Differences in Pressure Pain Threshold and Strain Elastography Between Women with and Without Fibromyalgia: A Cross-Sectional Study
María Aguilar-García, María Encarnación Aguilar-Ferrándiz, Ana González-Muñoz, Santiago Navarro-Ledesma

TL;DR
The study compares pain sensitivity and tissue stiffness in women with fibromyalgia and healthy controls at specific body sites.
Contribution
It provides empirical evidence on pressure pain thresholds and strain elastography differences at standardized tender-point sites in fibromyalgia.
Findings
Women with fibromyalgia had significantly lower pressure pain thresholds at all sites.
Fibromyalgia patients showed lower tissue deformation scores at most sites using strain elastography.
No differences in strain elastography were found at certain anatomical regions like the forearm and cervical area.
Abstract
Background: Fibromyalgia (FM) is a chronic pain condition primarily linked to central sensitization, although peripheral tissue-related factors have also been suggested. Ultrasound strain elastography (SEL) provides a semi-quantitative, operator-dependent estimate of tissue deformation under standardized compression, yet evidence comparing SEL findings and pressure pain sensitivity between FM and healthy controls at standardized tender-point sites remains limited. Objective: To compare pressure pain threshold (PPT) and SEL-derived tissue deformation between women with FM and healthy controls across standardized FM tender-point sites. Methods: In this cross-sectional study, 84 women (42 with FM; 42 healthy controls) were recruited from a private rehabilitation center in Málaga (Spain). PPT and SEL were assessed bilaterally at 13 standardized tender-point sites. Between-group differences…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1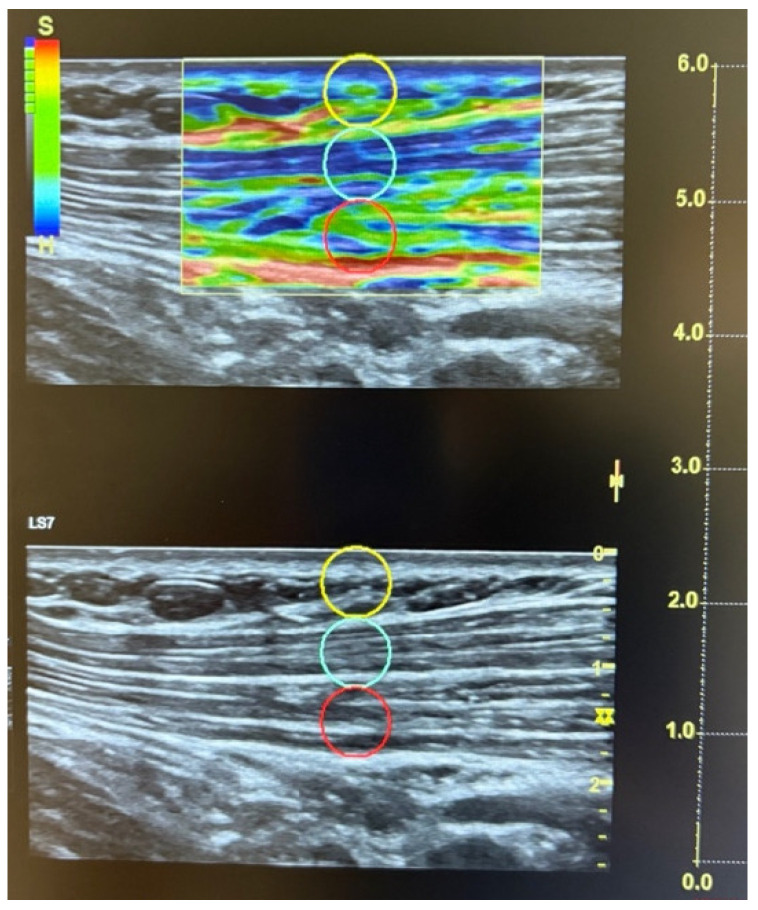 Figure 2
Figure 2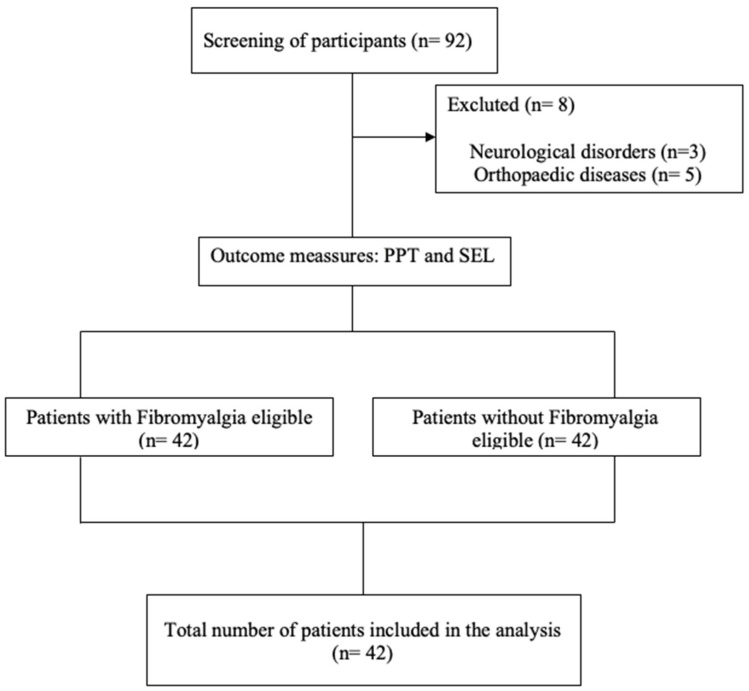 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFibromyalgia and Chronic Fatigue Syndrome Research · Pregnancy-related medical research · Myofascial pain diagnosis and treatment
1. Introduction
Fibromyalgia (FM) is a syndrome of uncertain etiology characterized by chronic widespread musculoskeletal pain, accompanied by symptoms such as dysesthesia, fatigue, morning stiffness, tender points (TPs), headache, sleep disturbances, anxiety, and cognitive impairments. Although FM is primarily conceptualized as a central sensitization syndrome, peripheral tissue-related factors have been proposed as potential contributors or secondary adaptations to persistent pain, which remains an unresolved issue [1,2,3,4,5].
