The Effect of Human Papillomavirus Infection on Pregnancy Outcomes: A Scoping Review
Borek Sehnal, Jan Zapletal, Martin Hruda, Vit Drochytek, Katerina Maxova, Michael J. Halaska, Lukas Rob, Ruth Tachezy

TL;DR
This review explores how HPV infection during pregnancy may be linked to preterm birth and other complications, but more research is needed to confirm cause and effect.
Contribution
The study systematically reviews the association between HPV infection and adverse pregnancy outcomes using molecular confirmation methods.
Findings
HPV infection is linked to increased risk of preterm premature rupture of membranes and preterm birth.
HPV presence in placental tissue may contribute to adverse pregnancy outcomes.
Evidence for HPV's role in preeclampsia and fetal growth restriction remains inconclusive due to limited and varied studies.
Abstract
Background: Human papillomavirus (HPV) is the most common sexually transmitted viral infection worldwide. Moreover, the prevalence of HPV infection is twice as high in pregnant women as in non-pregnant individuals. The aim of this review was to examine adverse pregnancy outcomes associated with cervicovaginal or placental HPV infection confirmed by a sensitive molecular method. Methods: We conducted searches on major medical databases including PubMed, EMBASE, Global Health, and the Cochrane Library to identify all studies examining HPV infection during pregnancy. Additionally, other online sources were consulted for relevant studies. Thirty-four records out of the initial 1868 identified were included in this review for thematic synthesis. The PRISMA-ScR guidelines were followed. Results: This scoping review included a total of 28 original observational studies, 1 systematic review,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
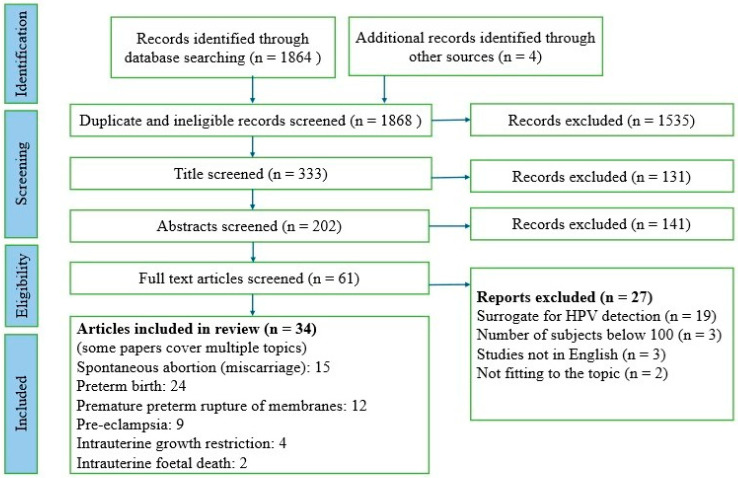 Figure 1
Figure 1- —European Union—Next Generation EU
- —Ministry of Health of the Czech Republic
- —Third Faculty of medicine, Charles University, Prague
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Women's cancer prevention and management · Reproductive tract infections research
1. Introduction
The human papillomavirus (HPV) is a group of viruses that 75–80% of sexually active individuals are infected with at least once during their lifetime. It is therefore the most common sexually transmitted viral infection worldwide [1]. HPV viruses infect the skin and mucous membranes of the anogenital and orofacial areas. Infection is often asymptomatic and resolves spontaneously over time. However, in a small percentage of infected individuals, the virus persists with an increased risk of tumour transformation of the infected tissue. The DNA of some genotypes integrates into the genome of the host infected cell with subsequent increased activation of expression of viral oncogenes E6 and E7, which can lead to malignant transformation of the cell. However, there are other mechanisms by which HPV without integration into the host genome increases the risk of malignancy. Based on the ability of each genotype to initiate carcinogenesis, HPV is divided into high-risk (HR) and low-risk (LR) [2]. HPV is the most common infectious cause of malignancy [1,3]. According to the International Agency for Research on Cancer (IARC), 13 genotypes are currently classified as HR HPV, with HPV genotypes 16, 18, 31, 33 and 45 considered the most important for the development of human malignancies [2]. The total number of HPV-related cancers has been estimated to account for approximately 4.5% of all human cancers worldwide each year, including 8.6% in women and 0.8% in men [4].
Although the greatest risk of HPV infection lies in the initiation of benign and malignant tumours, HPV infection can also adversely affect the course of pregnancy. Most published studies have found a higher prevalence of HPV infection in pregnant women compared to non-pregnant women. A recent 2023 meta-analysis of 144 studies reported a global prevalence of HPV in pregnancy of up to 30.4% (95% CI: 26.9–34.0) in the cervix and vagina, 17.8% (95% CI: 9.8–27.5) in the placenta, 32.1% (95% CI: 25.1–39.7) in serum, 2.3% (95% CI: 0.1–8.1) in amniotic fluid, and 25.5% (95% CI: 23.3–27.8) in urine and the urinary tract. The highest prevalence was observed in populations in Africa and the lowest in Europe and the Eastern Mediterranean [5]. The exact consequences and implications of HPV infection in pregnant women have not yet been studied in detail, but there is evidence for mechanisms of adverse effects of HPV infection in pregnancy. The aim of this scoping review article is to summarize current knowledge of the impact of active HPV infection on pregnant women and unborn children.
