Lateral Cephalometric Radiography: Principles, Common Positioning Errors, and AI-Driven Quality Control
Rossana Izzetti, Maria Pisano, Chiara Cinquini, Lorenzo Cinci, Antonio Barone, Cosimo Nardi

TL;DR
This paper reviews lateral cephalometric radiography, focusing on proper positioning, common errors, and how AI can improve diagnostic accuracy.
Contribution
The paper introduces a synthesis of AI-driven quality control methods for improving diagnostic reliability in lateral cephalometric radiography.
Findings
Precise patient positioning is crucial to avoid inaccuracies in cephalometric measurements.
AI tools can enhance workflow consistency but require validation and human oversight.
LCR offers a favorable radiation dose and diagnostic utility compared to 3D imaging.
Abstract
This narrative review provides a contemporary synthesis of lateral cephalometric radiography (LCR), addressing both its foundational principles and the impact of technological integration, with a focus on enhancing diagnostic reliability. A structured literature search (PubMed, up to September 2025) was conducted around five domains: LCR’s diagnostic role, acquisition methods, positioning errors, comparisons with cone-beam computed tomography (CBCT), and Artificial Intelligence (AI)-driven quality control. Precise patient positioning—maintaining symmetry and a horizontal Frankfort plane—is paramount, as common errors (tilting, rotation, nodding) introduce quantifiable inaccuracies in key measurements. While digital innovation, particularly deep learning models for automated landmark detection and error flagging, improves the consistency of workflow, current AI tools require validation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1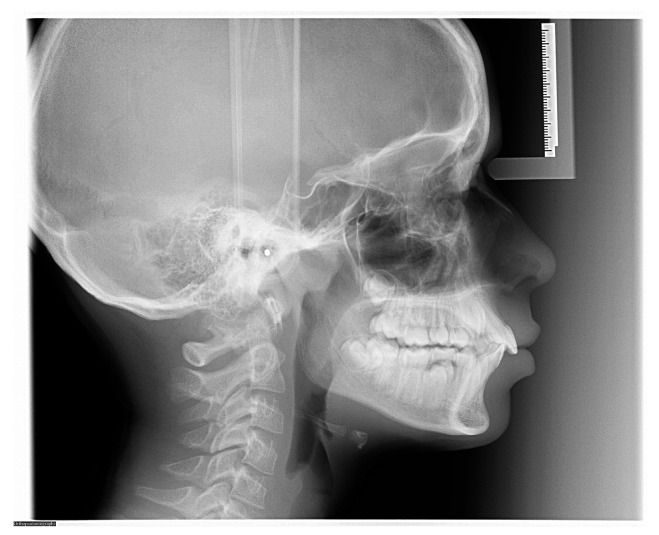 Figure 2
