Autologous Stem Cell Transplantation in HIV-Positive and HIV-Negative Patients with Lymphoma: A Propensity Score-Matched Comparative Analysis
Alessandro Re, Margherita Oberti, Armando Stabile, Angelo Andreini, Chiara Cattaneo, Chiara Pagani, Salvatore Casari, Maria Antonia Forleo, Cristina Tecchio, Camillo Almici, Alessandra Tucci, Francesco Castelli, Giuseppe Rossi, Mauro Krampera

TL;DR
This study shows that autologous stem cell transplantation is more effective for HIV-positive lymphoma patients compared to HIV-negative patients, with better survival and lower relapse rates.
Contribution
The study is the first to demonstrate better progression-free survival and lower relapse rates in HIV-positive patients after stem cell transplantation compared to HIV-negative patients.
Findings
HIV-positive patients had significantly higher 4-year progression-free survival (81%) compared to HIV-negative patients (51%).
Relapse rates were significantly lower in HIV-positive patients (23%) compared to HIV-negative patients (36%).
Four-year overall survival was 81% in HIV-positive and 67% in HIV-negative patients, though not statistically significant.
Abstract
Treatment of HIV-associated lymphoma (HIV-Ly) with autologous stem cell transplantation (ASCT) has shown to be feasible and effective. In this study we compare the clinical outcomes of HIV-Ly and lymphomas of the general population receiving ASCT, analyzing two series of consecutive HIV-positive and HIV-negative patients, based on a 1:1 propensity score match analysis. Forty-four patients were identified in both groups. Progression-free survival (PFS), defined as the time from ASCT to relapse, progression or death for any cause, was significantly higher in HIV-positive patients (4-year PFS 81% and 51%, in HIV-positive and HIV-negative patients, respectively, p = 0.027). The 4-year OS was 81% in HIV-positive and 67% in HIV-negative patients (p = 0.15). The relapse rate was significantly higher in HIV-negative patients (36% vs. 23%) (p = 0.04). Our results increase the awareness of ASCT…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
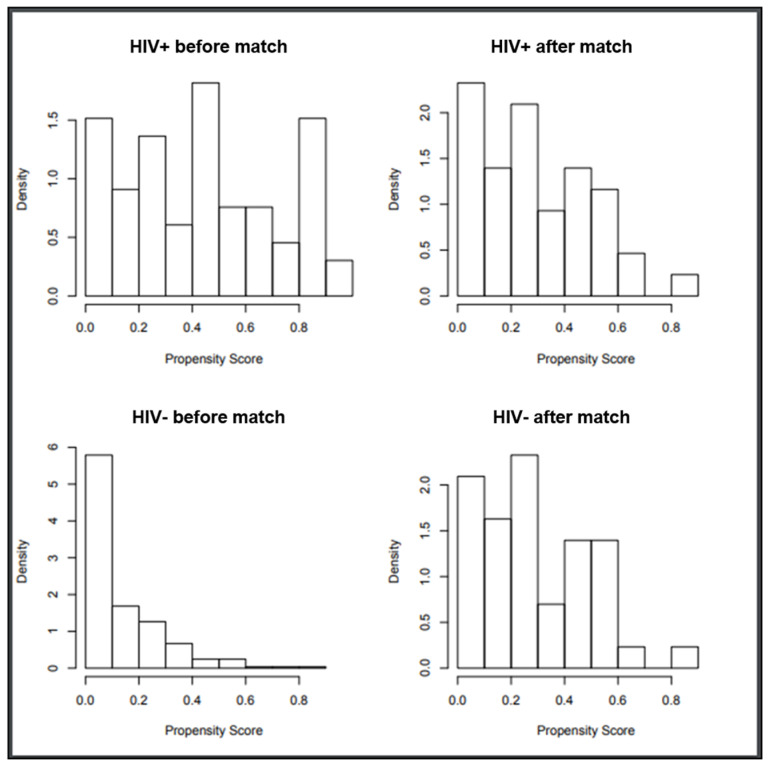 Figure 1
Figure 1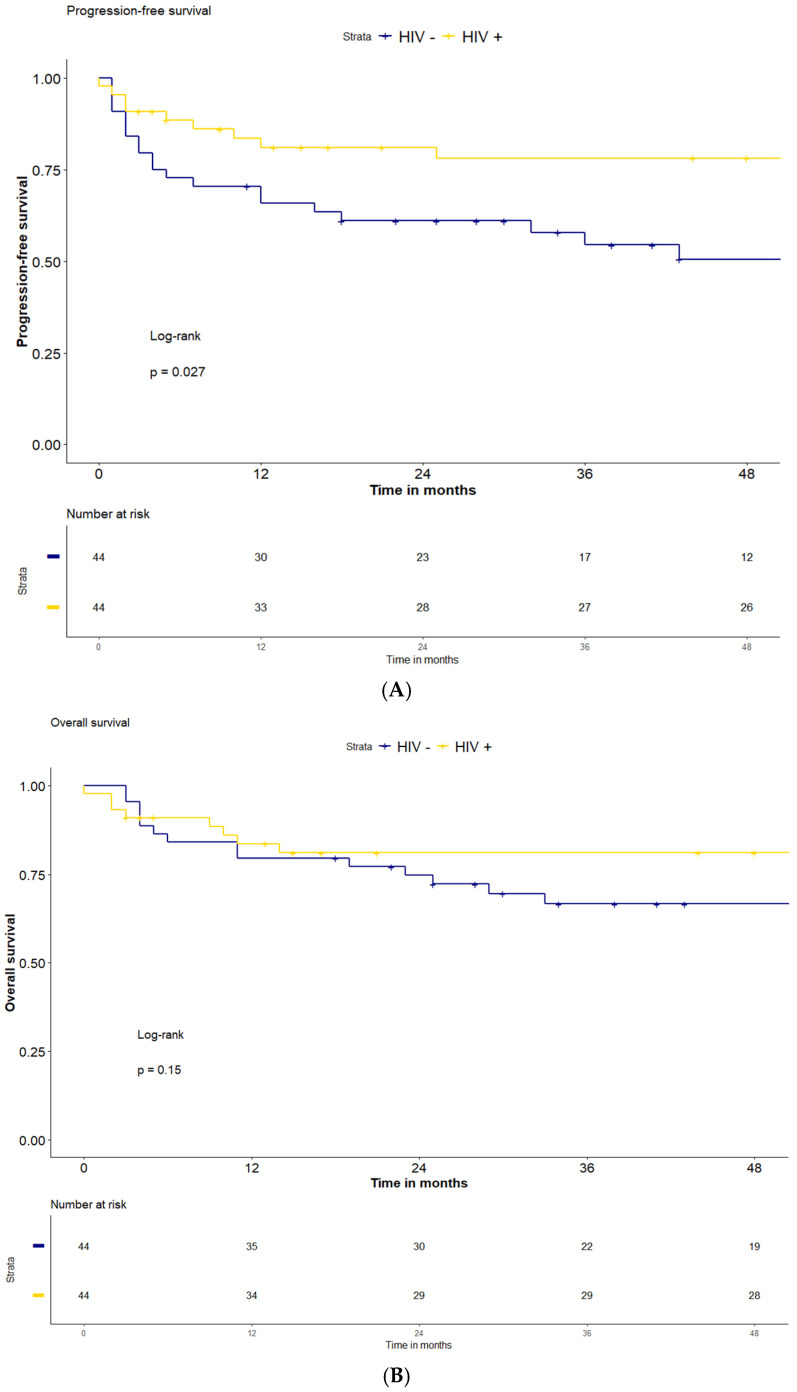 Figure 2