2. Materials and Methods
2.1. Design
A scoping review framework was selected to guide decision-making by identifying and analyzing the literature on a specific topic [6]. This review adhered to the following steps: identifying the research question, locating relevant studies, selecting studies, charting the data, summarizing and reporting the findings, and consulting with knowledge users [7]. Ethical approval was not required since this review methodology did not involve experimental research or human participants.
2.2. Population of Interest
We included studies investigating adverse pregnancy outcomes in women with and without HPV infection in various genital sites (vulva, vagina, cervix), placenta, or other products of conception. HPV status was required to be determined using a sensitive molecular method, namely PCR (polymerase chain reaction) or HCA (hybrid capture assay). Studies reporting both general HPV infections and type-specific infections were included.
Two main research questions guided the scoping review:
- Is there a significant association between HPV infection, as detected by PCR or HCA in the lower genital tract or trophoblastic tissue (placenta), and adverse pregnancy outcomes?
- Can we estimate the effect of HPV infection on the risk of miscarriage (spontaneous abortion), preterm birth, premature preterm rupture of membranes (PPROM), preeclampsia, fetal growth restriction (FGR), and intrauterine fetal death?
Additionally, we aimed to determine the strength of the association between cervicovaginal or urinary HPV infection and the presence of HPV infection in trophoblasts.
2.3. Search Strategy
The following databases were searched to identify all suitable studies: Medline PubMed, EMBASE, Global Health, and the Cochrane Library (Table 1, Search strategy). A sensitive literature search strategy was developed to locate published peer-reviewed literature, with search terms combined using Boolean operators. The terms used in various combinations included the following: (“human papillomavirus” OR “HPV”) AND (“pregnancy” OR “miscarriage” OR “spontaneous abortion” OR “pregnancy loss” OR “preterm birth” OR “premature rupture of membranes” OR “PROM” OR “preeclampsia” OR “eclampsia” OR “pregnancy-induced hypertension” OR “PIHD” OR “fetal growth restriction” OR “FGR” OR “intrauterine growth restriction” OR “IURG” OR “small for gestational age” OR “SGA” OR “intrauterine fetal death” OR “stillbirth” OR “adverse birth outcome”). The search was limited to research published in English from 1 January 2000 to 31 August 2025.
We conducted a scoping review following the standard six-stage approach [8] and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and its extension for scoping reviews [9]. We did not use any registered review protocol.
2.4. Types of Studies
We included all types of observational studies: cohort (both retrospective and prospective), case–control, and cross-sectional studies. Additionally, we considered data from systematic reviews and meta-analyses.
2.5. Inclusion and Exclusion Criteria
Full-text evaluation was conducted based on the inclusion and exclusion criteria and the availability of the necessary data to address the main question of this review. Any disagreements were resolved through discussion in an expert-led environment. Due to the specific focus of this review and the publication repertoire in online databases, we did not explicitly search for additional grey literature.
2.6. Data Extraction
Data extraction was initially performed by one reviewer using a predefined data extraction framework, with three authors determining the relevant variables to be collected from the included studies. To ensure accuracy and minimize potential bias, the extracted data were subsequently reviewed and cross-checked by additional members of the research team. Key study characteristics and outcome measures were independently verified, and any discrepancies were resolved through discussion and consensus within the author group. This iterative process was conducted throughout the review to enhance methodological rigour and data reliability (Figure S1, engagement strategy framework). Information extracted from each study included publication characteristics, study design parameters, and pregnancy outcomes among HPV-positive individuals, following the PRISMA Extension for Scoping Reviews (ScR) 2020 guidelines [9].
3. Results
A total of 1864 titles from the main databases and 4 titles from other databases were identified and verified (Figure 1, PRISMA 2020 flowchart representing the study selection process) [10]. Out of these, 1535 articles were either duplicates or ineligible for other reasons and were excluded. Another 131 articles were excluded after screening titles, and 141 studies were excluded after reviewing abstracts for not fitting our topic and inclusion criteria. No additional articles were found during the reference list screening.
Finally, 61 articles were screened by reading the full text, resulting in the inclusion of 28 original observational studies [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38], one systematic review [39], and five meta-analyses [40,41,42,43,44]. Review articles published without clear statistical data were not included [45,46,47,48,49,50]. The final search results were exported into the Zotero program. The search strategy and inclusion criteria were verified by three reviewers. The characteristics and results of the included studies are presented in Table 2 (characteristics of included studies), while the summary results of meta-analyses on the effect of HPV on the course of pregnancy are shown in Table 3 (results of published meta-analyses).
3.1. Miscarriage (Spontaneous Abortion)
Miscarriage (spontaneous abortion) and stillbirth are two general terms describing the death of the fetus, but they refer to losses that occur at different times during pregnancy. The various definitions used therefore pose a methodological difficulty when attempting to interpret and accurately compare stillbirth rates and associated risk factors [51]. WHO recommends a weight of 500 g as the cut-off point between miscarriage and stillbirth [52]. More than half of miscarriages are thought to be due to chromosomal abnormalities in the first trimester of pregnancy [53]. Other common causes include maternal or fetal infections.