The prevalence of fibromyalgia varies depending on the diagnostic criteria applied [6]. The most commonly used diagnostic framework is established by the American College of Rheumatology (ACR), which has evolved over time from tender point–based approaches to symptom-based criteria, including widespread pain lasting for at least three months, pain elicited by 4 kg of digital pressure, and widespread tenderness assessed through a standardized map of characteristic musculoskeletal tender points [4,6,7,8]. According to the latest 2016 update by ACR, the diagnostic criteria for FM must include widespread pain in at least 4 of 5 body regions, symptoms or pain persisting for at least 3 months, or elevated scores on the Widespread Pain Index (WPI) or the Symptom Severity Scale (SSS), indicating a worsening in both the extent and intensity of pain [3]. Although these criteria support the differential diagnosis of FM from other rheumatic and pain-related disorders, they do not exclude the possibility of coexisting conditions [3]
The global prevalence of FM ranges from 2 to 3% [6,9], with reported rates in Europe varying between 2.1 and 2.4%. In Spain, the prevalence is 4.2% among women and 0.2% among men [9,10,11,12,13,14], with the highest frequency observed in individuals aged 50 to 59 years [11,12,15,16,17].
Although the pathophysiological origin of FM remains unclear, current evidence supports its classification as a central sensitization syndrome [6]. Central sensitization is defined as a mechanism of amplified neuronal signaling within the central nervous system (CNS) [6,18], resulting in heightened pain perception. This phenomenon involves, among other factors, dysfunction of the hypothalamic–pituitary–adrenal (HPA) axis, which plays a key role in modulating stress responses and regulating neuroendocrine processes associated with pain [6,18,19,20,21,22]. Both ascending and descending pain pathways, as well as neurotransmitter systems, may be altered, which contributes to the presence of hyperalgesia and allodynia in individuals with fibromyalgia [6,18,20,21]. In parallel, peripheral sensitization refers to an augmented response of peripheral nociceptors, potentially increasing nociceptive input and contributing to site-specific pain sensitivity [6,16,20,21,23,24,25].
From a conceptual standpoint, central sensitization is considered a primary driver of widespread pain in FM, whereas peripheral tissue alterations—if present—may act as modulators, local amplifiers, or secondary adaptations to chronic pain and altered autonomic/inflammatory milieu. Moreover, this condition of central sensitization and chronic pain involves a low-grade inflammatory state and alterations in brain regions responsible for pain processing and behavioral regulation [5,26,27]. On the other hand, peripheral sensitization involves an augmented response of peripheral nociceptors, which leads the neuronal system to progressively respond to increasingly milder stimuli [6]. Previous studies have investigated and demonstrated the relationship between psychological factors and autonomic symptoms in individuals with FM [5,6,26,28,29]. Low-grade inflammation present in patients with FM, along with sympathetic nervous system activity, affects the elasticity of soft tissue and even cartilaginous tissue [5,30,31,32,33,34].