Figure 2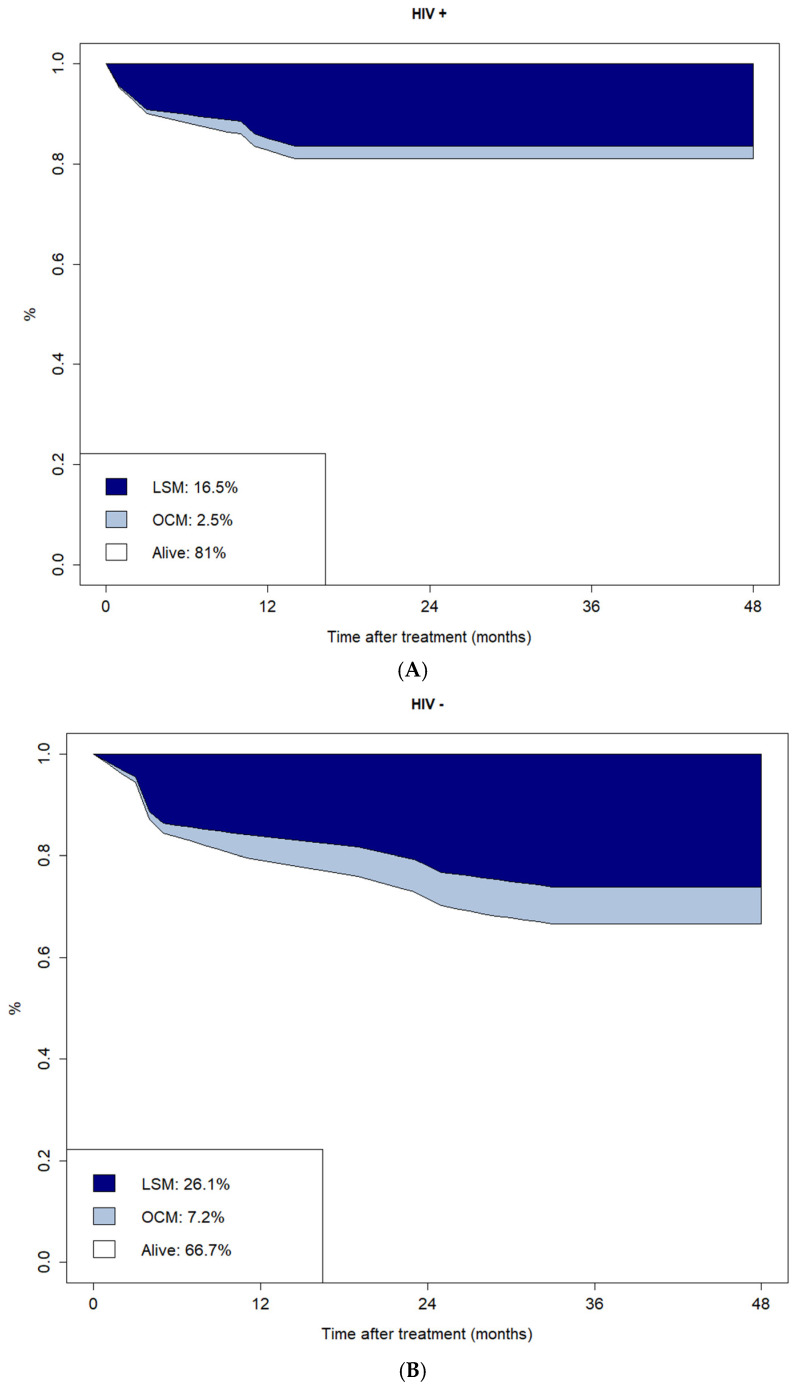 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · HIV Research and Treatment · Cytomegalovirus and herpesvirus research
1. Introduction
The global incidence of HIV-associated lymphoma (HIV-Ly) decreased consistently after the widespread use of combination antiretroviral therapy (cART). Nevertheless Hodgkin (HL) and non-Hodgkin lymphoma (NHL) remain a major cause of morbidity and mortality in people living with HIV (PLWH) [1,2]. Treatment outcomes of HIV-Ly have improved in recent decades, due to effective cART and better supportive care, making standard therapeutic regimens established for HIV-negative patients also feasible in the HIV setting. Outcomes nowadays are similar in HIV-positive and HIV-negative patients with lymphoma when treated with the same standard therapies [3]. However, several population-based studies have highlighted a major health care disparity between the HIV-positive and negative population and studies of novel cancer therapeutics still usually exclude patients with HIV infection [4,5].
