Maternal Stress, Depression, Anxiety, and Participation in Care in Neonatal Semi-Intensive and Intensive Care Units: Results of a Cross-Sectional Study in Two Sri Lankan Hospitals
Nimesha Gamhewage, Mohamed Rishard, Nalin Gamaathige, Loshika Janet, Ilaria Mariani, Hemantha Senanayake, Marzia Lazzerini

TL;DR
Mothers of infants in neonatal units in Sri Lanka experience high stress, depression, and anxiety, and are often not involved in their care.
Contribution
This study provides insights into maternal psychological burden and care participation in neonatal units in a resource-limited setting.
Findings
94.3% of mothers experienced at least one psychological condition, and 59% experienced all three.
Only 13% of mothers achieved a high level of participation in neonatal care.
Higher maternal participation was associated with reduced stress and anxiety.
Abstract
What are the main findings? We observed high psychological morbidity and limited maternal participation in newborn care among mothers of infants admitted to neonatal units.Anxiety and stress levels were higher among mothers who were less involved in the care of their neonates. We observed high psychological morbidity and limited maternal participation in newborn care among mothers of infants admitted to neonatal units. Anxiety and stress levels were higher among mothers who were less involved in the care of their neonates. What are the implications of the main findings? Mothers should be encouraged to actively participate in the care of their newborns during neonatal unit admission.In Sri Lankan settings, routine screening for maternal psychological burden, along with policy reforms, is recommended. Mothers should be encouraged to actively participate in the care of their newborns…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
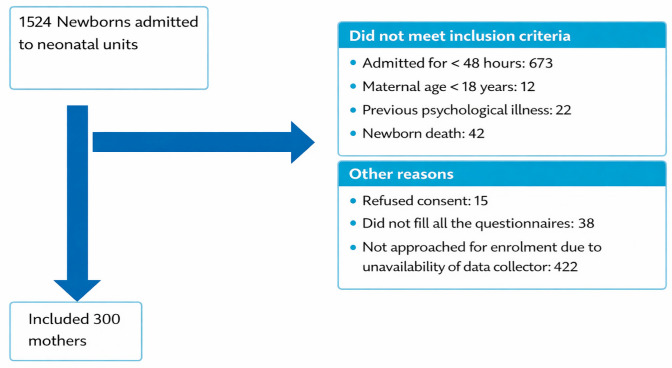 Figure 1