The scoping review identified 11 studies [12,13,14,15,18,21,23,28,29,31,38], 1 systematic review [39], and 3 meta-analyses [41,43,44]. The outcomes of the individual studies were inconclusive. For example, in his systematic review, Ambühl pointed to a higher prevalence of HPV in women who had spontaneous abortion but without clear evidence of HPV infection as the cause. HPV prevalence in women with spontaneous abortion was statistically significantly different from women with term delivery in the cervix only (24.5% vs. 17.5% p < 0.05) and in the placenta (24.9% vs. 8.3%; p < 0.05) [39]. These results are consistent with those of some earlier studies. Bennani et al. demonstrated HPV infection as a risk factor for spontaneous abortion (aOR 3.76, p = 0.001) [13]. Ticconi et al. detected a lower prevalence of HPV DNA on the cervix in patients with recurrent unexplained pregnancy loss (26.5%; 13/49) compared to women who had delivered at least one fetus at term and no history of miscarriage (61.9%; 294/475; p < 0.001). The authors hypothesized that the increased immune response of the body potentially responsible for recurrent spontaneous abortion is also a protective factor against HPV infection [31]. Similarly, Bober et al. observed a statistically significant higher prevalence of HPV infection in cervical smears and trophoblasts in women with abnormal first trimester pregnancy [14]. HPV was detected in 17.9% (15/84) of patients in the study group and in 6.8% (4/59) of patients in the control group.
Similarly, HR HPV infection was significantly more common in patients with abnormal first-trimester pregnancy (15.5% vs. 5.1%; p = 0.03). Moreover, HR HPV trophoblast infection was found only in patients in the study group (9.5% vs. 0.0%; p = 0.02) [14]. While these three studies [13,14,31] and a systematic review [39] documented HPV infection as a significant risk factor for miscarriage, the other seven studies [12,15,18,21,23,28,29] indicated a potential risk of HPV infection but without statistical significance (Table 2, characteristics of included studies). A study of 281 women in Mexico found a prevalence of cervical HPV infection in 24.4% of women with first-trimester spontaneous abortion and 15.2% of controls, with HPV 16 and HPV 58 genotypes being the most detected in both groups. Anamnestically, 27.3% of HPV-positive and 17.4% of HPV-negative women reported at least one previous pregnancy loss; however, HPV was not statistically significantly associated with a single or recurrent spontaneous abortion. A history of spontaneous abortion was significantly more frequently associated with age over 35 years, alcohol consumption and multiple sexual partners [18]. In a study from Poland, HPV DNA was detected in chorionic tissue in 17.7% (9/51) of women with spontaneous abortion between 6 and 16 weeks of pregnancy and in 24.4% (19/78) of placentas of women who delivered at term (p = 0.366). The prevalence of HPV 16/18 detection was not statistically different between the cohorts (11.8% vs. 12.8%; p = 0.859) [29].
The 2018 meta-analysis included 12 studies on a total of 3007 patients with different outcomes. Five cohort and three case–control studies found a higher risk of spontaneous abortion associated with HPV infection (OR 1.40; 95% CI: 0.56–3.50), with the cohort studies having a higher risk (OR 1.47; 95% CI: 0.86–2.50) than the case–control studies (OR 1.02; 95% CI: 0.21–5.02). However, the presence of HR HPV infection alone (four studies) did not support an increased risk of miscarriage (OR 0.65; 95% CI: 0.21–1.98). Conversely, the other four studies calculated more than twice the odds of spontaneous miscarriage when any HPV infection was detected (OR 2.24; 95% CI: 1.37–3.65) [43].
The evidence regarding the association between HPV infection and miscarriage remains inconsistent, and the observed findings appear to be largely influenced by methodological differences across individual studies. While some investigations have demonstrated a statistically significant increased risk of spontaneous abortion among HPV-positive women, others have found no association. Variability in the published results is largely attributable to differences in study design, sample size, and, importantly, the anatomical site of HPV detection. Some studies assessed cervical HPV infection, whereas others examined trophoblastic or placental tissue. Cervical HPV detection may reflect transient mucosal colonization rather than direct placental involvement; thus, studies relying exclusively on cervical samples may either overestimate or underestimate the biological relevance of HPV infection for early pregnancy loss. In contrast, studies detecting HPV DNA in trophoblastic tissue may better represent a direct mechanistic association, although they are often limited by smaller sample sizes.
Adjustment for potential confounders further contributes to heterogeneity. Maternal age, smoking status, previous obstetric history, sexual behaviour, and coexisting infections are established risk factors for miscarriage. Not all included studies accounted for these variables, which may partially explain the divergent findings.
Meta-analyses have also yielded inconsistent conclusions. Although some suggested increased odds of miscarriage among HPV-positive women, statistically significant associations were not consistently demonstrated.
Taken together, the current body of evidence does not allow for a definitive conclusion regarding a causal role of HPV infection in miscarriage. The observed discrepancies likely reflect methodological heterogeneity rather than a true biological contradiction. Because spontaneous abortion is the most common adverse outcome of pregnancy, it is important to further study the issue of HPV infection as a causative agent in more detail to reach more definitive conclusions [46,47,48,49].
3.2. Preterm Birth and Premature Preterm Rupture of Membranes (PPROM)
Preterm birth is defined as a birth that occurs before 37 completed gestational weeks (less than 259 days) of gestation. The number of preterm births has been steadily increasing worldwide over the past two decades. Prematurity is associated with a considerable risk of morbidity and mortality, particularly among extremely preterm infants (i.e., <28 weeks). Worldwide, the incidence of preterm births is estimated to be approximately 10% (range 5% in parts of Europe to 18% in parts of Africa), and approximately 15 million children are born preterm each year (range 12 to 18 million) [54,55]. In the United States, approximately 550,000 preterm infants are born each year, with about 10 percent of all live births born before 37 weeks GA and almost 3 percent born <34 weeks [56].