The use of high-dose therapy (HDT) with autologous stem cell transplantation (ASCT) has been shown to be feasible and highly effective in HIV-Ly for several years [6,7,8,9,10]. To date ASCT is offered to HIV-positive patients with lymphoma with the same indication as for HIV-negative patients, at least in developed countries, and concerns about potentially higher infection toxicity do not limit the use of this procedure [11]. A surprisingly low relapse rate has been reported in some series of PLWH who received ASCT for HIV-Ly [7,12,13,14,15]. Some of these studies have compared the results of monocentric or multicentric cohorts of HIV-positive subjects with historical series of HIV-negative patients undergoing ASCT or with controls identified among HIV-negative groups of patients according to various matching criteria. Although the HIV-positive patients usually had a higher clinical risk, a trend in favor of a lower relapse rate and longer progression-free survival (PFS) has been reported for PLWH, although statistically not significant [11,13,14,15].
In this study, we performed a comparison between two series of consecutive HIV-positive and negative patients with lymphoma receiving HDT and ASCT at two Italian centers, based on a 1:1 propensity score match (PSM) analysis, considering the main confounding variables. The aim was to directly compare, in a statistically reliable manner, the impact of ASCT, in terms of clinical outcome and toxicity, according to patients’ HIV status.
2. Material and Methods
2.1. Study Design and Population
We compared the clinical outcome of a case series of HIV-Ly that underwent ASCT and a cohort of comparable HIV-negative patients with lymphoma who received the same treatment, using a propensity score system to appropriately match the two groups.
The HIV-positive cohort comprised 66 consecutive patients receiving HDT and ASCT at the Hematology Department of Spedali Civili di Brescia, Brescia, Italy, from January 2001 to December 2019. As the comparison group we chose two consecutive series of HIV-negative patients who underwent ASCT at the Hematology Unit of Spedali Civili di Brescia, Brescia, Italy and at the Policlinico Borgo Roma, Verona, Italy, to increase the likelihood of finding adequately matched cases. Patients who underwent the first ASCT in a tandem program of autologous–autologous or autologous–allogeneic transplantation were excluded as patients who had prior ASCT or allogeneic transplantation. Two hundred and eighty-five HIV-negative patients between 2010 and 2017 were identified.
All patient data were collected from an anonymized database previously gathered with patients’ consent, for research and publication purposes. To adjust for confounders in baseline differences between the two groups, a balance was achieved using a 1:1 PSM analysis that led to a final population of 88 patients (44 HIV-positive and 44 HIV-negative). Matching criteria included age, sex, histology, disease status at the time of transplant and number of previous therapy regimens. Disease status at ASCT was classified according to the following three categories: first complete remission (CR); chemotherapy-sensitive disease (chemo-s), which includes partial response (PR) after first-line therapy, or chemotherapy-sensitive disease (at least PR) after salvage therapy; and chemotherapy-resistant disease (chemo-r), when less than PR was achieved with the latest therapy received. Disease response was defined by the Revised Response Criteria for Malignant Lymphoma [16]. All cases were diagnosed by expert pathologists, and a histological review was deemed unnecessary.
The primary objective of this study was to compare the PFS of the two groups of HIV-positive and negative patients. Secondary objectives included evaluation of overall survival (OS), relapse rates (RR), toxicity, mortality rates, and evaluation of the causes of death. Then, the primary endpoint was PFS and secondary endpoints were OS; RR; toxicity according to the Common Terminology Criteria for Adverse Events, version 5.0 [17]; pre- and post-infectious event rates; mortality rates; lymphoma-specific mortality (LSM); and other-cause mortality (OCM) rates.