Figure 1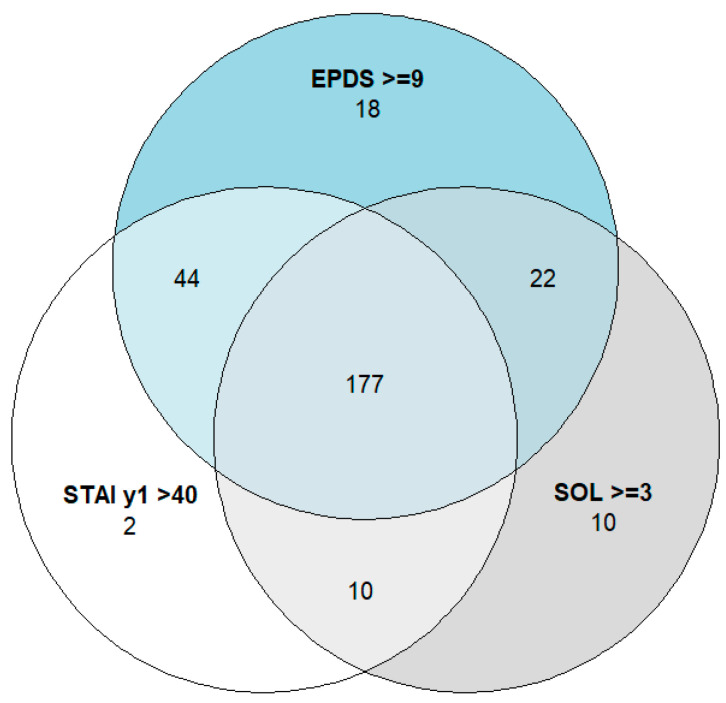 Figure 2
Figure 2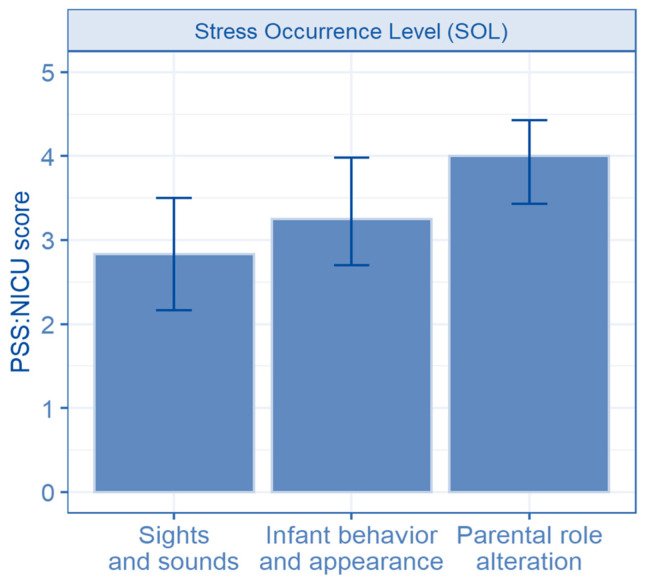 Figure 3
Figure 3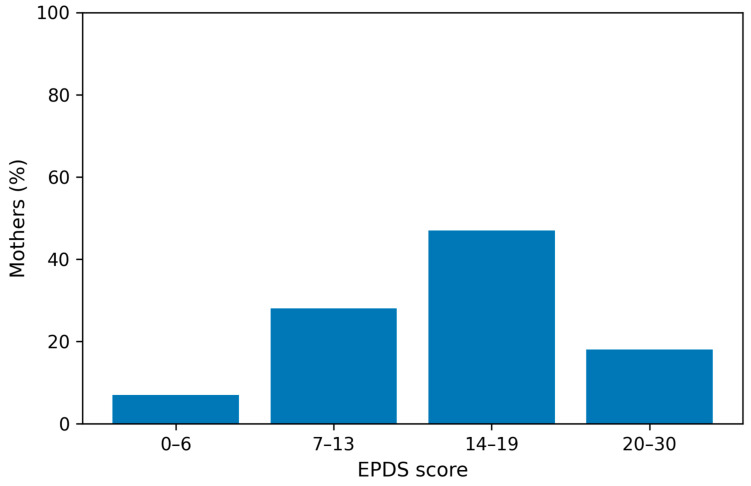 Figure 4
Figure 4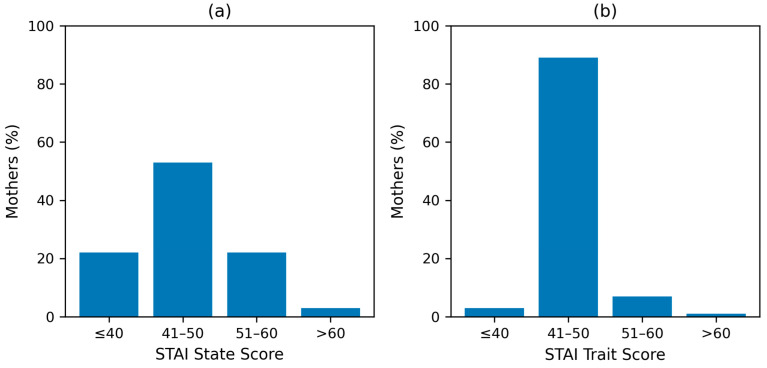 Figure 5
Figure 5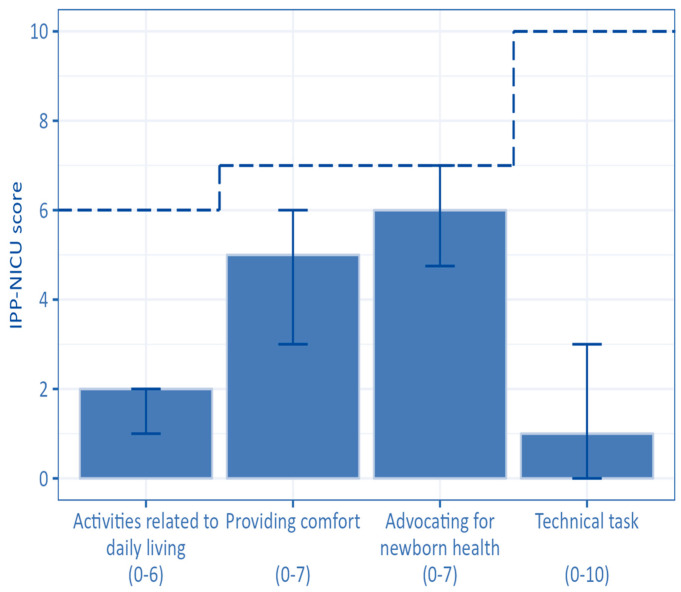 Figure 6
Figure 6- —Italian Ministry of Health
- —Institute for Maternal and Child Health, IRCCS Burlo Garofolo, Trieste, Italy
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Development and Preterm Care · Neonatal Respiratory Health Research · Family and Patient Care in Intensive Care Units
1. Introduction
Globally, up to 30 million neonates require inpatient care annually [1]. The reasons include prematurity, hypoxic ischaemic encephalopathy, neonatal sepsis, jaundice, and congenital anomalies [1]. The neonatal intensive care unit (NICU) environment is stressful for neonates, leading to detrimental effects on their health and development [2].
In recent years, there has been a growing recognition of the burden of parental stress, depression, and anxiety when a newborn is admitted to the NICU [3,4]. However, data from resource-poor settings are scarce. In a single-centre study conducted in a Sri Lankan NICU, 44% and 32% of mothers reported having severe and extreme levels of stress, respectively [5]. The primary causes of stress were changes in the parental role, the physical environment of the NICU, the severity of the baby’s illness, past neonatal fatalities, and having a previous baby who required NICU admission [5]. No data are available regarding the rates of depression and anxiety of mothers with a neonate admitted to the NICU in Sri Lanka.