Numerous techniques, including magnetic resonance imaging (MRI), microanalytical techniques, infrared thermography, and ultrasonography, have been employed to quantify and assess myofascial pain in FM [6,35]. Recently, ultrasound-based techniques such as strain elastography have emerged, facilitating a more accessible and clinically applicable assessment of tissue-related pain features [36,37,38]. However, ultrasound elastography encompasses different modalities with distinct outputs; therefore, specifying the technique is essential. In particular, strain elastography (SEL) provides an operator-dependent, semi-quantitative estimate of tissue deformation under controlled compression, which differs conceptually and metrically from shear-wave elastography [36,39]. A recent study analyzed the correlations between psychological factors and SEL-derived tissue deformation patterns in patients with FM [40].
Previous studies have shown a relationship between the presence of tender points (TPs) and musculoskeletal disorders such as FM. A tender point (TP) can be defined as a specific localized area that may be found in muscle tissue, the muscle–tendon junction, fat pads, or the bursal region, and is characterized by extreme sensitivity to touch or pressure [23,35,41]. The term “TP” is used to describe areas where the application of local pressure elicits pain without radiation or reproduction of referred pain. TPs are commonly located in the back, face, neck, knees, calves, gluteus maximus, quadriceps, and hips [35,42]. In line with this, correlations between the pressure pain threshold (PPT) at characteristic FM pain points and tissue deformation pattern assessed by SEL have been studied in patients with FM [37].
Despite increasing interest in SEL and peripheral tissue characterization in FM, prior elastography literature remains heterogeneous regarding anatomical targets and elastography modalities, and evidence directly comparing SEL measures between women with FM and healthy controls at standardized FM tender-point sites, while concurrently quantifying pain sensitivity using PPT, remains scarce. Although previous studies have explored SEL-based tissue deformation responses at characteristic pain points in individuals with FM as potential outcome measures in relation to pain and psychological factors [37,40], there are currently no studies that have compared SEL-based measures with PPT between healthy individuals and patients with FM across standardized tender-point sites.
Therefore, the objective of the present study is to compare the PPT and SEL-derived deformation measures between a FM group and a healthy control group at the characteristic pain points described in patients with FM. It was hypothesized that women with FM would present lower PPT values and differences in SEL measures compared with healthy controls, reflecting differences in tissue deformation under compression rather than direct evidence of tissue pathology.
2. Materials and Methods
2.1. Study Design
This was a cross-sectional observational study. Ethical permission was approved by the Ethics Committee of Human Research at the University of Granada, Spain (approval number: 1044/CEIH/2020). The study was conducted in accordance with the principles of the Declaration of Helsinki and in line with the Statement of Recommendations for Observational Studies (STROBE).
2.2. Setting
The total study sample, consisting of 84 participants, was recruited from a private rehabilitation center in the province of Málaga, Spain, using a convenience sampling approach based on voluntary participation.
2.3. Sample
A sample of 84 women participated in this study. Forty-two women comprised the control group, and forty-two were assigned to the fibromyalgia group. Participants in the FM group did not receive any type of treatment in order to avoid potential interference with the measurements collected.
A physiotherapist was responsible for recruiting participants at a private center in Málaga and for assigning them to their respective groups. Compliance with the inclusion and exclusion criteria for group allocation was also supervised by a physiotherapist. Participation in the study was voluntary, and only women were included to reduce sex-related variability in pain sensitivity and SEL-derived deformation measures.
All SEL and PPT measurements were performed by a single experienced evaluator. However, intra-observer reliability was not formally assessed in the present study.
The evaluator was not blinded to group allocation. Limb dominance was determined by self-report, asking participants to indicate the upper limb they preferentially used for daily activities.
2.3.1. Healthy Group
Inclusion criteria
-Aged between 18 and 64 years.-Participants not diagnosed with fibromyalgia.
Exclusion criteria
-Presenting any inflammatory, orthopedic, or neurological disorder.
2.3.2. Fibromyalgia Group
Inclusion criteria
-Aged between 18 and 64 years.-Being diagnosed with fibromyalgia according to the ACR classification criteria.