2.2. Statistics and Definition of Outcomes
Statistical analyses comprised a few steps. First, medians and interquartile ranges (IQR) or frequencies and proportions were reported for continuous or categorical variables, respectively. A Mann–Whitney U test and a Chi-square test were applied to determine the statistical significance of differences in medians and proportions, respectively. Second, propensity score match analysis was performed to achieve a comparable cohort of patients affected and not affected by HIV, respectively. Propensity scores were computed for each patient using the 1:1 nearest-neighbor approach with a caliper width of 0.1, by modeling logistic regression with the dependent variable as the presence of HIV and accounting for the following confounders: age, sex (male, female), histology, disease status at ASCT (1st CR, chemo-s, chemo-r) and the number of prior lines of therapy (1, 2, ≥3). Third, survival analyses were performed by means of Kaplan–Meier curves, using a log-rank test to compare different groups. Fourth, Cox regression analysis was performed for univariable survival analyses. For univariate analysis of prognostic factors for survival, the following parameters were considered: age, sex, histology, disease status at transplant, and number of prior lines of therapy. Finally, cumulative incidence analyses were used to plot LSM and OCM rates. PFS was defined as the time from ASCT to relapse, progression or death for any cause. OS was measured from ASCT to death for any cause, or the last time the patient was known to be alive. LSM was defined as mortality due to active lymphoma, and OCM as mortality due to any cause other than disease relapse or progression. Neutrophil engraftment was defined as the first day with an absolute neutrophil count greater than 500/μL and platelet engraftment as a self-supporting platelet count greater than 20,000/μL.
Grade > 2 toxicities were considered, according to the Common Terminology Criteria for Adverse Events, version 5.0. Infectious events were classified by post-ASCT time frames: pre-engraftment period (PRE-EP) refers to the period between HDT and hematological engraftment and post-engraftment period (POST-EP) refers to the time frame after the hematological engraftment and the first two years from ASCT. All analyses were performed using the R software v.3.6.3. All tests were two-sided with a significance level set at p < 0.05.
3. Results
3.1. Patients’ Characteristics
Following propensity score-based nearest-neighbor 1:1 matching, we identified 44 HIV-positive patients (from the initial 66) and 44 HIV-negative patients (from the initial 285) (Figure 1). Baseline patients’ characteristics are shown in Table 1. Half of the patients had a Diffuse Large B-cell Lymphoma, the great majority had a chemo-s disease and 50% had received more than two lines of previous therapy. Within the HIV-positive population, the median CD4+ T-cells before ASCT was 219/µL (range 60–720) and only one patient (2%) had detectable HIV viremia. All patients were on cART at the time of ASCT. Only two patients discontinued cART for at least 1 week after ASCT due to oral mucositis and hepatic toxicity, respectively. Co-infection with hepatitis B and hepatitis C virus was present in 1 (2%) and 12 (27%) HIV-positive patients and in 1 (2%) and 5 (11%) HIV-negative patients.
3.2. Clinical Outcomes
Overall, after a median follow-up of 51 months (IQR: 15–80), the 2-year and 4-year PFS were 71% and 65%, and the 2-year and 4-year OS were 78% and 74% for the entire series of 88 patients. PFS in the HIV-positive group was significantly higher compared to the HIV-negative population (2-year and 4-year PFS 81% and 78% vs. 61% and 51%, respectively, p = 0.027) (Figure 2). The 2-year OS and 4-year OS were both 81% for the HIV-positive patients and 75% and 67% for the HIV-negative patients (p = 0.15). The median follow-up for the two groups was 51 months (IQR: 8–87) for HIV-positive and 43 (IQR 24–73) for the HIV-negative population.