Maternal stress, anxiety, and depression can lead to lasting psychological effects, necessitating support and intervention [6,7,8]. These negative experiences could adversely affect the developmental outcomes of infants. In addition, they lead to behavioural issues and affect parent-infant relationships and parental roles [7,9]. To mitigate these detrimental effects, interventions such as family-centred care and parental involvement in the care of newborns in the NICU are recommended [10,11]. However, awareness that parents can play a greater role in the care of their neonates in NICUs in resource-limited settings seems to be limited.
Sri Lanka has achieved remarkable gains in neonatal care over the past several decades. The neonatal mortality rate in 2023 was 7.2 per 1000 live births [12], which compares well with countries with a higher per capita income [13]. Despite these accomplishments, the psychological aspects have been neglected, and only a few studies have been conducted to evaluate parental psychological health [5], with none related to parental participation in their newborn’s care. In Sri Lankan NICU settings, the care is focused almost entirely on the outcomes of the neonates. Mothers are permitted to visit their infants only during designated times, and their involvement in neonatal care is largely limited to providing expressed breast milk and participating in kangaroo mother care.
This study was the Sri Lankan component of a multicentre international cross-sectional quality improvement project titled “Empowering parents in the NICU” (EPiNICU), which aimed to collect data and to develop and test evidence-based models of interventions to improve parental participation, mental health, and well-being of parents of newborns admitted to the NICU. This study was conducted to assess the prevalence and severity of NICU-related maternal stress, depression, and anxiety. We also assessed the level of maternal involvement in the newborn’s care while the baby was managed in the neonatal unit. Additionally, the study assessed risk factors associated with maternal psychological morbidity.