Exclusion criteria
-Presenting any inflammatory, orthopedic, or neurological disorder.
2.4. Outcome Measures
2.4.1. SEL-Derived Tissue Deformation Assessment
Ultrasound strain elastography (SEL) was used to assess relative soft-tissue deformation behavior under compression at standardized tender-point sites. All measurements were performed by a physiotherapist with 11 years of experience in ultrasound imaging, using a Logiq S7 device with a 15 MHz linear probe (GE Healthcare, Milwaukee, WI, USA), acknowledging the operator-dependent nature of the technique. The transducer was placed longitudinally along the muscle fibers, with the center of the probe positioned over the tender points (TPs) in the regions previously described [43] and with the patient positioned according to the established TP identification protocol (Figure 1) [44,45].
Compression magnitude was monitored and standardized using the system’s built-in quality control (“dedicated software”), which displays compression adequacy via green bars; only sequences meeting the recommended quality (green bars) were retained for analysis. The recommended compression size was approximately 2–5 mm. The elastography color scale displayed red (hard), green (medium), and blue (soft) tissue patterns, accompanied by a reference bar with ‘S’ (soft) at the top and ‘H’ (hard) at the bottom.
SEL values ranged from 0 to 6 (0 = greater deformation; 6 = lower deformation) according to the manufacturer’s algorithm, reflecting semi-quantitative deformation estimates rather than direct measures of tissue stiffness or pathology. The exact raw strain value was calculated using a standardized 5 mm circular region of interest (ROI) placed within the selected area, following manufacturer instructions and previous studies (see Figure 2). Three high-quality acquisitions were obtained per site, and the mean of the three measurements was used to minimize intra-observer variation. Following the ACR criteria, a total of twenty-six points—thirteen on the dominant side and thirteen on the non-dominant side—were assessed [15]: (i) suboccipital muscle insertions; (ii) anterior aspect of the lower cervical intertransverse space (C5–C7); (iii) midpoint of the trapezius muscle (upper border); (iv) supraspinatus origin, above the scapular spine near the medial border; (v) paraspinal region at mid-scapular level, 3 cm lateral to the midline; (vi) second costochondral junction (second rib); (vii) level of the fourth rib at the anterior axillary line (lateral pectoral region); (viii) 2 cm distal to the epicondyle; (ix) medial epicondyle; (x) distal dorsal third of the forearm; (xi) upper outer quadrants of the buttocks, in the anterior fold of the gluteal muscle; (xii) greater trochanter, just posterior to the trochanteric prominence; and (xiii) medial fat pad of the knee.
2.4.2. Pain Pressure Threshold
A standard pressure algometer with a contact surface of 1 cm^2^ (FPK 20; Wagner Instruments, Greenwich, CT, USA) was used to measure the pressure pain threshold (PPT) at the 13 points on each side identified as characteristic of fibromyalgia according to the ACR consensus [15], following the established protocol [46].
PPTs were measured at the exact same points where tissue deformation was assessed using SEL. Standardized instructions were provided prior to testing to reduce potential learning effects, and all measurements were conducted by a physiotherapist with prior specific training. At each site, three consecutive PPT measurements were obtained and the mean value was used for analysis to improve measurement stability and reduce random error. The analyses performed using ultrasound strain elastography and pressure pain threshold were purely exploratory in nature.
2.5. Statistical Analysis
SPSS Statistics software version 24 for Windows (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. The Shapiro–Wilk test was applied to assess the normality and distribution of the variables. Descriptive variables with a Shapiro–Wilk p-value > 0.05 were expressed as mean ± standard deviation (SD), while those with a p-value < 0.05 were presented as median and interquartile range (IQR). Descriptive variables are shown in Table 1. Descriptive data for PPT and SEL are presented in Table 2 and Table 3, respectively. To analyze between-group differences, Student’s t-test was applied to variables with Shapiro–Wilk p > 0.05, and the Mann–Whitney U test was used for variables with Shapiro–Wilk p < 0.05. Group differences in PPT are presented in Table 4. Group differences in SEL are shown in Table 5.