Figure 2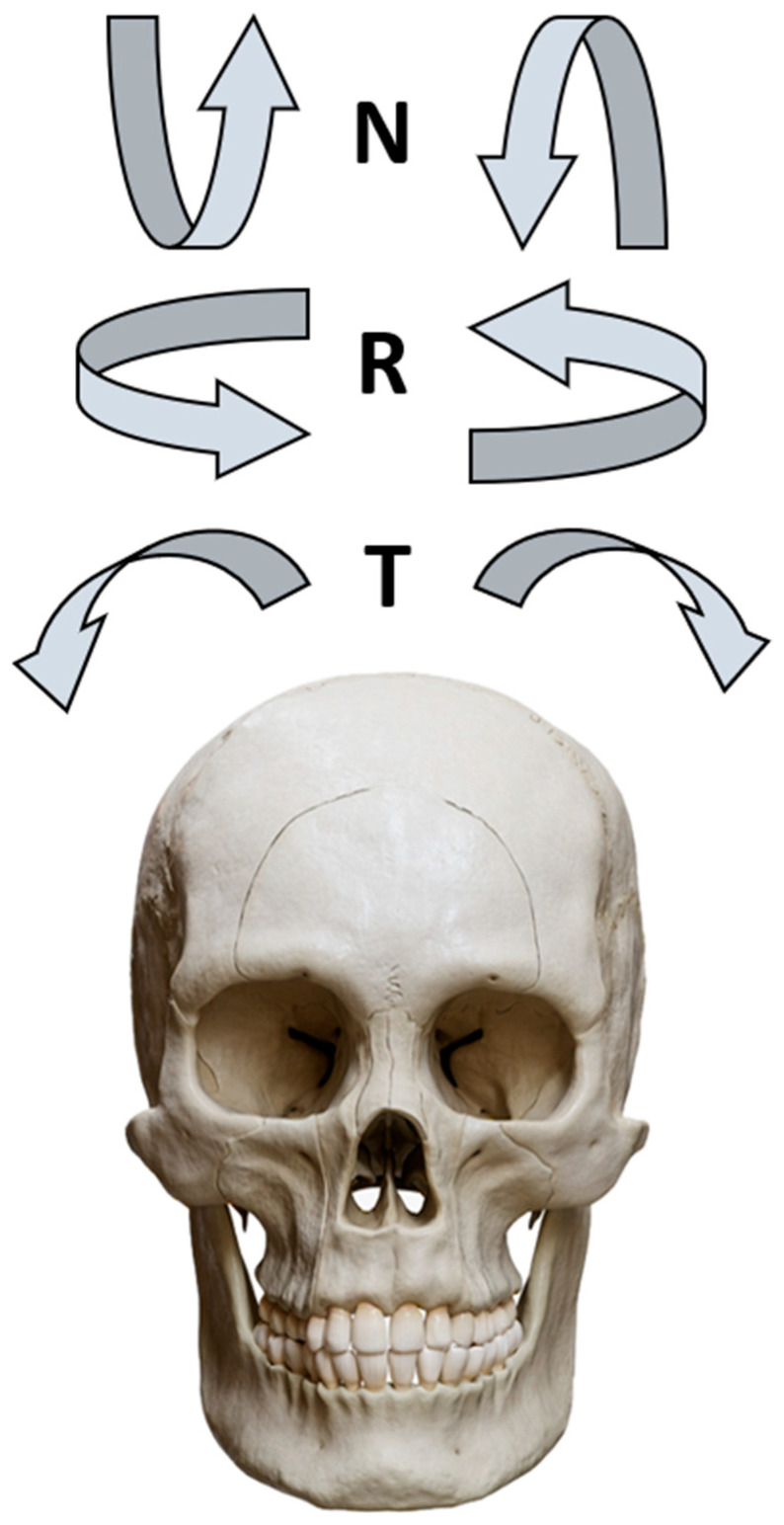 Figure 3
Figure 3 Figure 4
Figure 4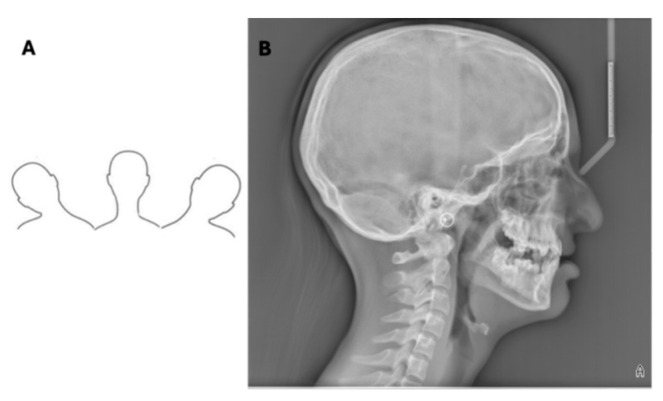 Figure 5
Figure 5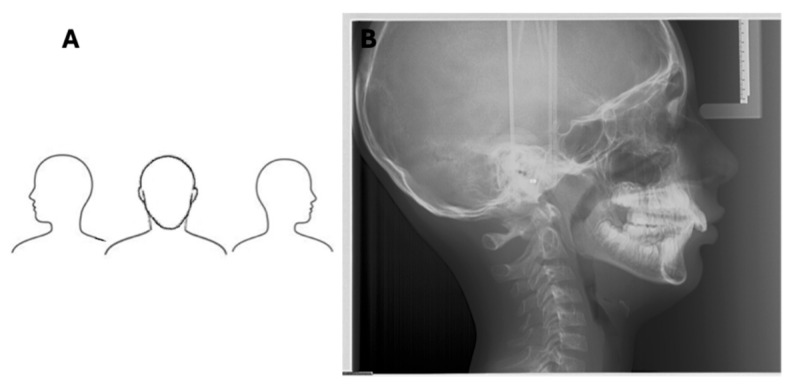 Figure 6
Figure 6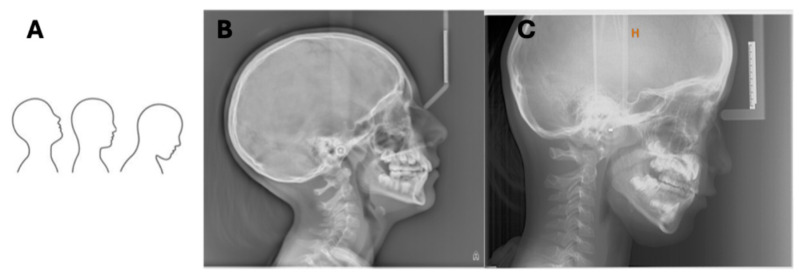 Figure 7
Figure 7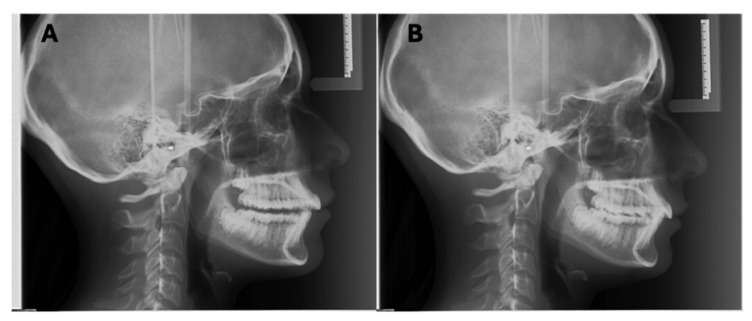 Figure 8
Figure 8 Figure 9
Figure 9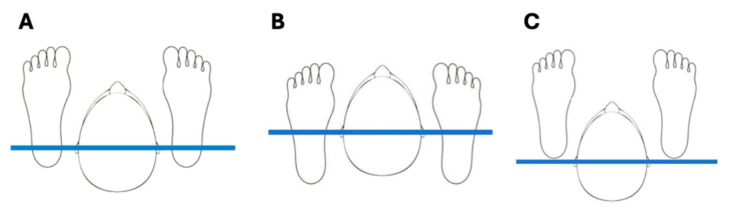 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Radiography and Imaging · Orthodontics and Dentofacial Orthopedics · Forensic Anthropology and Bioarchaeology Studies
1. Introduction
The lateral cephalometric radiograph (LCR) has been an integral part of orthodontic practice since its introduction in 1931, establishing a standardized two-dimensional (2D) representation of the craniofacial complex for diagnosis and treatment planning [1,2]. For decades, it has provided a critical tool for evaluating skeletal, dental, and soft tissue relationships. Despite its foundational role, the clinical utility and technical execution of LCR are subjects of ongoing debate and evolution [3,4]. While indispensable for quantitative assessment in many complex cases, inherent limitations of conventional 2D radiography—including projective geometric errors, sensitivity to patient positioning, landmark identification variability, and radiation exposure concerns, especially in pediatric populations—have prompted scrutiny of its routine necessity [5]. Concurrently, the technological landscape has transitioned from film-based systems to digital acquisition, and more recently, toward the integration of artificial intelligence (AI) for automated analysis and quality control [6]. However, this rapid technological shift, while promising enhanced efficiency and consistency, introduces new challenges regarding algorithmic validation, generalizability, and integration into established clinical workflows.
At present, a significant gap exists in the literature that synthesizes these parallel narratives: the importance of foundational acquisition principles and the potential of digital innovation. While technological advances are often documented, there is a need for a cohesive analysis of how innovations like AI-driven automation interact with—and can potentially mitigate—traditional sources of error to redefine the modern diagnostic pathway.
This narrative review, therefore, addresses this gap with a dual focus. First, it provides a detailed examination of the core principles of LCR image acquisition and a systematic analysis of common patient positioning errors, quantifying their impact on measurement accuracy. Second, it critically evaluates the latest technological advancements to analyze how these tools are creating a novel diagnostic workflow. By bridging fundamental knowledge with forward-looking innovation, this review aims to serve as a comprehensive and practical guide for clinicians and radiologists navigating the evolving standards of contemporary orthodontic practice.