2. Materials and Methods
2.1. Study Design and Setting
Given the absence of prior data from Sri Lankan NICUs on these psychosocial outcomes, an observational cross-sectional design was necessary to characterise the local context. Therefore, this study was conducted in two tertiary care hospitals in Colombo, Sri Lanka, namely, the De Soysa Hospital for Women and the Colombo South Teaching Hospital. The two hospitals have a total of 10,000 deliveries per year and 1800 admissions to the neonatal units. The two units have 22 NICU beds and 20 semi-intensive care spaces. During the study period, 72 nurses, 27 doctors, and 4 neonatologists were in service in the two facilities. Both hospitals accept in utero transfers of complicated pregnancies and neonatal transfers. Results are reported according to the STROBE guidelines [14] (Supplemental Table S1). The study design was aligned with the EPINICU multicentre protocol to allow meaningful comparison across diverse healthcare settings.
2.2. Study Participants
Mothers having a neonate needing intensive care or semi-intensive care for more than 48 h at the study sites were eligible for inclusion. Mothers who were under 18 years of age, those with existing mental illness that precluded them from providing informed consent, and those facing the impending death of their baby were excluded.
A trained multilingual data collector approached the mothers close to the date of discharge from the neonatal unit and obtained informed written consent before recruitment. A convenience sampling method was followed based on the availability and willingness to participate of mothers. The data collector used the NICU and semi-intensive care unit registry. Mothers were approached in the waiting area of the neonatal unit, where they generally remain until accompanied by a staff member to the postnatal wards.
2.3. Data Collection Tools
2.3.1. Parental Stressor Scale: NICU
The reduced version of the Parental Stressor Scale (PSS:NICU), a scale specific to measuring parental stress related to the NICU, was utilised to measure stress [15]. PSS:NICU has been used previously in Sri Lanka [5]. The scale is composed of 26 statements categorised into three domains: stress resulting from “sights and sounds”, “infant behaviour and appearance”, and “parental role alteration”. Questions in the PSS:NICU do not refer to a specific period of time. Stress is scored on a five-point Likert scale, with one point assigned for “not at all stressed” and five points assigned for “severe stress”. The total PSS:NICU scores are determined in two ways: the stress occurrence level (SOL) and the overall stress level (OSL). SOL is computed using only experienced items, and OSL with one point deducted for “not applicable” items. In this study, we determined only the SOL score, as it is suggested to use the OSL when the focus is on the NICU environment and the SOL when the focus is on the parent [15]. A cut-off of three or more has been used in the literature to identify those affected by stress [16].
2.3.2. Edinburgh Postnatal Depression Scale
The Edinburgh Postnatal Depression Scale (EPDS), which has been validated in Sri Lanka, was utilised to assess the presence of symptoms of depression [17]. There are ten items on the scale, each with four answers, with scores ranging from 0 to 3. According to the total score obtained, the severity of symptoms is categorised as none or minimal depression (0–6), mild depression (7–13), moderate depression (14–19), and severe depression (20–30) [18]. Validated versions of this tool are available both in Sinhala and Tamil. The Sri Lankan study that validated the EPDS suggested a cut-off score of 9 for screening for depression in our settings [17].
2.3.3. State–Trait Anxiety Inventory
Anxiety was evaluated by the State–Trait Anxiety Inventory (STAI), which is composed of two scales: state anxiety (Y1), i.e., how one feels at the moment, and trait anxiety (Y2), i.e., how one generally feels [19]. Each STAI scale contains 40 items with a four-point Likert scale (from 0 to 3 points). The questionnaire is not specific to parents’ anxiety in the NICU [20]. The presence of anxiety was identified with a score above 40. Mild, moderate, and severe anxiety are indicated by scores between 41 and 50, 51–60, and >60, respectively [20,21]. STAI has been previously validated and used in Sri Lanka [22]. We utilised state anxiety scores to describe maternal anxiety.
2.3.4. Index of Parental Participation
Participation in care was assessed via the Index of Parental Participation (IPP-NICU) questionnaire. This was originally used on parents whose children were admitted to the hospital [23]. We used an adapted version of it to reflect activities related to newborn care. This adapted version has been successfully used in similar low-resource settings [24]. The IPP-NICU assesses parental involvement during the previous 24 h in four domains: activities related to daily living (6 items), providing comfort (7 items), advocating for newborn health (7 items), and technical tasks (10 items). There are no recommendations in the literature regarding the cut-off score of the IPP-NICU, but we used a cut-off of 20 in accordance with previous studies [16]. The maximum score is 30.