Because multiple anatomical sites were analyzed, an increased Type I error (false-positive) risk due to multiple comparisons was considered. Therefore, p-values were adjusted using false discovery rate (FDR) control (Benjamini–Hochberg; q = 0.05) across site-level tests. For p-values reported as <0.001, a conservative value of 0.001 was used for the adjustment. Effect sizes (Cohen’s d) were additionally reported to quantify the magnitude of between-group differences independently of statistical significance. All analyses were conducted on a site-specific basis. No averaging of dominant and non-dominant sides was performed at any stage of the analysis. These effect sizes quantify between-group differences and do not imply causality in this cross-sectional design. PPT was treated as the primary outcome of the study, and all analyses involving SEL were predefined as exploratory and site-specific.
2.6. Sample Size
The sample size was estimated using G*Power version 3.1.9.7 (Heinrich Heine University, Düsseldorf, Germany). Based on data from a previous cross-sectional study that assessed pressure pain threshold via sonoelastography in individuals with nonspecific lumbopelvic pain<sup>31</sup>, a minimum of 18 participants with FM was required to achieve a statistical power of 80% with an alpha level (α) of 0.05 [47]. Given the exploratory nature of the present study and the intention to perform between-group comparisons across multiple anatomical sites, the target sample size was increased to enhance statistical precision and robustness. Ultimately, the final sample included a total of 84 women, with 42 assigned to the control group and 42 diagnosed with FM.
3. Results
3.1. Sociodemographic Characteristics
The sociodemographic characteristics are shown in Table 1, Table 2 and Table 3. Eighty-four women participated in the study. A total of 42 participants were included in the control group and 42 in the FM group. All participants met the inclusion and exclusion criteria established for this study. A flow diagram has been included (Figure 3). Effect sizes (Cohen’s d) are reported in Table 4 and Table 5 to quantify the magnitude of between-group differences across anatomical sites.
3.2. Differences in PPT and SEL Between the Control Group and the Fibromyalgia Group
Table 4 presents the between-group differences in PPT variables analyzed using Student’s t-test and the Mann–Whitney U test. To address the increased Type I error (false-positive) risk associated with multiple site-level comparisons, p-values were additionally adjusted using false discovery rate control (Benjamini–Hochberg; q = 0.05). Results for PPT and SEL are presented in Table 4 and Table 5, respectively. All PPT comparisons remained significant after FDR correction.
Table 5 presents Student’s t-test results and Mann–Whitney U test results for between-group differences in SEL variables. To address the increased Type I error (false-positive) risk associated with multiple site-level comparisons, p-values were additionally adjusted using false discovery rate control (Benjamini–Hochberg; q = 0.05). Results for PPT and SEL are presented in Table 4 and Table 5, respectively.
4. Discussion
The present study aimed to investigate whether differences in pressure pain thresholds at TPs and in SEL measures exist between women with and without FM. All findings should be interpreted cautiously given the cross-sectional, exploratory design, the heterogeneous anatomical targets assessed, and the increased risk of Type I error due to multiple testing across sites. Women in the FM group exhibited markedly lower PPT values than the control group across all assessed tender-point sites. Beyond statistical significance (p < 0.01 at all sites), the magnitude of these differences was consistently very large (Cohen’s d range −2.18 to −3.78), supporting robust pressure pain hypersensitivity across regions.
With respect to SEL, between-group differences were site-dependent, and the pattern was notably less uniform than that observed for PPT. It is important to note that SEL reflects operator-dependent, imaging-based tissue deformation responses under compression rather than direct measures of tissue stiffness or elasticity. To mitigate Type I error, p-values were additionally adjusted using false discovery rate control (Benjamini–Hochberg). After FDR correction, SEL between-group differences remained significant at most sites (19/26), with effect sizes ranging from negligible to large across locations (Cohen’s d −0.07 to −1.93). No significant SEL differences were observed at the forearm (dominant and non-dominant), lower cervical region (non-dominant), paraspinal region (dominant and non-dominant), and lateral pectoral regions (dominant and non-dominant).
4.1. Comparison with Other Studies
The data presented in this study support the presence of marked alterations in pressure pain sensitivity in fibromyalgia and suggest site-dependent differences in ultrasound strain elastography (SEL) measures. The statistically significant results found when analyzing between-group differences in pressure pain thresholds were consistent with previous literature, which described FM as a condition characterized by enhanced pain perception, reduced pain thresholds, hyperalgesia, and allodynia [6,18,21]. Previous studies used the same protocol to measure pressure pain thresholds in women with FM [14,22,37]; however, to the best of current knowledge, the concurrent application of this PPT protocol together with SEL in both the FM group and a healthy control group across a standardized tender-point panel has been scarcely investigated. Although the pathophysiological processes responsible for fibromyalgia are still being investigated, the condition is currently defined as a central sensitization syndrome based on the available evidence [6,18,24]. Alterations in functional neuroimaging findings and in neurotransmitters involved in sensory and pain transmission have been reported in patients with fibromyalgia, indicating the presence of widespread hyperalgesia and/or allodynia [21,24,48]. These central alterations may help explain the reduced tolerance to pressure pain thresholds observed in the FM group.