Overall, 30 patients (34%) had lymphoma relapse after ASCT. The relapse rate was significantly higher in HIV-negative (20 patients, 45%) compared to HIV-positive patients (10 patients, 23%) (p = 0.04). The median time to relapse was 57 months (IQR 12–89) for HIV-positive versus 27 months (IQR 5–53) for HIV-negative patients (p = 0.03). Twenty-six cases of death were recorded. Ten patients (23%) in the HIV-positive group died: seven from lymphoma, two from infection during CR (one had stopped cART by his own decision several months after ASCT), and one due to suicide. In the HIV-negative group, 16 patients (36%) died: 11 from lymphoma, four from infection (one patient in CR due to pneumonia, 11 months after ASCT, and three while receiving further therapies for lymphoma relapse), and one from a second tumor (pancreatic adenocarcinoma).
The CI plots of LSM and OCM are reported in Figure 3. The CIs of LSM and OCM at four years for HIV-positive versus HIV-negative patients were 16.5% vs. 26.1% and 2.5% vs. 7.2%, respectively.
3.3. Engraftment, Toxicity, and Infections
In all patients, peripheral hematopoietic stem cells were used for transplantation. The median number of CD34+ cells infused was 6.3 (IQR 5.0–7.3) × 10^6^/kg in the HIV-positive and 5.75 (IQR 4.9–7.9) × 10^6^/kg in the HIV-negative patients (p = 0.72). Neutrophil and platelet engraftment was achieved in all patients, except for one HIV-positive patient with chemo-r disease who died 10 days after ASCT because of sepsis. The median time to neutrophil and platelet engraftment was 10 days and 13 days for both HIV-positive and negative patients.
As infection prophylaxis HIV-negative patients received acyclovir and trimethoprim sulfamethoxazole until 3 months after ASCT. HIV-positive patients received acyclovir and fluconazole for 3 months after ASCT, and trimethoprim sulfamethoxazole for at least 6 months (or until CD4 count > 200/mcl). Levofloxacin was used in both groups during the neutropenic period before engraftment.
Eighteen (41%) HIV-positive patients had a total of 20 grade 3–4 treatment-related toxicity events (10 oral mucositis, 6 gastrointestinal toxicity/diarrhea, 3 enteritis, 1 seizure), while in the HIV-negative group, 16 grade 3–4 toxicity events were seen in 15 (34%) patients (14 oral mucositis, 2 enteritis) (p = 0.6). Nineteen patients (43%) in the HIV-positive group had an episode of fever of unknown origin (FUO) versus 26 (59%) in the HIV-negative group (p = 0.2). During the PRE-EP, there was a similar number of infectious events between the two groups (15 events in 14 patients and 11 events in 9 patients within the HIV-positive and negative group, respectively, p = 0.48). A documented bacterial infection was seen in 9 HIV-positive patients (20%) (including 3 g-negative and 4 g-positive episodes of sepsis), and in 7 HIV-negative patients (16%) (including 3 g-negative and 1 g-positive episodes of sepsis). A pneumonitis was recorded in one HIV-positive and two HIV-negative patients. Two cases (4%) of asymptomatic cytomegalovirus (CMV) reactivation, one (2%) herpes zoster (HZV) infection, and one (2%) human herpes virus-6 (HHV-6) infection were seen in the HIV-positive group while only one (2%) HHV-6 infection was observed in the HIV-negative group. One C.parapsilosis sepsis was observed in one HIV-negative patient and one HIV-positive patient had a probable invasive pulmonary aspergillosis. During the POST-EP there was a significant majority of infections or febrile events in the HIV-positive population compared to the HIV-negative group (34 vs. 17, respectively, p = 0.02). A total of 29 documented late infections occurred in 23 HIV-positive patients, including 5 bacterial infections, 20 viral infections (8 CMV, 11 HZV, 1 Rhinovirus pneumonia), and 4 cases of pneumonia. In the HIV negative-population, 12 patients had 15 documented infection events: two bacterial infections, 10 viral (7 CMV and 3 HZV), and 3 cases of pneumonia.