The study instruments, other than the EPDS and STAI, were translated and back-translated to Sinhala and Tamil, the two main languages spoken in the country, by two qualified translators to ensure accuracy and consistency.
Details of the baby (gestational age at birth, birth weight, APGAR score, complications during the hospital stay, need for intubation, surgical interventions, and length of stay) were collected from the patient records. Details regarding the mothers’ socioeconomic background and educational status were obtained directly from the interview with the mothers.
2.4. Data Collection Procedure
The eligible mothers were approached by a trained research assistant who was not involved in patient management or data analysis and was fluent in all three languages used in the country: Sinhala, Tamil, and English. All questionnaires were self-administered, and hard copies were provided to the participants. Data were collected from November 2023 to September 2024 at both sites. In January 2024 and May 2024, the data collector was not available. Therefore, mothers were not approached for enrolment in those months.
2.5. Study Outcomes and Sample Size Calculation
Prevalence of maternal NICU-related stress evaluated with SOL was predefined as the primary study outcome. Other key outcomes were the prevalence of maternal depression, maternal state and trait anxiety, and maternal participation in newborn care.
A sample of 271 mothers was required based on the reported prevalence of stress in parents of newborns in neonatal units of 50 ± 10% [16], with a confidence level of 99.9%.
2.6. Data Analysis
Descriptive statistics were used to describe the characteristics of neonates and mothers, to summarise the scores of depression, stress, anxiety, and parental participation in care, and to determine the prevalence of the above psychological conditions.
Univariate and multivariate logistic regression models were conducted for each mental health condition under analysis (i.e., depression, stress, and anxiety) considering the following variables as explanatory variables: maternal participation in care (dichotomised as IPP-NICU ≥ 20 or below), maternal socioeconomic background (ethnicity, maternal age, and maternal occupation), and newborn characteristics (APGAR at 5 min, the birth weight of the neonate, gestational age, need for ventilation, admission to NICU/semi-intensive care, presence of respiratory distress, sepsis, and total duration of hospital stay). For twin pregnancies in which both infants required admission, only the characteristics of the first twin were collected and included in the analysis.
Dependent variables were analysed as binary variables using the following cut-offs: SOL ≥ 3, EPDS ≥ 9, and STAI Y1 > 40. Odds ratios (ORs) and adjusted odds ratios (aORs) were calculated, with 95% confidence intervals (CIs) and p values of significance.
All statistical tests were two-tailed. Statistical analyses were performed using Stata V.14 and R V.4.1.1. A p-value less than 0.05 was considered statistically significant.
3. Results
Among the 1524 neonates admitted to neonatal units at the study sites during the study period, 775 were eligible. Very few mothers refused participation (n = 15). Overall, we included 300 neonates and 300 mothers (Figure 1).
The characteristics of the mothers are summarised in Table 1. The median age of mothers was 30 years (IQR 26–34, mean 30, SD 6). All mothers were married, and most belonged to the Sinhala ethnic group (n = 199, 66.3%). All had received either secondary or higher education.
The characteristics of the neonates are summarised in Table 2. The median birth weight was 2335 g (IQR 1430–2990, mean 2238.2, SD 885.7). Approximately a quarter of newborns were born less than 32 completed weeks of gestation, and 27.6% (n = 83) weighed less than 1500 g. The majority were admitted to the NICU (78.3%).
3.1. Overall Prevalence of Stress, Depression, and Anxiety
A total of 283 (94.3%) mothers were detected as experiencing at least one condition, whereas 177 (59.0%) experienced all three conditions together (Figure 2). In the study sample of 300 mothers, only 16 reported no condition. The PSS:NICU score was not collected for one mother.
3.2. Prevalence of Stress, Depression, and Anxiety
3.2.1. Maternal Stress
A total of 219 mothers (73%) scored 3 or more on the PSS:NICU SOL score, indicating the presence of stress. The mean PSS:NICU SOL score was 3.34 (Table 3). The highest mean subscore was noted in the parental role alteration domain (mean 3.81, SD 0.89; median 4, IQR 3.43–4.43) (Figure 3, Supplemental Table S2).