Preterm birth is the result of the activation of the same mechanisms as term birth, but in the case of preterm birth, their activation is pathological. Often the exact cause of preterm birth cannot be determined; the provoking factor is often an infection of the feto-maternal unit [57,58,59]. Premature rupture of membranes (PROM) is defined as the rupture of the amniotic sac (amnion) before the onset of uterine activity. If spontaneous amniotic fluid outflow occurs before 37 weeks of gestation, it is a premature preterm rupture of the membranes (PPROM); spontaneous amniotic fluid outflow before the onset of regular uterine activity at term is termed a term PROM [60].
A total of 18 studies [11,12,16,17,19,22,23,24,25,26,27,28,30,32,33,34,35,38], one systematic review [39] and five meta-analyses [40,41,42,43,44] met the inclusion criteria for the scoping review regarding preterm birth, and a total of nine studies [16,17,20,22,23,28,33,34,36] and three meta-analyses [41,42,44] were included regarding PPROM (premature preterm rupture of the membranes). Altogether, 10 studies [19,24,25,26,27,30,32,34,35,38] and a systematic review [39] demonstrated a statistically significant effect of HPV infection on the risk of preterm birth and eight studies [11,12,16,17,22,23,28,33] did not, but three of these studies [16,17,28] showed a significant risk of HPV infection for PPROM. Cotton-Caballero et al. found that preterm birth in HPV infection is often due to PPROM [61]. The 2021 HERITAGE cohort study of 899 pregnant women confirmed a nearly 4-fold increased risk of preterm birth (adjusted odds ratio, aOR 3.72; 95% CI: 1.47–9.39) with persistent vaginal HPV infection with 16/18 genotypes. Surprisingly, any vaginal HPV infection did not show a statistically significant effect (aOR 1.39; 95% CI: 0.79–2.46) [27]. The presence of placental HPV 16/18 infection was also significantly more common in women with preterm delivery (aOR 2.92; 95% CI: 1.09–7.81) [27]. Similarly, in a systematic review, Ambühl published a higher detection of HPV in the cervix (47.0% vs. 17.5%) and placenta (50.0% vs. 8.3%; p < 0.0001) in women with preterm birth [39]. McDonnold from the USA reports an almost 2-fold increased risk of preterm delivery before 37 weeks in the presence of cervicovaginal HR HPV infection (OR 1.83; 95% CI: 1.03–3.26) and even a 7-fold increased risk of delivery before 35 weeks (OR 6.85; 95% CI 1.87–25.09) [25]. Mosbah et al. detected HPV placental infection in 18.9% (10/53) of Egyptian women who delivered preterm and 4.0% (2/50) of women who delivered at term (p = 0.019). The authors suggest that HPV infection (and particularly HR genotypes) is a risk factor for preterm birth in the Egyptian population [26]. Several studies have analyzed the effect of HPV infection on PPROM. Cho et al. found that 27.3% of women with PPROM had cervical HR HPV infection, whereas in the HR HPV-negative group, PPROM was seen in only 14.2% of women (p = 0.029). The authors conclude that the presence of HR HPV infection is a significant risk factor for PPROM [17]. In a relatively small sample, Pandey found HPV positivity in the vagina in 14.6% of women with PPROM compared to 3.2% in the control group (p = 0.026) [28]. In another retrospective study of 2153 women, the presence of HPV infection approximately doubled the risk of PPROM (OR 2.07, 95% CI: 1.03–4.14) [61].
However, other studies have not produced such convincing results. Data from the Scottish registry (386 women with preterm delivery and 4942 women with term delivery) showed only a risk of preterm delivery in women with a history of surgically treated cervical precancer (OR 1.84; 95% CI 1.10–3.08, p = 0.020) and not with proven cervical HR HPV infection [11]. A prospective multicentre cohort study also found similar results.
HPV infection during pregnancy was not significantly associated with increased risk for the risk of spontaneous preterm birth (aOR 2.26; CI95%: 0.79–6.50, p = 0.13) and for PPROM (aOR 0.62; CI95%: 0.07–5.59, p = 0.67) [33].
However, meta-analyses (Table 3, results of published meta-analyses) and large cohort studies [34,36,38] have demonstrated quite convincingly the negative impact of HPV infection on the risk of PPROM and preterm birth. A 2014 meta-analysis of eight studies calculated the risk of preterm birth to be approximately twice as high in HPV-positive pregnant women compared to HPV-negative women (OR 2.12; 95% CI: 1.51–2.98; p < 0.001) [40]. Another 2018 meta-analysis (four studies, 1408 pregnant women) defined HR HPV infection as a risk factor for preterm birth (OR 2.84; 95% CI: 1.95–4.14), which was confirmed by a sub-analysis of three cohort studies (1348 pregnant women), albeit with a slightly lower risk (RR 2.37; 95% CI: 1.68–3.35) [43]. In a meta-analysis of 36 studies, Niyibizi and colleagues calculated the presence of HPV infection as a risk factor for preterm birth (aOR 1.50; 95% CI: 1.19–1.88), PPROM (aOR 1.96; 95% CI: 1.11–3.45) and TPROM (term premature rupture of membranes before the onset of uterine activity, aOR 1.42; 95% CI: 1.08–1.86) [41]. Similarly, according to a 2021 meta-analysis, HPV infection is a significant risk factor for preterm birth (OR 1.81; 95% CI: 1.25–2.62; p = 0.002) and also for PPROM (OR 1.74; 95% CI: 1.45–2.10; p < 0.00001), although, according to the authors, the reliability of the results may have been affected by the different designs in the individual studies [42]. And the most recent meta-analysis identified HPV infection also as a statistically significant risk factor for preterm birth (OR = 1.94; 95% CI: 1.31–2.87; p = 0.005) [44]. A large retrospective analysis of 400,583 nulliparous women from the Swedish population-based registry was published in 2021 [34]. The presence of HPV infection (detected by PCR or cervical cytology) was defined as a risk factor for preterm birth (aOR 1.19; 95% CI: 1.01–1.42; p = 0.042), PPROM (aOR 1.52; 95% CI: 1.18–1.96; p < 0.001) and TPROM (aOR 1.24; 95% CI: 1.08–1.42; p = 0.002), as well as for neonatal mortality (aOR 2.69; 95% CI: 1.25–5.78; p = 0.011). Similar results were also found for women at risk with a history of cervical surgery for precancer; only the risk of preterm delivery was higher in these women (aOR 1.85; 95% CI: 1.76–1.95; p < 0.001) [34].
