs beyond the conventional EGFR and antiangiogenic therapies explored in earlier trials, and accelerate the development of personalized treatment strategies for never-smoker LC patients.
On the other hand, a study performed in a large NSCLC cohort showed that never-smokers were more likely to be diagnosed at an earlier stage (stage I–II) compared with smokers, suggesting differences in clinical presentation between these groups. In this scenario, surgical resection remains the mainstay of curative treatment [7,36]. The different molecular profiles and survival statuses between smokers and never-smokers may influence postoperative risk stratification and adjuvant treatment decisions. Therefore, future perioperative and adjuvant clinical trials specifically designed for never-smokers may help refine recurrence risk assessment and guide personalized adjuvant or neoadjuvant therapeutic strategies in early-stage disease.
Complementarily, since NSCLC is the most common lung cancer subtype in never-smokers, it is understandable that clinical trials conducted to date have primarily focused on this histology. However, building on the improved molecular and genetic characterization efforts discussed above, it would be of interest to investigate the occurrence of SCLC in never-smokers and to explore therapeutic strategies specifically directed at this subtype.
Furthermore, in silico and computational approaches are excellent tools to improve our understanding of LC in never-smokers and to predict therapy responses. Some studies have already developed risk prediction models specifically for this population. Those are crucial to access personalized risk assessment for lung cancer, helping identify high-risk never-smoking patients and helping in the formulation of future LC screening strategies, where the inclusion of this population is vital [37]. Nevertheless, it remains important to continue research in this area to refine predictions and integrate them with molecular and therapeutic data. Moreover, in silico research focused on never-smoker LC patients remains more centred on these computational risk prediction models. Consequently, other advanced studies such as therapy response modelling, virtual trials, or even digital twin approaches are still largely unexplored in this population.
Considering the heterogeneity of lung cancer and the distinct molecular signatures in never-smokers, digital twin technology may serve as a dynamic integrative platform to simulate tumour evolution, optimize therapy, and advance precision oncology. Digital twin technology is an emerging computational approach that enables the simulation of disease progression and treatment responses through the integration of multi-level patient data. In oncology, this field is still in early development but shows potential for supporting clinical decision-making, optimizing therapeutic strategies, and guiding the design of future clinical trials. However, several challenges remain, including data heterogeneity, technical complexity, computational requirements, and ethical considerations [38,39]. Nevertheless, as the molecular and clinical characterization of lung cancer in never-smokers continues to improve, digital twin-based approaches may in the future offer a complementary framework to explore disease behaviour and personalized therapeutic strategies in this patient population.
4. Conclusions
Lung cancer remains the most prevalent and deadliest cancer worldwide. Over recent years, the epidemiological profile of this disease has been changing, with a growing proportion of cases occurring in never-smokers. This trend partly reflects the global decline in tobacco consumption but also indicates the increasing contribution of other risk factors such as air pollution (e.g., long-term exposure to PM_2.5_), occupational exposures, and genetic susceptibility. Non-small-cell lung cancer (NSCLC) is the predominant type among never-smokers, whose tumours often display distinctive genetic and molecular features. Consequently, the design of therapeutic regimens tailored to these molecular characteristics is of paramount importance. Never-smoker lung cancer frequently harbours oncogenic drivers (e.g., EGFR, ALK, ROS1, RET, MET). It exhibits a distinct immune–genomic milieu compared with tobacco-associated disease, with implications for both targeted therapies and immunotherapy. These features underscore the need for comprehensive molecular profiling at diagnosis, including broad next-generation sequencing panels, optimizing therapeutic matching, and avoiding under-treatment. In parallel, improved phenotyping of environmental exposures, particularly fine particulate matter and indoor/occupational toxicants, should be integrated into clinical datasets to clarify exposure–genotype–phenotype relationships and refine risk stratification [40,41,42].