3.2.2. Maternal Depression
A total of 261 mothers (87%) scored 9 or more in the EPDS score (Figure 2). The median EPDS score for the study population was 15 (IQR 11–18, mean 14.76, SD 5.4) (Table 3). In total, 140 mothers (46.7%) scored 14–19 (moderate symptoms), while 53 mothers (17.6%) scored 20–30 (severe symptoms) in the EPDS score (Supplemental Table S3). Figure 4 illustrates the severity categories of depression.
3.2.3. Maternal Anxiety
The mean STAI state score was 45.52 (SD 8.42; median score 46, IQR 41.50–50.50), and 77.7% of mothers (n = 233) had scores above 40 (Table 3, Figure 2). The majority of mothers (n = 158, 52.7%) had mild anxiety symptoms (Supplemental Table S3).
Trait anxiety was present in 96.7% (n = 290) of mothers (mean score 45.79, SD 3.23; median 47, IQR 45–48) (Table 3). The majority of mothers (n = 268, 89.3%) had mild levels of trait anxiety (Supplemental Table S3).
Figure 5 illustrates the severity categories of maternal state and trait anxiety.
3.3. Maternal Participation in Care of the Neonate
The mean IPP-NICU score was 13.81 (SD 4.95; median score 13, IQR 11.00–16.50) (Table 3). Only 13.0% of mothers (n = 39) had IPP-NICU scores ≥ 20. The domain with the lowest median value was the “technical tasks” domain (mean 2.03; SD 2.72; median score 1, IQR 0–3). The median scores and the IQR of the IPP-NICU are shown in Figure 6 (Supplemental Table S4).
3.4. Logistic Regressions
3.4.1. Stress
Univariate analysis revealed a statistically significant association between lower rates of stress in Tamil mothers compared to Sinhalese mothers (OR 0.37, 95% CI 0.19–0.73, p = 0.004), and mothers with IPP-NICU scores ≥ 20 (OR 0.25, 95% CI 0.12–0.50, p < 0.001). Multivariate analysis confirmed results for mothers with IPP-NICU scores ≥ 20 (aOR 0.27, 95% CI 0.12–0.59, p = 0.001) (Table 4).
3.4.2. Depression
In univariate analysis, we found EPDS scores ≥ 9 more frequently in mothers with babies born at 32–37 weeks of gestation, compared with the group <27 weeks of gestation (OR 5.44, 95% CI 1.01–25.29, p = 0.034), and less frequently in babies admitted to the semi-intensive care unit compared to NICU admission (OR 0.43, 95% CI 0.21–0.91, p = 0.023). The multivariate analysis confirmed that the odds of depression were lower in mothers with babies admitted to a semi-intensive unit compared to the NICU (aOR 0.29, 95% CI 0.12–0.68, p = 0.004) (Table 5).
3.4.3. Anxiety
Univariate analysis revealed that mothers with IPP-NICU scores ≥ 20 (OR 0.4, 95% CI 0.20–0.83, p = 0.011) and both Tamil and Muslim mothers compared to Sinhala mothers (Tamil: OR 0.35, 95% CI 0.17–0.72, p = 0.004; Muslim: OR 0.43, 95% CI 0.22–0.85, p = 0.014) had lower chances of having STAI state anxiety scores > 40. The multivariate analysis confirmed these results (Tamil: aOR 0.27, 95% CI 0.12–0.63, p = 0.002; Muslim: aOR 0.34, 95% CI 0.16–0.73, p = 0.005; IPP-NICU scores ≥ 20: aOR 0.32, 95% CI 0.14–0.72, p = 0.005) (Table 6).
4. Discussion
This is the first comprehensive study from a South Asian setting to report maternal psychological morbidity when a baby is admitted to neonatal units. The findings are generally in concordance with other settings, but we found the prevalence of stress, anxiety, and symptoms of depression to be much higher in our study [3,24,25].
Symptoms of depression were found in 87.0% of the study participants. Other studies have reported a prevalence of 18.0% and 52.0% [3]. A multicentre study involving Italy, Brazil, and Tanzania reported prevalences of 33.3%, 35.8%, and 52.3%, respectively [24]. A community-based study conducted in two Medical Officer of Health areas in Sri Lanka revealed a prevalence of 15.5% on the 10th postpartum day and 7.8% at 4 weeks postpartum [26].