3.4. Predictive Factors for Relapse and Mortality
Considering the whole series of 88 patients, at univariable Cox regression analysis, two treatment lines prior to ASCT (HR: 0.07; p = 0.01) and chemo-refractory disease at ASCT (HR: 32; p < 0.01) significantly correlated with lower PFS. HIV infection resulted in being a protective factor for PFS (HR: 0.43; p = 0.03). Age (HR: 1.04; p = 0.03), NHL T histology (HR: 3.1; p = 0.05) and chemo-refractory disease at ASCT (HR: 6.6; 95% CI: 1.6–27; p = 0.01) were significantly correlated with a higher risk of death.
4. Conclusions
Thanks to the widespread use of cART, and the improvement in supportive care, standard-dose chemotherapy and HDT with ASCT are nowadays offered to HIV-positive patients with lymphoma with the same indications as for the HIV-negative general population.
However, access to target therapies and modern immunotherapies is still limited to PLWH, due to socio-economic factors and inadequate research to support safety and efficacy in this population. In the present study, we compared the outcomes of ASCT among two series of lymphoma patients affected or not affected by HIV infection using a 1:1 propensity score matching to reduce the bias of the retrospective comparison. Unpredictable satisfactory outcomes were previously reported for HIV-positive patients, comparable to HIV-negative subjects, with a surprising trend toward less relapses in the HIV-positive population [11,13,14,15].
The main result of our study was the significantly lower relapse rate in the HIV-positive group, which resulted in statistically significant higher PFS in PLWH compared to HIV-negative patients. This has also resulted in a not statistically significant trend toward improved OS in HIV-positive patients. PFS and OS of HIV-positive patients in the present study are in line with previous reports [9,18].
The fascinating finding of better PFS in patients with HIV infection compared to the general population is difficult to interpret. A beneficial effect of ASCT on the underlying HIV infection and on the immune status of patients with HIV may be hypothesized. Highly myelotoxic chemotherapy could deplete the reservoir that harbors HIV and facilitates immune recovery, and the restoration of an effective immune system might be relatively more beneficial in lymphomas developing in the context of failing immune response than in immunocompetent patients [19]. In hematologic malignancies, there are several examples of immunodeficiency-driven diseases that benefit from immune reconstitution, by simply reducing or modifying immune suppression, and several cases of lymphoma regression with treatment of HIV alone have been reported [20,21,22]. Moreover, a favorable long-term effect of cART may also play a role in the reduction in the relapse risk in HIV-Ly. Antiviral drugs included in cART regimens have been reported to exert a direct antineoplastic action [23,24,25]. Moreover, several studies have demonstrated the efficacy of the antiretroviral zidovudine, used in combination with interferon-α, against some adult T-cell leukemia subtypes, a disease etiologically associated with the human T-cell leukemia retrovirus type I. It is uncertain whether these drugs function via antiviral activity in cells in the tumor or microenvironment or through mechanisms other than antiviral activity [26]. Even if antiviral drugs have not been approved as antiproliferative agents, promising in vitro studies have demonstrated that nucleoside/nucleotide analog, reverse transcriptase inhibitors or integrase inhibitors can modulate cell growth and differentiation across various cancer types [27,28,29]. Investigations are ongoing to identify agents with the ability to inhibit key enzymes that play a crucial role in DNA metabolism and their possible application as antiretroviral and antitumoral agents [30].
In our study, we did not find significant differences both in acute toxicity and early infections after ASCT between the two groups of HIV-positive and negative patients. Instead, infections occurring later after engraftment were significantly higher in PLWH, and were mainly of viral origin. An increased rate of infections was also reported by the Spanish group [11], without a detrimental effect on survival. A previous study found a comparable immunologic recovery after ASCT between HIV-positive and negative patients, while other studies reported a delayed recovery in PLWH irrespective of efficient cART [11,19]. It is also known that chronic inflammation, immune cell metabolic dysregulation, and cellular dysfunction persist in PLWH even in the presence of effective cART and suppressed HIV viremia [31]. Our experience underlines the need for optimal supportive measures and careful follow-up in HIV-positive patients. Anyway, in our study not only LSM but also OCM showed a trend in favor of PLWH.