2. Methods
The research was conducted by two groups of reviewers (Group 1: RI/MP/CC; Group 2: LC/AB/CN). Both groups attended an online meeting to ensure alignment during the article selection process. The literature search was structured around five domains, namely the role of LCR in orthodontics, acquisition methods, sources of error during LCR execution, comparisons with cone-beam computed tomography (CBCT), and AI-driven methods aimed at ensuring optimal image acquisition. The two groups of reviewers independently conducted a double Medline search via PubMed, including literature published up to September 2025. All relevant articles identified were discussed between the groups prior to inclusion in the review. No predefined or restrictive keyword strategy was applied.
3. The Role of LCR in Orthodontic Treatment Planning
LCR provides a reproducible, quantitative, and standardized assessment of craniofacial structures, which is useful for monitoring the direction and magnitude of facial growth, assessing dentoalveolar development, and accurately quantifying the skeletal and soft-tissue changes induced by orthodontic treatment over time [7,8]. The technique’s primary benefit lies in its serial comparability, enabled by the standardization of patient positioning using a cephalostat. This repeatability is critical for longitudinal evaluations, allowing clinicians to monitor progress [8]. Beyond skeletal and dental analyses, a correctly executed LCR enables the evaluation of the nasopharyngeal airway, cervical spine morphology, and hyoid bone position—structures intrinsically linked to craniocervical posture and respiratory function, which can influence craniofacial development [9]. Achieving this level of diagnostic accuracy is dependent upon a technically optimal image acquisition. The standardized geometry of the cephalostat, with fixed distances between the X-ray tube, the patient’s head (centered on the sella turcica), and detector, is designed to minimize geometric magnification and distortion, ensuring that linear and angular measurements remain consistent across serial radiographs [10].
However, the decision to obtain an LCR necessitates a careful risk–benefit analysis, balancing its diagnostic potential against radiation exposure, particularly in pediatric patients [11]. The evidence regarding its indispensability for orthodontic treatment planning is still debated [12].
The contradictory findings in the literature can be attributed to several factors, including heterogeneity in study samples (e.g., mix of simple and complex malocclusions), variability in clinician experience, and differences in methodological design [13].
Ultimately, LCR’s impact is not universal but is dictated by its role in specific clinical decision-making steps [14,15]. Therefore, the current evidence supports a selective, indication-based approach where LCR provides decisive quantitative data precisely where clinical judgment reaches its limits.
Studies indicate that the influence of LCR is case-dependent. For example, Devereux et al. [2] reported that LCR caused a fundamental change to the treatment plan, primarily in patients with skeletal Class II malocclusions, while Nijkamp et al. [13] found no such effect in cases of Class II/Division 1 malocclusion. Similarly, some studies found LCR altered planning in a limited number of cases [16,17], whereas others, like those by Dinesh et al. [3] and Durao et al. [12], reported minimal impact on final decisions in the majority of evaluated cases. This suggests that LCR’s value is most pronounced in differentiating between the dental and skeletal etiology of a malocclusion, quantifying the severity of a sagittal or vertical skeletal discrepancy, assessing the soft tissue profile and its relationship to underlying skeletal structures, and determining the need for and timing of growth modification or surgical intervention [17].
4. Technology and Acquisition Methods
The image acquisition methodology in LCR is defined by the type of detector, with significant implications for image quality, artifact potential, and clinical workflow. In analog (film-screen) or computed radiography (photostimulable phosphor plate) systems, a single, brief exposure captures the entire field of view instantaneously [18]. This “single shot” method is fast, minimizing the risk of motion blur. Single-shot systems typically capture the entire skull, including the vertex and occiput (Figure 1).
Early direct digital radiography (DR) systems often utilize a moving sensor bar that scans the craniofacial structures with a narrow radiation beam over several seconds (typically 3–6 s). Direct DR systems utilize a moving sensor bar that scans the craniofacial structures with a narrow radiation beam over several seconds [19]. This prolonged scanning time increases the risk of motion artifacts, which can degrade landmark clarity. Therefore, patient instruction and cooperation are more critical when using DR systems to ensure a still posture is maintained throughout the extended exposure. Importantly, the finite travel range of the sensor bar often truncates the posterior or superior skull regions, a limitation clinicians must acknowledge during interpretation [20]. While modern cephalometric analyses rarely require these peripheral structures, this limitation of DR should be considered, particularly in cases where cranial base assessment is needed [21,22]. DR detectors, however, increasingly employ large-format, single-shot flat-panel detectors that acquire the image instantaneously, similarly to computed radiography, thereby eliminating scan-time artifacts. Modern orthopantomography units with integrated cephalostats can automatically adjust the field of view based on patient anatomy, partially mitigating this issue [22,23].