Compared with mothers whose babies required admission to the semi-intensive care unit, those whose babies were admitted to the NICU had a significantly greater prevalence of depressive symptoms. This indicates a need for routine screening of mothers for depression when babies require admission to the NICU. This finding aligns with recommendations for the routine screening of mood and anxiety disorders by many authorities [27,28]. As in several other settings, we could not observe a significant association between maternal sociodemographic characteristics, complications of the infant, or the total duration of hospital stay [24,25]. However, prematurity has been identified in the literature as a potential risk factor for postpartum depression [29]. In our study, the lack of an observed association in multivariate regression between prematurity and maternal depression may be attributable to the small sample size of mothers without depressive symptoms. Notably, the EPDS is only a screening tool, and confirmation of the diagnosis requires clinical input [30].
Similar to a previous study conducted in Sri Lanka regarding maternal stress [5], our study revealed a high prevalence of stress (74%). Furthermore, the observed prevalence was higher than that reported from other EPiNICU project facilities, where rates ranged from 4.5% in Tanzania to 64.5% in Brazil and 36.7% in Italy [24]. The domain with the highest levels of stress was the alteration in the parental role, similar to the findings of previous studies [16,24]. Mothers often feel unprepared for discharge due to limited engagement with their neonates, which can lead to emotional strain and increased risk of readmission [31]. This is further supported by the association of a higher incidence of stress in mothers who were less involved in their baby’s care (IPP-NICU scores less than 20). These factors highlight the need to guide and encourage mothers to play a greater role in their baby’s care. Variables such as maternal age, duration of stay in the NICU, the presence of neonatal seizures, and the need for ventilator support have been described as factors associated with increased stress [32]. However, in our study, no association was observed between these factors and maternal stress, indicating that the determinants of maternal stress may differ across settings.
We found a higher prevalence of state anxiety (77.7%) than in other facilities participating in the EPiNICU project (36.9% in Italy and 59.3% in Brazil) [24]. Sinhalese mothers were more likely to report state anxiety than the other two ethnic groups. Anxiety related to ethnicity has been reported in previous studies as well [24]. This may be an aspect that is worthy of further study. The associations between low IPP-NICU scores and anxiety and stress are significant findings that have not been demonstrated in other countries [24].
The score for participation in care was lower in our study population than in other studies. Using the same instrument, parents in Tanzania, Italy, and Brazil scored median IPP-NICU scores of 24 (IQR 21; 26), 18 (IQR 12; 22), and 21 (IQR 15; 24.8), respectively [24]. Similar to our observations, no country reached the highest possible level of parental participation in care. Furthermore, the largest gap across all countries was found in the “Technical tasks” domain [24]. In Sri Lankan NICUs, maternal involvement in neonatal care is not actively encouraged. The results of our study emphasise the need for a change in the culture of Sri Lankan neonatal units, promoting structured support systems, such as family-integrated care, which promote parental involvement and empowerment in NICUs [11,33]. Participation in care is a modifiable factor that could be achieved with changes in NICU policies and could influence maternal stress and anxiety levels.
Beyond the risk factors assessed in this study, maternal chronic illnesses, particularly those affecting fertility such as endometriosis, can contribute to a significant mental health burden, which may be present even before conception and persist after delivery [34,35].
We acknowledge the following limitations of our study. First, as it is a cross-sectional study, causal inference among different study variables cannot be assessed. However, it highlights a problem that is often overlooked in NICU settings. Second, except for EPDS and STAI, other study instruments have not been validated in Sri Lanka. Nevertheless, these questionnaires have been widely used in different contexts, including LMICs. Furthermore, the findings of this study cannot be generalised to the whole country, as we conducted the study in two urban tertiary care hospitals. However, we were able to include study participants from various socioeconomic, educational, and ethnic backgrounds. In addition, exclusion of mothers younger than 18 years, who are considered a vulnerable population requiring additional ethical safeguards, may limit the generalisability of the findings to adolescent mothers with neonates admitted to the NICU. Finally, these findings indicate the need for further studies in similar settings and also to study the psychological burden of fathers.