Regarding SEL findings, it should be emphasized that this technique provides an operator-dependent, imaging-based representation of tissue deformation under compression rather than a direct measurement of intrinsic tissue stiffness, elasticity, inflammation, or pathology. Accordingly, SEL findings cannot be used to infer specific neurochemical or pathophysiological mechanisms. Previous studies have reported alterations in neurotransmitter systems in FM, including increased levels of excitatory mediators and reduced inhibitory modulation [49,50,51,52]; however, these mechanisms are related to central pain processing and should be interpreted independently of SEL-derived measures.
Due to alterations in the central nervous system, in addition to central sensitization, patients with fibromyalgia are also characterized by neurovegetative symptoms and peripheral sensitization, as well as comorbidities such as irritable bowel syndrome, gynecological disorders, chronic fatigue syndrome, postural orthostatic tachycardia, circadian variations in blood pressure, and an exaggerated response to auditory, thermal, or mental stimuli [5,21,22,25,34,53,54,55]. Inflammatory processes are also known to be present in both peripheral structures and within the central nervous system in relation to fibromyalgia [6,56,57].
Within this complex clinical context, alterations in the central nervous system, along with autonomic symptoms and the low-grade inflammation observed in fibromyalgia, may indirectly influence peripheral tissue behavior. However, it should be emphasized that provides a semiquantitative assessment of tissue deformation under compression and does not allow direct inferences regarding inflammatory status, autonomic dysfunction, or peripheral pathology. Therefore, any observed between-group differences in SEL-derived measures should be interpreted as secondary and non-specific adaptations, rather than as evidence of primary peripheral pathology [5,30,31,32,34].
In the present data, SEL findings were heterogeneous across anatomical sites: lower SEL scores were observed at most sites, whereas several regions showed no statistically significant differences. Importantly, effect-size estimates for SEL ranged from negligible to large (Cohen’s d approximately −0.07 to −1.93), underscoring site-dependent variability rather than a uniform peripheral pattern. The points that did not show significant differences between groups were the dominant and non-dominant forearm, non-dominant lower cervical region, dominant paraspinal area, and both dominant and non-dominant lateral pectoral regions. This heterogeneity warrants further investigation. A possible hypothesis is that regional loading and habitual use (particularly in upper-limb sites) may contribute to more control-like SEL patterns in some locations; however, this interpretation remains speculative and should be tested by incorporating objective physical activity and muscle-function measures [5,37,43]. In this line, future research should consider evaluating the level of physical activity in both groups and exploring potential correlations between physical activity, SEL measures, and pressure pain thresholds. This approach may help clarify the influence of functional movement on peripheral tissue characteristics and pain sensitivity in individuals with FM.
Comparison with previous studies remains limited, as evidence directly comparing SEL measures between women with and without FM is methodologically heterogeneous across elastography modalities and anatomical targets. However, between-group elastography comparisons have been explored using different techniques, but significant differences between groups were not found. These authors employed techniques different from those used in the present investigation. In their studies, Muro-Culebras and Cuesta-Vargas used sonomyography and sono-myelastography to measure stiffness at trigger points, whereas Karayol and Sibel applied shear wave elastography to assess elasticity in the rhomboid major muscle [35,58]. Such methodological diversity (e.g., strain vs. shear-wave approaches and differing anatomical targets) limits direct comparability and may partially account for discrepant findings.
It is important to highlight that the use of strain elastography to non-invasively assess tissue deformation behavior has gained increasing attention in recent years. Numerous studies have demonstrated its usefulness for the analysis of various anatomical structures, as well as a tool for evaluating the effectiveness of different interventions [14,36,38,59,60,61,62]. Therefore, the findings presented here, although contrary to those reported by Muro-Culebras and Cuesta-Vargas as well as by Karayol and Sibel, should be interpreted cautiously in light of differences in elastography modality and the exploratory nature of multi-site testing. Lower SEL scores in the FM group suggest differences in strain elastography outputs under standardized compression; however, SEL provides a semi-quantitative deformation-based measure and should not be overinterpreted as a direct indicator of “tissue stiffness” in the biomechanical sense. The present findings suggest that differences observed in SEL-derived measures coexist with well-established alterations in central pain processing in FM, without implying a uniform or specific peripheral tissue mechanical signature. Accordingly, the present results do not support the use of SEL as a mechanistic or diagnostic biomarker in FM.