In conclusion, our results increase the awareness of ASCT as an effective curative option for patients with HIV-Ly and chemo-sensitive disease. ASCT indeed appeared to be highly effective in our study, and we reported for the first time a significantly lower relapse rate in HIV-positive patients compared to the general HIV-negative population.
We are aware that future clinical studies in the HIV setting should focus on novel molecules and immunological approaches while considering the effects on the underlying HIV disease, and some preliminary experiences paved the way in this direction [32,33,34]. While waiting for these new therapeutic approaches, rapidly developing in the HIV-negative population [35], to be demonstrated as safe and effective in the setting of HIV, ASCT remains a highly effective treatment strategy for HIV-Ly. A collaboration between all the involved professional figures, particularly infectious disease specialists and hemato-oncologists, represents the key to the correct management of these patients to guarantee the best achievable oncological outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Robbins H.A. Pfeiffer R.M. Shiels M.S. Li J. Hall I. Engels E.A. Excess cancers among HIV-infected people in the United States J. Natl. Cancer. Inst.2015107 dju 50310.1093/jnci/dju 50325663691 PMC 4334816 · doi ↗ · pubmed ↗
- 2Kimani S.M. Painschab M.S. Horner M.J. Muchengeti M. Fedoriw J. Shiels M.S. Gopal S. Epidemiology of haematological malignancies in people living with HIV Lancet HIV 20207 e 641e 65110.1016/S 2352-3018(20)30118-132791045 PMC 10199168 · doi ↗ · pubmed ↗
- 3Re A. Cattaneo C. Montoto S. Treatment management of haematological malignancies in people living with HIV Lancet Haematol.20207 e 679e 68910.1016/S 2352-3026(20)30115-032791044 · doi ↗ · pubmed ↗
- 4Coghill A. Suneja G. Cancer care disparities in people with HIV in the United States Curr. Opin. HIV AIDS 201712636810.1097/coh.000000000000032027753654 PMC 6424354 · doi ↗ · pubmed ↗
- 5Uldrick T.S. Ison G. Rudelk M.A. Noy A. Schwartz K. Bruinooge S. Schenkel C. Miller B. Dunleavy K. Wang J. Modernizing Clinical Trial Eligibility Criteria: Reccomendations of the American Society of Clinical Oncology-Friends of Cancer Research HIV Working Group J. Clin. Oncol.2017353774378010.1200/JCO.2017.73.733828968173 PMC 5793223 · doi ↗ · pubmed ↗
- 6Gabarre J. Azar N. Autran B. Katlama C. Leblond V. High-dose therapy and autologous haematopoietic stem-cell transplantation for HIV-1-associated lymphoma Lancet 2000251071107210.1016/S 0140-6736(00)02041-910744095 · doi ↗ · pubmed ↗
- 7Re A. Cattaneo C. Michieli M. Casari S. Spina M. Rupolo M. Allione B. Nosari A. Schiantarelli C. Vigano M. High-dose therapy and autologous peripheral-blood stem-cell transplantation as salvage treatment for HIV-associated lymphoma in patients receiving highly active antiretroviral therapy J. Clin. Oncol.200314423442710.1200/JCO.2003.06.03914581441 · doi ↗ · pubmed ↗
- 8Krishnan A. Molina A. Zaia J. Nademanee A. Kogut N. Rosenthal J. Woo D. Forman S.J. Autologous stem cell transplantation for HIV associated lymphoma Blood 2001983857385910.1182/blood.V 98.13.385711739198 · doi ↗ · pubmed ↗