3.3. Preeclampsia
Preeclampsia is a pregnancy-specific multi-organ disease of unclear etiology that is conditioned by abnormal placentation and endothelial dysfunction and is accompanied by a systemic inflammatory response. Only the presence of the placenta is required for the development of the disease without the presence of the fetus; it is, in a narrower sense, a vasculopathy with insufficient trophoblast invasion of the decidua with subsequent development of placental ischemia. The prevalence is around 4.5% of pregnant women worldwide [62,63]. The etiology of preeclampsia is multifactorial, and many risk factors have been defined [64]. Some studies point to inflammation as a trigger of endothelial dysfunction [65]. It is speculated that viral and bacterial infections, e.g., cytomegalovirus, Chlamydia pneumoniae, Helicobacter pylori and potentially human papillomavirus, may play a role in the etiopathogenesis of preeclampsia [18,47,66,67].
The scoping review included eight studies [17,19,22,23,25,28,30,37] and one meta-analysis [41]. Only two studies observed a significant effect of HPV infection on the risk of preeclampsia [25,30]. A retrospective study of 942 pregnant women concluded that HR HPV cervical infection doubles the risk of preeclampsia (10.2% vs. 4.9%; p = 0.004; aOR 2.18; 95% CI: 1.31–3.65) [25]. Slatter et al. found by analysis of HR HPV detection from a total of 339 placentas that the presence of HR HPV infection was significantly higher in parturients with preeclampsia, preterm delivery and delivery of a hypotrophic fetus (always p < 0.05) [30]. Another small study from New Zealand found a high 81% expression of E6/E7 HR HPV RNA (an indicator of active viral infection) in placentas of women with preeclampsia positive for HR HPV DNA, in contrast to 13% E6/E7 HR HPV RNA expression in placentas of women without preeclampsia (p = 0.0006) The authors speculate that HPV is active in the trophoblast in these women from early in placental development in the first trimester, when placental quality is determined, and thus HPV infection contributes to the increased risk of developing preeclampsia [68]. However, none of the other studies (Table 2, characteristics of included studies) included in the review nor the meta-analysis (Table 3, results of published meta-analyses) showed an effect of HPV infection on the risk of preeclampsia. Current knowledge does not allow us to establish HPV infection as a risk factor for preeclampsia or other hypertensive disorders induced by pregnancy.
3.4. Fetal Growth Restriction
Fetal growth restriction (FGR), formerly called intrauterine growth restriction (IUGR), is a condition in which the fetus grows slowly due to a pathological process and is unable to reach its genetically determined size. Retrospective data show that 5–10% of all pregnancies are affected by pathologically abnormal fetal growth [69,70,71]. The causes can be diverse; most often FGR develops as a result of placental pathology, e.g., in preeclampsia. Compared to normal-growing individuals, babies with FGR have a 10 times higher risk of perinatal mortality. There is no causal treatment; we try to eliminate risk factors and correct timing of delivery. The infectious etiology in the development of FGR is established for infections of the TORCH group (toxoplasma gondii, rubella, cytomegalovirus, herpes simplex viruses type 1 and 2) [72,73,74,75,76]. Some studies have also found an increased risk of FGR in association with infection with varicella-zoster virus, Treponema pallidum, Plasmodium falciparum, parvovirus B19 and also HPV [47,66,74,77,78].
Only six studies [22,23,28,36,37,38] and one meta-analysis [41] met the inclusion criteria for the scoping review. Kaur et al. analyzed the results of self-reported HPV infection from the Pregnancy Risk Monitoring System from 2004 to 2011 (26,085 subjects). HPV infection was significantly associated with low birth weight (OR: 1.94, 95% CI: 1.14–3.30), but not with preterm birth, PPROM, and preeclampsia [22]. Pandey et al. did not demonstrate the effect of HPV infection on FGR on 104 pregnant women with vaginal HPV test performed in the first trimester (4.8% vs. 4.7%, p = 0.100) [28]. The retrospective observational cohort study on 6285 pregnant women from Beijing did not observe HR HPV infection as a risk factor for FGR (1.8% for HR-HPV positive, 0.6% for HPV negative, p = 0.615) [23]. Slatter et al. collected HPV from the decidua of 339 women. HPV was more frequently detected in pregnant women with acute chorioamnionitis, FGR, and preterm delivery. A total of 76.4% (55/72) of decidua HPV-positive infants had a weight below the 5th percentile [30]. Retrospective study based on abnormal cervical cytology smear detected a 90% (95% CI: 40–150%) higher risk of giving birth to a baby weighing below the third percentile. However, this risk was only 50% (95% CI: 10–100%) when other risk factors (maternal age, ethnicity, social status, occupation, smoking, comorbidities) were eliminated [79].