The exposure technique in LCR is optimized for both diagnostic yield and patient safety. The standard use of a high-kilovoltage (“hard beam”) technique (100–110 kVp) provides the moderate contrast necessary to visualize both bony landmarks and the soft tissue profile simultaneously, which is essential for comprehensive analysis [24,25,26]. In pediatric patients, dose-optimization protocols may employ lower kVp settings while maintaining diagnostic quality. This technique also contributes to dose reduction, as fewer photons deposit their full energy in patient tissues [25,26]. While this can result in images that appear overexposed, digital post-processing allows for easy correction to achieve diagnostic quality—a significant advantage over analog methods where overexposure would render an image non-diagnostic [23]. Adherence to the ALARA (As Low As Reasonably Achievable) principle is paramount, especially for the pediatric and adolescent demographic, which constitutes the majority of orthodontic patients. This involves justifying each examination, employing optimized digital systems, and utilizing the exposure parameters that deliver the minimum dose required for an adequate diagnostic image [27].
LCR can also be acquired using hybrid imaging devices that combine panoramic, cephalometric, and cone-beam computed tomography (CBCT) capabilities in a single unit [28]. While offering workflow efficiency, the CBCT components in such hybrid devices often feature small fields of view suited for dentoalveolar imaging rather than full craniofacial capture. Dedicated large-field CBCT scanners, whether standalone or, less commonly, integrated into hybrids, can reconstruct synthetic 2D cephalograms from a 3D volumetric dataset. Although this provides a projection-error-free image, the associated radiation dose is typically higher than that of a standard 2D LCR, necessitating strict clinical justification [29].
5. Correct Execution
In LCR, the X-ray tube and detector are positioned at a standard distance of 1.524 m (5 feet), while the patient-to-detector distance is 15 cm. The consistent distance between the X-ray tube and the center of the patient’s head and between the center of the patient’s head and the detector limits intrinsic geometric distortions in two-dimensional imaging, particularly the magnification effect. This makes it possible to obtain repeatable measurements over time to compare examinations performed on the same patient at different stages of treatment [11]. The midpoint between the ear rods is considered the central point of the skull and corresponds to the sella turcica. From this central reference point, the block supporting the ear rods can be rotated to perform postero-anterior cephalometric projection. Specifically, the positioning for the frontal cephalogram is identical to that for the lateral plane, except the patient’s head is rotated 90 degrees towards the detector. LCRs allow for the visualization of the soft tissues of the face as there is a wedge filter at the X-rays source that absorbs part of the radiation, thereby making soft tissues perceptible in the radiograph (Figure 2).
The imperative for correct execution extends to patient safety. The diagnostic necessity of the examination must always be weighed against the principle of As Low As Reasonably Achievable (ALARA), particularly given that a significant proportion of orthodontic patients are children and adolescents [12]. Modern digital acquisition systems contribute to this balance by optimizing exposure parameters, often employing a higher-kilovoltage (“hard beam”) technique. This approach reduces patient dose while providing the moderate contrast necessary for delineating both bone landmarks and the soft tissue profile—a dual requirement for comprehensive cephalometric analysis [8,24]. Therefore, this meticulous technique not only safeguards the diagnostic reliability and reproducibility of the LCR but also aligns with the ethical obligation to minimize radiation exposure.
6. Errors in Patient Positioning During LCR
Positioning errors do not merely reduce image clarity; they systematically distort the projected relationships between craniofacial landmarks, leading to quantifiable inaccuracies in the angular and linear measurements that form the basis of cephalometric diagnosis and treatment planning. Specifically, tilting refers to lateral movement along the coronal plane; rolling refers to rotation around the vertical axis; and nodding refers to pitch movement around the transverse (inter-aural) axis. Such errors can be categorized as follows and are schematized in Figure 3:
- Lateral head movement (Tilting): Movement along the coronal plane, leading to asymmetrical images and difficulty assessing bilateral structures.
- Head rotation (Rolling): Rotation around the vertical axis, distorting midline structures and bilateral superimposition.