5. Conclusions
Our study demonstrates an exceptionally high prevalence of depressive symptoms, anxiety, and stress among mothers of neonates admitted to Sri Lankan NICUs, which is a significant, previously under-recognised entity. The strong association between low maternal participation in neonatal care and increased psychological distress highlights the importance of supporting maternal involvement in the newborns’ care during NICU admissions. These findings provide context-specific evidence to inform improvements in neonatal care practices and policy development in Sri Lanka, in accordance with the objectives of the EPiNICU project, which aimed at identifying and developing context-specific interventions to empower parents in NICUs.
Routine screening for maternal psychological conditions using validated tools, such as the EPDS, should be integrated into standard NICU care to enable early identification and timely intervention. Collaboration with mental health services within NICUs should be promoted. Introducing FCC models to Sri Lankan NICUs may help reduce maternal psychological distress and empower parents. Culturally sensitive psychosocial support is essential, given the observed ethnic differences in anxiety levels.
Beyond the clinical setting, admission to a NICU should be recognised as a significant risk factor for maternal mental health problems. Mothers with hospitalised neonates should be included as a high-risk group in public health programmes. Early identification and support during the immediate postnatal period, alongside staff training in recognising maternal distress and implementing family-centred care, have the potential to improve maternal well-being, mother–infant bonding, and long-term child developmental outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organisation Survive and Thrive: Transforming Care for Every Small and Sick Newborn in 2019 Available online: https://apps.who.int/iris/bitstream/handle/10665/326495/9789241515887-eng.pdf(accessed on 10 February 2025)
- 2Van Dokkum N.H. de Kroon M.L. Reijneveld S.A. Bos A.F. Neonatal stress, health, and development in preterms: A systematic review Pediatrics 2021148 e 202105041410.1542/peds.2021-05041434548378 · doi ↗ · pubmed ↗
- 3Shetty A.P. Halemani K. Issac A. Thimmappa L. Dhiraaj S. Mishra P. Upadhyaya V.D. Prevalence of anxiety, depression, and stress among parents of neonates admitted to neonatal intensive care unit: A systematic review and meta-analysis Clin. Exp. Pediatr.20246710410.3345/cep.2023.0048637986569 PMC 10839189 · doi ↗ · pubmed ↗
- 4Malouf R. Harrison S. Pilkington V. Opondo C. Gale C. Stein A. Franck L.S. Alderdice F. Factors associated with posttraumatic stress and anxiety among the parents of babies admitted to neonatal care: A systematic review BMC Pregnancy Childbirth 20242435210.1186/s 12884-024-06383-538724899 PMC 11084127 · doi ↗ · pubmed ↗
- 5Nirubaa U. Sathiadas M.G. Maternal stress level when a baby is admitted to the neonatal intensive care unit at Teaching Hospital Jaffna, and the influence of maternal and infant characteristics on this level Sri Lanka J. Child Health 201645909410.4038/SLJCH.V 45I 2.8003 · doi ↗
- 6Chiha K. Khemakhem K. Regaieg C. Touhemi D.B. Ayadi H. Hmida N. Gargouri A. Moalla Y. Maternal stress and postnatal hospitalisation of the baby Eur. Psychiatr.202366 S 722S 72310.1192/j.eurpsy.2023.1514 · doi ↗
- 7Saharoy R. Potdukhe A. Wanjari M. Taksande A.B. Postpartum depression and maternal care: Exploring the complex effects on mothers and infants Cureus 202315 e 4138110.7759/cureus.4138137546054 PMC 10400812 · doi ↗ · pubmed ↗
- 8SalomèS. Mansi G. Lambiase C.V. Barone M. Piro V. Pesce M. Sarnelli G. Raimondi F. Capasso L. Impact of psychological distress and psychophysical wellbeing on posttraumatic symptoms in parents of preterm infants after NICU discharge Ital. J. Pediatr.2022481310.1186/s 13052-022-01202-z 35073953 PMC 8785440 · doi ↗ · pubmed ↗