Although alterations in the central nervous system may induce changes in the tensegrity of peripheral tissue structures, the systems involved in pain processing appear to be primarily responsible for the increased pain response observed in individuals with fibromyalgia. While this idea is consistent with current evidence, which links the pathophysiology of fibromyalgia to central sensitization, it should be interpreted cautiously given the operator-dependence, semi-quantitative nature of strain elastography and the absence of intra-/inter-rater reliability assessment in the present study. Strain elastography assessments are operator-dependent; further studies are required to confirm our findings. Also, it would be important to investigate whether other factors could explain the lower SEL values observed in the FM group compared to the control group, such as differences in physical activity levels, muscular condition, or related physiological variables, and whether these factors are correlated with pressure pain thresholds.
4.2. Clinical Application
These cross-sectional findings do not support diagnostic, prognostic, or monitoring use of strain elastography (SEL) in fibromyalgia. Nevertheless, SEL may be considered a complementary research tool to characterize tissue deformation response alongside clinical assessment and pain sensitivity measures but not as a tool for diagnosis, prognosis, or mechanistic inference.
The observed between-group differences in PPT and the site-dependent SEL pattern suggest that tissue deformation behavior under standardized compression may differ between the FM group and the control group at selected anatomical sites. However, SEL provides a semi-quantitative, deformation-based output and should not be overinterpreted as a direct measure of tissue stiffness or “elastic properties” in a biomechanical sense.
Although central sensitization remains the primary mechanistic framework for FM, the present SEL findings are compatible with the presence of differences in tissue deformation responses under compression and/or secondary adaptations to chronic pain; however, no causal or pathophysiological inferences can be drawn from this cross-sectional design.
The potential role of SEL in FM should therefore be framed as exploratory, and any clinical application (e.g., phenotyping or subgrouping) requires confirmation in adequately powered studies that include standardized acquisition protocols and formal intra- and inter-rater reliability assessment.
Longitudinal and interventional designs are also required before considering SEL for monitoring disease course or treatment response. Future research should determine whether SEL patterns are reproducible across operators and devices, and whether they relate to clinical outcomes when potential confounders (e.g., physical activity, muscle condition, and clinical management) are measured and controlled. Only then can the utility of SEL as a biomarker candidate for progression or therapeutic response be appropriately evaluated.
4.3. Strengths
It is important to emphasize several strengths of this study. To our knowledge, it is the first investigation to systematically evaluate SEL-derived tissue deformation measures across 26 standardized anatomical sites in women with FM compared with healthy controls. The combination of SEL with PPT measurements allowed for a more comprehensive characterization of the peripheral and sensory alterations associated with FM. All assessments were conducted by a physiotherapist with extensive experience in musculoskeletal ultrasound, ensuring methodological consistency, and triplicate measurements were taken at each site to enhance data reliability.
4.4. Limitations
Several limitations should be acknowledged. First, the cross-sectional design precluded the establishment of causal relationships between SEL-derived tissue deformation measures, PPT and central sensitization. Accordingly, no temporal, mechanistic, or casual inferences can be draw from the present findings.
Assessor were not blinded to group allocation, which may have introduced measurement bias. Although all assessments were performed by an experienced physiotherapist, the absence of assessor blinding represents a methodological limitation.
Although the sample size was sufficient to detect statistically significant differences, its magnitude may limit the generalizability of the findings to other populations.
In addition, SEL is an operator-dependent imaging technique and remains sensitive to variations in transducer placement and applied compression, even when standardized protocols are used.
Intra- and inter-rater reliability for SEL acquisition and interpretation was not assessed, which limits reproducibility and may contribute to variability across anatomical sites.
Furthermore, although FDR control was applied, the analysis involved a large number of site-level comparisons and the results should therefore be considered multiple anatomical sites and should be considered hypothesis-generating. Residual Type I error risk and site-dependent heterogeneity cannot be fully excluded. Accordingly, all site-specific SEL analysis should be interpreted as exploratory and hypothesis-generating, whereas PPT findings represent the primary outcome of the present study.
Only women were included in the present study, which limits the applicability of the findings to male patients with FM.