- Chin elevation or depression (Nodding): Alters the vertical relationships of facial structures, affecting the mandibular plane angle and facial height assessment.
- Misalignment of the Frankfurt plane: Results in incorrect orientation of the craniofacial structures relative to the true horizontal.
- Failure to achieve maximum intercuspation: The mandible must be in its most superior occlusal position where teeth are fully interlocked; failure to do so invalidates the assessment of arch relationships.
Radiopaque markers on the ear rods and frontonasal support are visible on the radiograph to verify correct positioning. Properly positioned ear rods appear as a single overlapping point or a distinct target image, indicating the absence of tilting or rolling, while the frontonasal support prevents nodding (Figure 4) [30,31]. Motion during exposure may manifest as blurred dental structures.
6.1. Horizontal Plane
An asymmetric head position on the horizontal plane typically results from incorrect placement of the ear rods. When the radiopaque markers are perfectly superimposed, a symmetric position is achieved [32]. Asymmetry due to patient positioning, rather than true anatomy, is evidenced by a lack of superimposition of the posterior mandibular rami, orbits, and external acoustic meati. Tilting displaces these structures in the cranio-caudal direction, while rolling causes misalignment in the antero-posterior direction (Figure 5 and Figure 6).
6.2. Sagittal Plane
Errors in the sagittal plane involve upward or downward head movement (nodding). The Frankfurt plane must be horizontal and parallel to the floor to project symmetric bilateral structures at the same height. Misalignment leads to nodding, which is often associated with compensatory spinal posture, resulting in an emphasis on cervical lordosis or straightening of the cervical spine (Figure 7) [33]. The frontonasal support is crucial for stabilizing the antero-posterior position of the head.
6.3. Occlusal Plane
Patients must maintain maximum intercuspation during exposure (Figure 8). Failure to achieve this necessitates a repeat examination to accurately assess the relationship between the upper and lower dental arches [32]. To facilitate this, patients should perform opening and closing movements, swallow, and then maintain a natural lip seal—neither separated nor pursed (Figure 9)—during the exposure. It is acknowledged that patients with malocclusions or craniofacial anomalies may not have a stable intercuspation; in such cases, retaking the LCR would only be harmful due to unjustified re-exposure.
To achieve a correct occlusion with dental crowns in maximum intercuspation, it is beneficial for the patient to perform some mouth-opening and -closing movements beforehand, then swallow and finally maintain occlusion during the radiation exposure, keeping the lips naturally closed. The lips should be in a competent position, neither separated nor pursed.
6.4. Cervical Spine
The alignment of the cervical spine and associated structures is critical for a standardized, reproducible head posture [34]. The “ear rods–malleoli axis” is a key mechanical principle: positioning the patient’s ankles (malleoli) directly under the vertical projection of the ear rods to the floor aligns the body’s weight-bearing axis, promoting a neutral, unstrained cervical posture (Figure 10A). Incorrect foot placement either anterior or posterior to this axis (Figure 10B,C) facilitates compensatory nodding of the head forward or backward, respectively, to re-establish balance, thereby altering the cervical spine’s radiographic representation.
6.5. Impact of Positioning Errors on Cephalometric Analysis
Head positioning errors can significantly impact the accuracy of cephalometric measurements, causing the incorrect identification of key landmarks like sella turcica, nasion, and gonion, which are critical anatomical references for assessing skeletal relationships [35].
These effects, such as a lateral head rotation (rolling) of 5°, can result in discrepancies of over 2° in the ANB angle and 2 mm in the Wits appraisal, while a 10° pitch (nodding) can alter the mandibular plane angle (SN-GoGn) by more than 3° and anterior facial height by up to 4 mm [22,30,32,33,35]. These changes can be clinically significant, potentially shifting diagnostic classifications (e.g., from skeletal Class I to Class II) or altering surgical treatment plans. A synthesis of quantified impacts from key studies is provided in Table 1.