HPV exposure was associated with FGR in the meta-analysis of seven studies (aOR, 1.17; 95% CI:1.01–1.37; I^2^ = 0%). Moreover, HPV exposure was also significantly associated with low birth weight (aOR 1.91; 95% CI:1.33–2.76, 4 studies, I^2^ = 13%) [41].
3.5. Intrauterine Fetal Death
The International Classification of Diseases defines stillbirths or intrauterine fetal death (IUFD) as the death of a fetus that has reached a birth weight of 500 g, or if birth weight is unavailable, gestational age of 22 weeks or crown-to-heel length of 25 cm [51]. On the other side, WHO recommends using the higher limit (1000 g/28 weeks/35 cm) of third-trimester stillbirths for international comparisons and reporting [51,80]. The legal requirements for registration of fetal deaths vary between and even within countries. For example, The American College of Obstetricians and Gynecologists (ACOG) in the USA defines fetal deaths as delivery of fetus with no signs of life whose birth weight is of 350 g or more, or if weight is unknown, of 20 completed weeks gestation or more. In Australia, stillbirth is also defined as fetal death (no signs of life), whether antepartum or intrapartum, at ≥20 weeks of gestation or ≥400 g birthweight if gestational age is unknown. The United Kingdom defines stillbirth as fetal death at 24 or more completed weeks of gestation [51]. The reported incidence of stillbirth varies significantly between studies from different countries and depending on the definitions used but generally ranges from 3.1 to 6.2/1000 births or 1 in 160 deliveries [51,80,81].
The causes may be on the side of the mother, the fetus or the function of the fetoplacental unit. While the etiology remains unknown in about a quarter of cases, one prospective study revealed that nearly two-thirds of cases are attributable to placental dysfunction [51,81]. Infections of the amniotic fluid are responsible for 2–15% of IUFDs (formerly predominantly caused by lues or variola, nowadays mainly by group B streptococci, anaerobic fusobacteria and Listeria monocytogenes, but also by some viruses) [82,83].
There are not many papers studying the association between IUFD and HPV infection, also because the diagnosis of IUFD is rare. Only one study [34] and one meta-analysis [41] met the inclusion criteria for this scoping review. The large retrospective population-based Swedish Medical Birth Register study included 1,044,023 women with singleton deliveries from 1999 to 2016. Compared to the reference group with an intrauterine fetal death of 0.2%, the risk of intrauterine fetal death in the group with HPV positivity detected by cytology was increased to 0.4% (aOR 1.55, 95% CI 1.13–2.12, p = 0.006) [34]. Niyibizi et al. included in his meta-analysis only two studies [30,84] meeting the criteria and calculated approximately twice the odds of intrauterine fetal death with proven HPV infection (aOR 2.23; 95% CI: 1.14–4.37, I^2^ = 0.0%) [41].
Slatter et al. observed a potential association between placental HPV infection and intrauterine fetal death. In their study, they declared that 81.2% (13/16) of fetal deaths were diagnosed in placental HPV-positive mothers with no other alteration in health status. They correlated placental HPV infection with a higher risk of fetal deaths similar to other infectious villitis [30]. Subramaniam found that 3.7% (9/242) of pregnant women with a diagnosis of IUFD had abnormal cancer screening results (abnormal cytology or HPV positivity), and only 1.4% (29/2079) had normal results (an assumption of HPV negativity) (aOR 2.6; 95% CI: 1.2–5.8; p = 0.01). Because monitoring the frequency of IUFD was not the primary objective of the study, the authors could not definitively establish a firm conclusion regarding this association [84].
4. Discussion
Certain infectious pathogens have been repeatedly shown to have a negative effect on pregnancy with severe damage to the newborn. While a causal association between preterm birth and active infection with certain microorganisms (Ureaplasma urealyticum, Mycoplasma hominis, Fusobacterium spp. and Streptococcus agalactiae) has been repeatedly confirmed [85,86], evidence for a trigger mechanism for viral infections in preterm birth is limited. One of the reasons is the limited ability to detect specific markers of viral infections [53]. Intrauterine infection activates the immune system, cytokines are secreted and, subsequently, prostaglandins are synthesized, which cause uterine contractions. HPV infection of the vagina or cervix may trigger an inflammatory immune response by altering the vaginal microflora, thereby potentially inducing preterm labour. HPV also infects rapidly replicating trophoblasts and, due to distress of the fetoplacental unit, the tendency to preterm labour is greatly enhanced [46,47,48,49].
HPV disrupts cell cycle regulation, inhibits placental trophoblast growth, reduces their viability and induces cell death [47,87,88]. Human trophoblasts are permissive for HPV, and they have receptors for HPV; thus, they facilitate virus entry into the cell and virus replication [12,30,47]. In vitro studies have shown that the complete HPV life cycle can take place in the trophoblast cell [47]. You et al. also showed that active HPV infection, in addition to reducing the number of trophoblasts, also reduces their ability to adhere to decidua cells [89]. Boulenouar et al. evaluated the response of trophoblastic BeWo cell lines to viral oncogenes E5, E6 and E7 of HPV 16 genotype and observed a significantly reduced growth and adhesion capacity of these cells [90]. This is probably due to the ability of oncoproteins E5, E6 and E7 to inhibit the expression of E-cadherin, a molecule essential for cell adhesion. Expression of viral oncoprotein E5 probably creates hydrophilic pores in cell membranes, leading to osmosis and thus rapid cell death (apoptosis) [47,90]. The influence of viral oncoproteins E6 and E7 results in weakened endometrial cell attachment with embryo expulsion [12,30,88,90]. HPV selectively infects villous trophoblasts and thereby induces spontaneous abortion. Disrupted invasion of extravillous trophoblasts in turn leads to placental dysfunction and preterm birth [12,68,88].