Finally, the absence of systematically collected data on physical activity levels, occupational exposure, pharmacological management and other concomitant treatments precluded control for these potential confounders, which may have influence.
4.5. Future Research
Further research is needed to examine whether PPT values and SEL-derived tissue deformation measures change over time and in response to interventions in women with fibromyalgia, using longitudinal and interventional designs. Such studies should incorporate standardized acquisition protocols and formal intra- and inter-rater reliability assessment for SEL to establish measurement reproducibility given the operator-dependent, semi-quantitative nature of the technique before evaluating clinical utility. It would also be useful to incorporate tools that assess psychological variables, physical activity levels, and muscular condition in order to explore their potential correlations with pressure pain threshold and SEL measures in women with FM, and to determine whether these variables explain site-dependent heterogeneity in SEL outcomes without implying direct mechanistic or pathological inferences. In addition, systematically recording potential confounders related to clinical management (e.g., pharmacological treatment and other concomitant therapies) would strengthen interpretability of future findings.
5. Conclusions
In this cross-sectional study, women with FM showed lower PPT and site-dependent differences in SEL measures at standardized tender-point sites compared with healthy controls. Given the exploratory design, the operator-dependence, semi-quantitative nature of SEL, and multiple testing across anatomical sites, these findings should be interpreted cautiously and do not establish causal or mechanisms interpretations. Future longitudinal and interventional studies incorporating standardized reliability assessment and predefined primary outcomes are warranted to confirm the observed patterns and clarify their clinical relevance.
Further research should also examine the joint contribution of psychological variables, physical activity, muscle condition, and pain sensitivity to better characterize interactions between central mechanisms and SEL-derived tissue deformation features, without implying direct peripheral pathology in chronic pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arnold L.M. Bennett R.M. Crofford L.J. Dean L.E. Clauw D.J. Goldenberg D.L. Fitzcharles M.-A. Paiva E.S. Staud R. Sarzi-Puttini P. AAPT Diagnostic Criteria for Fibromyalgia J. Pain 20192061162810.1016/j.jpain.2018.10.00830453109 · doi ↗ · pubmed ↗
- 2Bair M.J. Krebs E.E. Fibromyalgia Ann. Intern. Med.202017210.7326/AITC 20200303032120395 · doi ↗ · pubmed ↗
- 3Wolfe F. Clauw D.J. Fitzcharles M.A. Goldenberg D.L. Häuser W. Katz R.L. Mease P.J. Russell A.S. Russell I.J. Walitt B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria Semin. Arthritis Rheum.20164631932910.1016/j.semarthrit.2016.08.01227916278 · doi ↗ · pubmed ↗
- 4Sosa-Reina M.D. Núñez-Nagy S. Gallego-Izquierdo T. Pecos-Martín D. Monserrat J. Álvarez-Mon M. Effectiveness of Exercise Therapy in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials Bio Med Res. Int.20172017235634610.1155/2017/235634629291206 PMC 5632473 · doi ↗ · pubmed ↗
- 5Navarro-Ledesma S. Carroll J. González-Muñoz A. Pruimboom L. Burton P. Changes in Circadian Variations in Blood Pressure, Pain Pressure Threshold and the Elasticity of Tissue after a Whole-Body Photobiomodulation Treatment in Patients with Fibromyalgia: A Tripled-Blinded Randomized Clinical Trial Biomedicines 202210267810.3390/biomedicines 1011267836359198 PMC 9687325 · doi ↗ · pubmed ↗
- 6Jurado-Priego L.N. Cueto-Ureña C. Ramírez-Expósito M.J. Martínez-Martos J.M. Fibromyalgia: A Review of the Pathophysiological Mechanisms and Multidisciplinary Treatment Strategies Biomedicines 202412154310.3390/biomedicines 1207154339062116 PMC 11275111 · doi ↗ · pubmed ↗
- 7Lorente L.C. Ríos M.C.G. Ledesma S.N. Haro R.M.T. Barragán A.C. Correa-Rodríguez M. Ferrándiz M.E.A. Functional status and body mass index in postmenopausal women with fibromyalgia: A case–control study Int. J. Environ. Res. Public Health 201916454010.3390/ijerph 1622454031744126 PMC 6888241 · doi ↗ · pubmed ↗
- 8De Formación C. Revista de la Sociedad Española del Dolor 2009 Available online: https://www.elsevier.es/resed(accessed on 15 May 2025)