Positioning errors become particularly problematic when comparing serial radiographs for growth assessment or treatment monitoring. Emerging AI-based tools are being developed to address positioning errors. Deep learning models, particularly convolutional neural networks (CNNs), are trained to detect specific error patterns [36]. Algorithms can specialize in identifying asymmetry in bilateral structures or identifying nodding by assessing the angle of the Frankfort plane or cervical spine alignment relative to a learned horizontal standard [18]. Other systems offer real-time feedback via preview monitors, allowing for repositioning before exposure, while post-processing software can algorithmically correct minor rotational (rolling) misalignments by digitally re-orienting the image to a standardized reference plane [37,38]. These AI-driven methods aim to reduce operator dependency and improve consistency, although their clinical integration requires validation across diverse patient cohorts and imaging devices. A checklist to minimize positioning errors is proposed in Table 2, and additional recommendation for the clinician is provided in Table A1 and Table A2.
7. Comparative Analysis of LCR, CBCT, and AI-Driven Innovations
In recent years, LCR has evolved from analog film-based systems into sophisticated digital platforms, offering enhanced resolution, lower radiation exposure, and excellent diagnostic accuracy [39]. The implementation of digital sensors and high-definition imaging software for 2D imaging has improved landmark visibility and minimized geometric distortion, facilitating more accurate evaluations [39,40]. However, its flat geometry may still be inadequate for studying anatomical volume and its evolution during growth. Consequently, even in orthodontics, CBCT has been significantly increasing in the last few years since this technique is capable of achieving precise reconstructions of bone structures in all three dimensions of space [41]. The advent of CBCT has introduced a new dimension to orthodontic imaging, offering an accurate visualization of complex anatomical relationships [42]. While CBCT eliminates projection errors and magnification artifacts, providing 86.4% accuracy in landmark identification within 1 mm for a majority of clearly defined craniofacial landmarks [43], it exposes patients to higher radiation doses than conventional radiographs. Reported ranges vary widely from approximately 50–600 µSv for CBCT versus 5–20 µSv for LCR, depending on device settings, field of view, and patient age [44,45]. It is important to note that these numeric comparisons are influenced by significant heterogeneity across studies, including differences in CBCT machine types, acquisition protocols, dosimetry methods, and landmark definitions. Furthermore, the cited accuracy percentage for CBCT landmark identification is derived from studies with specific sample characteristics and imaging conditions; generalizability may be limited by variations in operator experience, image quality, and anatomical complexity. Therefore, the role of CBCT in orthodontic diagnosis and treatment planning is still being evaluated due to the increased cost and interpretation time and the lack of standardized 3D cephalometric norms. Given that orthodontic patients are often children and adolescents, who are more sensitive to the effects of ionizing radiation, it is essential to weigh the potential benefits of CBCT against the risks of radiation exposure.
The most transformative innovation, however, is the integration of AI, which has revolutionized cephalometric analysis.
Contemporary AI tools are powered by sophisticated deep learning architectures. Modern Convolutional Neural Networks (CNNs) can achieve sub-2 mm mean radial error for landmark identification on standardized datasets, matching the intra-observer consistency of trained clinicians [44,45]. However, AI performance is contingent on the quality, size, and diversity of training datasets. Models trained on specific populations or imaging devices may suffer from reduced generalizability (dataset bias) and can struggle with atypical anatomy, severe malocclusions, or poor-quality images—scenarios where clinical expertise remains irreplaceable [46,47]. Therefore, AI currently functions best as an assistive tool, with human oversight being essential for verification, especially in complex cases.
Concurrently, cloud-based storage and digital workflow platforms have modernized data management, enabling the secure, real-time sharing of cephalometric records across multidisciplinary teams. This is particularly beneficial in complex treatments requiring coordination between various specialists and in the growing field of tele-orthodontics [48]. Evidence on the accuracy of digital setups and the influence of 3D predicted outcomes on patient expectations underscores the clinical implications of adopting digital cephalometric workflows and the need to validate predictive models against real outcomes [49]. While CBCT-based volumetric assessments can reveal anatomical relationships that are not visible on 2D radiographs [50], advanced algorithms—often generative adversarial networks (GANs) or other deep learning models trained on paired 2D–3D data—can now extrapolate pseudo-3D models from standard LCR, offering enhanced anatomical insight without increasing radiation burden [51]. These reconstructions are inferential approximations, not true measurements, and their accuracy is constrained by the inherent loss of 3D information in a 2D projection, limiting their current clinical utility [52,53].
The integration of AI into clinical practice also introduces ethical and regulatory considerations, including algorithmic transparency, data privacy, and the need for rigorous clinical validation to meet medical device standards [54].