Most studies on pregnant women have studied HPV infection in the cervix [91], but HPV infection has also been detected in placenta, amniotic fluid, cord blood, and also in saliva or other oral secretions of newborns and on the surface of fetal membranes, confirming the possibility of vertical transmission of HPV from mother to unborn fetus [46,47,49,92,93,94]. HPV infection of villous and extravillous trophoblasts is likely a contributing factor to adverse pregnancy outcomes. There appears to be a strong correlation between cervicovaginal or urinary HPV infection and placental HPV infection in pregnant women. In one study, 33% (69/207) of women with placental HPV had a positive HPV smear result before pregnancy, compared to 9.4% (8/85) of women with HPV-negative placentae (p = 0.0001) [30]. Ambühl et al. observed that only a history of any HPV disease (p = 0.032) and cervical cancer history (p < 0.001) significantly impacted the presence of placental HPV infection, as opposed to other sociodemographic and clinically relevant parameters [12]. The risk of HPV-positive chorionic villi was found to be four times higher (RR 4.4, 95% CI: 1.6–12.1, p = 0.0018) among women with HPV-positive cervical smears who experienced miscarriages compared to those with HPV cervical negativity [15]. A recent study found that midgestational high-risk HPV in urine was significantly associated with placental HPV infection compared to women without high-risk HPV (aOR 13.1, 95% CI: 3.53–73.21; p < 0.001) [32]. However, despite a high HPV prevalence in urine samples (40%) among pregnant women and the persistence of infections through to delivery in 52% of them, no significant associations were observed with the investigated pregnancy outcomes [37]. Nevertheless, it is important to note that not all published studies on the potential risk of HPV infection on the course of pregnancy and fetoplacental unit function report the same results. However, individual studies differ significantly in methodology, parameters and size of the study population. For example, when calculating the risk of intrauterine fetal death from a large cohort of 400,583 primiparous women, the authors reached different results when HPV infection from the cervix was diagnosed by cytology (aOR 1.55; 95% CI: 1.13–2.12, p = 0.006) or by PCR (aOR 0.93; 95% CI: 0.41–2.09, p = 0.86) [34]. Therefore, a definitive conclusion cannot be drawn based on individual studies, but the results of meta-analyses support HPV infection as a risk factor for preterm amniotic fluid leakage and preterm birth (Table 2).
Given the high population prevalence of HPV infection, it is reasonable to assume that HPV vaccination should also improve perinatal outcomes. This assumption is supported, for example, by the findings of a meta-analysis of six studies with 11,869 subjects, which found more than double the risk of female sterility in the presence of HR HPV infection alone (OR 2.33; 95% CI: 1.42–3.83, p = 0.0008) [95]. A thorough analysis of health registries from Australia from 2000 to 2015 (a routine vaccination started in Australia in 2007) revealed modest improvements in some perinatal outcomes for mothers who were vaccinated against HPV at a young age. The authors observed a modest decrease in the rate of preterm birth by 3.2% (95% CI: 1.1–5.3) and fewer hypotrophic babies by 9.8% (95% CI: 8.2–11.4) among those vaccinated (after adjusting for other risk factors) [96]. Also, a Finnish study analyzing 20,513 births from a national registry (Finnish Population Register Centre) found that the rate of preterm births was significantly lower in the group of primigravidae previously vaccinated against HPV [97]. Preterm delivery before 37 weeks of gestation was observed in 13/409 (3.2%) primigravidae vaccinated with bivalent HPV vaccine and in 98/1923 (5.1%) primigravidae who did not receive HPV vaccine (OR 0.61, 95% CI: 0.34–1.09). Very preterm delivery before 32 weeks of gestation was not observed in any primigravida vaccinated against HPV (0/409) and in 1.0% (20/1923) primigravidas not vaccinated against HPV (p = 0.04) [97].
A major challenge in interpreting the available evidence is the substantial methodological heterogeneity among the included studies. This heterogeneity arises from several key sources. First, HPV detection methods differed considerably. While most studies used PCR-based techniques, others relied on hybrid capture assays or cytology-based classification as a surrogate for HPV infection. The diagnostic sensitivity and specificity of these methods vary, potentially leading to misclassification bias and inconsistent prevalence estimates. Second, the anatomical site of HPV detection was not uniform across studies. HPV was assessed in cervical samples, placental tissue, trophoblasts, urine, and occasionally other biological materials. Given that placental infection may represent a different biological process than transient cervicovaginal colonization, these differences may partly explain discrepancies in reported associations with adverse pregnancy outcomes. Third, not all studies differentiated between low-risk and high-risk HPV genotypes, and only a subset performed genotype-specific analyses (e.g., HPV 16/18). Since oncogenic genotypes may have different biological effects on trophoblastic function, inconsistent genotype stratification further complicates direct comparison between studies. Fourth, the timing of HPV testing during pregnancy varied substantially, ranging from the first trimester to mid-gestation or delivery. Considering that HPV infection may be transient or persistent, differences in sampling time may influence both detection rates and the observed association with pregnancy outcomes. This methodological heterogeneity was most evident in the interpretation of findings concerning the association between HPV infection and miscarriage. One important source of variability was study design. Case–control studies and smaller cohort studies more frequently reported statistically significant associations, whereas larger population-based cohorts often demonstrated weaker or non-significant effects. Smaller studies may be more susceptible to random variation and selection bias, particularly when miscarriage cases are recruited from specialized clinical settings.