Although some clinical trials have specifically addressed never-smoker patients, most remain limited in scope and focus mainly on classical targets such as EGFR and angiogenesis. Future studies should adopt biomarker-enriched umbrella/basket designs, adaptive randomization, and pragmatic endpoints that reflect real-world effectiveness. Harmonized definitions of “never-smoker”, standardized exposure assessment, and better representation of women and diverse geographic regions will also be critical to improve external validity and equity of evidence. Given the rising incidence and mortality within this group, there is an urgent need to reinvigorate research efforts through the integration of multi-omics approaches (genomics, transcriptomics, proteomics, and metabolomics), interinstitutional collaboration, and in silico methods. Mechanistic and data-driven models can accelerate target discovery, drug repurposing, and dose optimization, while federated analytics may enable privacy-preserving learning across institutions. In parallel, investment in digital twin technologies, namely virtual, continuously updated patient models that couple tumour biology, pharmacology, and clinical trajectories, represents a promising and underexplored strategy to forecast response, personalize sequencing of therapies, and improve outcomes for never-smoker lung cancer patients.
Finally, a comprehensive agenda should align prevention and therapy, including strengthening air quality regulations and workplace safety, deploying early-detection strategies tailored to never-smokers with high non-tobacco exposure burden, and embedding longitudinal exposure metrics into clinical care. Such an integrated framework, linking exposure mitigation, precision diagnostics, and adaptive therapeutics, will be essential to bend the mortality curve for never-smoker lung cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferlay J.E.M. Lam F. Laversanne M. Colombet M. Mery L. Piñeros M. Znaor A. Soerjomataram I. Bray F. Global Cancer Observatory: Cancer Today International Agency for Research on Cancer Lyon, France 2024 Available online: https://gco.iarc.who.int/today(accessed on 8 January 2026)
- 2Ruano-Raviña A. Provencio M. Calvo de Juan V. Carcereny E. Moran T. Rodriguez-Abreu D. López-Castro R. Cuadrado Albite E. Guirado M. Gómez González L. Lung cancer symptoms at diagnosis: Results of a nationwide registry study ESMO Open 20205 e 00102110.1136/esmoopen-2020-00102133214227 PMC 7678343 · doi ↗ · pubmed ↗
- 3Schabath M.B. Cote M.L. Cancer Progress and Priorities: Lung Cancer Cancer Epidemiol. Biomark. Prev.2019281563157910.1158/1055-9965.EPI-19-0221 PMC 677785931575553 · doi ↗ · pubmed ↗
- 4Zito Marino F. Bianco R. Accardo M. Ronchi A. Cozzolino I. Morgillo F. Rossi G. Franco R. Molecular heterogeneity in lung cancer: From mechanisms of origin to clinical implications Int. J. Med. Sci.20191698198910.7150/ijms.3473931341411 PMC 6643125 · doi ↗ · pubmed ↗
- 5Nooreldeen R. Bach H. Current and Future Development in Lung Cancer Diagnosis Int. J. Mol. Sci.202122866110.3390/ijms 2216866134445366 PMC 8395394 · doi ↗ · pubmed ↗
- 6Thai A.A. Solomon B.J. Sequist L.V. Gainor J.F. Heist R.S. Lung cancer Lancet 202139853555410.1016/S 0140-6736(21)00312-334273294 · doi ↗ · pubmed ↗
- 7Ramos R. Moura C.S. Costa M. Lamas N.J. Correia R. Garcez D. Pereira J.M. Lindahl T. Sousa C. Vale N. Lung Cancer Therapy: The Role of Personalized Medicine Cancers 20251772510.3390/cancers 1705072540075573 PMC 11899562 · doi ↗ · pubmed ↗
- 8Ramos R. Moura C.S. Costa M. Lamas N.J. Correia R. Garcez D. Pereira J.M. Sousa C. Vale N. Enhancing Lung Cancer Care in Portugal: Bridging Gaps for Improved Patient Outcomes J. Pers. Med.20241444610.3390/jpm 1405044638793028 PMC 11121920 · doi ↗ · pubmed ↗