Critically, these reconstructions are inferential approximations rather than true measurements; their accuracy is fundamentally constrained by the loss of 3D information in a 2D projection, making them unreliable for assessing transverse dimensions or asymmetries and limiting their validation primarily to research settings [52].
Collectively, these innovations are reshaping clinical practice and advancing orthodontic education and research, as digital platforms enable interactive learning, large-scale data analysis, and the development of predictive diagnostic tools. Nevertheless, the field must address key challenges—including algorithmic bias, data privacy in cloud systems, and the rigorous clinical validation of AI and pseudo-3D tools—to ensure these technologies are both equitable and robust. As digital technology continues to progress, LCR remains an essential and increasingly powerful instrument in modern orthodontic diagnostics, defined by its precision, efficiency, and adaptability [55].
8. Conclusions
Lateral cephalometric radiography remains a useful diagnostic tool in orthodontics when applied selectively and with appropriate clinical justification. The accuracy and reproducibility of cephalometric analysis are strongly dependent on correct image acquisition, as patient positioning errors can substantially affect landmark identification and measurement reliability, particularly in longitudinal evaluations.
Advances in digital imaging and artificial intelligence have improved workflow efficiency and consistency of analysis; however, they do not replace the need for standardized technique and careful patient positioning. AI-based tools may support landmark detection and quality control, but their clinical application still requires validation and professional oversight. Future progress hinges on establishing robust, multi-center validation pathways for AI tools and developing standardized cephalometric norms derived from 3D datasets to better inform 2D diagnostic criteria.
Compared with three-dimensional imaging, LCR continues to offer a favorable balance between diagnostic information and radiation exposure. While cone-beam computed tomography provides additional spatial detail, its routine use remains limited by the higher radiation doses and restricted indications. This narrative review is inherently limited by its methodological design, which, while comprehensive, does not constitute a systematic synthesis and may reflect the selective inclusion of evidence. However, LCR appears to retain a defined role in contemporary orthodontic practice when used according to indication-based criteria and established radiological principles.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang C.H. Randazzo L. Evolution of imaging and management systems in orthodontics Am. J. Orthod. Dentofac. Orthop.201614979880510.1016/j.ajodo.2016.03.01627241988 · doi ↗ · pubmed ↗
- 2Devereux L. Moles D. Cunningham S.J. Mc Knight M. How important are lateral cephalometric radiographs in orthodontic treatment planning?Am. J. Orthod. Dentofac. Orthop.201113917518110.1016/j.ajodo.2010.09.02121300228 · doi ↗ · pubmed ↗
- 3Dinesh A. Mutalik S. Feldman J. Tadinada A. Value-addition of lateral cephalometric radiographs in orthodontic diagnosis and treatment planning Angle Orthod.20209066567110.2319/062319-425.133378477 PMC 8032255 · doi ↗ · pubmed ↗
- 4Durão A.R. Alqerban A. Ferreira A.P. Jacobs R. Influence of lateral cephalometric radiography in orthodontic diagnosis and treatment planning Angle Orthod.20158520621010.2319/011214-41.125191839 PMC 8631877 · doi ↗ · pubmed ↗
- 5Graf C.C. Dritsas K. Ghamri M. Gkantidis N. Reliability of cephalometric superimposition for the assessment of craniofacial changes: A systematic review Eur. J. Orthod.20224447749010.1093/ejo/cjab 08235175333 · doi ↗ · pubmed ↗
- 6Guinot-Barona C. Alonso Pérez-Barquero J. Galán López L. Barmak A.B. Att W. Kois J.C. Revilla-León M. Cephalometric analysis performance discrepancy between orthodontists and an artificial intelligence model using lateral cephalometric radiographs J. Esthet. Restor. Dent.20243655556510.1111/jerd.1315637882509 · doi ↗ · pubmed ↗
- 7KapetanovićA. Oosterkamp B.C.M. Lamberts A.A. Schols J.G.J.H. Orthodontic radiology: Development of a clinical practice guideline Radiol. Med.2021126728210.1007/s 11547-020-01219-632462471 PMC 7870627 · doi ↗ · pubmed ↗
- 8Ghazali L. Mohd Yusof M.Y.P. Norman N.H. Effects of scanning parameters reduction in dental radiographs on image quality and diagnostic performance: A randomised controlled trial J. Orthod.20214851210.1177/146531252097164133200660 · doi ↗ · pubmed ↗