Finally, definitions of adverse pregnancy outcomes (e.g., miscarriage, preterm birth, intrauterine fetal death, fetal growth restriction) were not uniform across studies and sometimes followed different national or institutional criteria. Such variability limits the ability to synthesize results and may contribute to the conflicting findings reported in the literature. Taken together, these methodological inconsistencies reduce the comparability of individual studies and must be considered when interpreting the overall body of evidence.
It is also important to emphasize that the evidence summarized in this review is derived predominantly from observational studies. While several associations between HPV infection and adverse pregnancy outcomes have been reported, observational study designs do not permit definitive causal inference. Therefore, the findings should be interpreted as indicative of potential associations rather than proof of causality. Future research should aim to implement standardized HPV detection protocols, consistent genotype stratification, clearly defined pregnancy outcomes, and uniform timing of assessment in order to enhance interpretability and enable more robust synthesis of findings. Furthermore, establishing a causal relationship would require well-designed prospective studies with standardized exposure assessment and adequate control of potential confounding factors. Our scoping review has some limitations. The studies included in this review were heterogeneous in design, and their results cannot be directly interpreted collectively. Some studies combined women with HPV infection confirmed by PCR or hybrid capture assay with those classified as HPV-positive based on cytology results or clinical manifestations used as surrogate markers. Several studies showed already lower adverse pregnancy outcomes in women vaccinated against HPV infection before their sexual debut. Another limitation of this scoping review is that the study protocol was not prospectively registered (e.g., in PROSPERO). Prior registration would have further enhanced transparency and minimized the potential risk of reporting bias. Nevertheless, this review was conducted in accordance with the PRISMA-ScR guidelines, and the methodology was established before the initiation of data extraction. Therefore, this scoping review provides a comprehensive summary of the current knowledge on the investigated topic.
5. Conclusions
The adverse effects of some infections on pregnancy and unborn fetuses are well known. Active human papillomavirus infection during pregnancy is likely to negatively affect the health of both mother and child and to increase the risk of specific pregnancy complications, particularly premature rupture of membranes and preterm birth. However, definite conclusions regarding the causal association between HPV infection and other potential adverse pregnancy outcomes cannot be established at this time. Prospective well-designed studies that consider the higher prevalence of HPV infection during pregnancy, as well as all possible pregnancy complications and associated risks, will be necessary to draw more definitive and clear conclusions. The recently demonstrated reduction in pregnancy complications among HPV-vaccinated populations, as shown by several studies, suggests that HPV infection may act as a cofactor in certain adverse perinatal events.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Forman D. de Martel C. Lacey C.J. Soerjomataram I. Lortet-Tieulent J. Bruni L. Vignat J. Ferlay J. Bray F. Plummer M. Global burden of human papillomavirus and related diseases Vaccine 201230 F 12F 2310.1016/j.vaccine.2012.07.05523199955 · doi ↗ · pubmed ↗
- 2Bouvard V. Baan R. Straif K. Grosse Y. Secretan B. El Ghissassi F. Benbrahim-Tallaa L. Guha N. Freeman C. Galichet L. A review of human carcinogens—Part B: Biological agents Lancet Oncol.20091032132210.1016/S 1470-2045(09)70096-819350698 · doi ↗ · pubmed ↗
- 3DyrhonováM. Chlíbek R. Pandemic of hepatitis C virus infection Epidemiol. Mikrobiol. Imunol.201665727827467323 · pubmed ↗
- 4de Martel C. Georges D. Bray F. Ferlay J. Clifford G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis Lancet Glob. Health 20208 e 180e 19010.1016/S 2214-109X(19)30488-731862245 · doi ↗ · pubmed ↗
- 5Ardekani A. Sepidarkish M. Mollalo A. Afradiasbagharani P. Rouholamin S. Rezaeinejad M. Farid-Mojtahedi M. Mahjour S. Almukhtar M. Nourollahpour Shiadeh M. Worldwide prevalence of human papillomavirus among pregnant women: A systematic review and meta-analysis Rev. Med. Virol.202333 e 237410.1002/rmv.237435678261 · doi ↗ · pubmed ↗
- 6Peters M.D.J. Marnie C. Tricco A.C. Pollock D. Munn Z. Alexander L. Mc Inerney P. Godfrey C.M. Khalil H. Updated methodological guidance for the conduct of scoping reviews JBI Evid. Synth.2020182119212610.11124/JBIES-20-0016733038124 · doi ↗ · pubmed ↗
- 7Levac D. Colquhoun H. O’Brien K.K. Scoping studies: Advancing the methodology Implement. Sci.201056910.1186/1748-5908-5-6920854677 PMC 2954944 · doi ↗ · pubmed ↗
- 8Oravec N. Monnin C. Gregora A. Bjorklund B. Dave M.G. Schultz A.S.H. Chudyk A.M. Protocol for a scoping review to map patient engagement in scoping reviews Res. Involv. Engagem.202282710.1186/s 40900-022-00361-x 35725640 PMC 9210720 · doi ↗ · pubmed ↗