Relationship Between Mitral Annular Calcification and Inflammatory Indices in Patients with Cardiometabolic Risk Factors
Paula Cristina Morariu, Alexandru Florinel Oancea, Maria Mihaela Godun, Diana Elena Floria, Oana Sîrbu, Anca Ouatu, Daniela Maria Tanase, Ionela Daniela Morariu, Cristina Gena Dascălu, Mariana Floria

TL;DR
This study finds that inflammatory markers are not independently linked to mitral annular calcification once cardiometabolic factors are considered, suggesting metabolic issues are more central to its development.
Contribution
The study clarifies that inflammatory indices reflect cardiometabolic context rather than being directly linked to mitral annular calcification.
Findings
Inflammatory markers like CRP and NLR differ between patients with and without MAC in unadjusted comparisons.
After adjusting for cardiometabolic factors, inflammatory markers do not independently associate with MAC.
Age and glucose metabolism abnormalities are the strongest independent predictors of MAC.
Abstract
Background: Mitral annular calcification (MAC) is associated with systemic atherosclerosis and cardiometabolic risk factors. Although hematologic inflammatory indices have been reported to be correlated with MAC, whether these associations persist after accounting for the cardiometabolic context in which MAC occurs remains unclear. Methods: In a prospective, cross-sectional study of consecutive adults, patients with mild MAC were compared to those without MAC. Individuals with major inflammatory conditions, advanced chronic kidney disease, cirrhosis, malignancy, autoimmune/acute inflammatory disorders, significant valvular disease, prosthetic valves/pacing devices, psychiatric disorders, or moderate-severe MAC were excluded. C-reactive protein (CRP) and hematological inflammatory indices, including neutrophil-to-lymphocyte ratio (NLR), Systemic Inflammatory Response Index (SIRI), and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
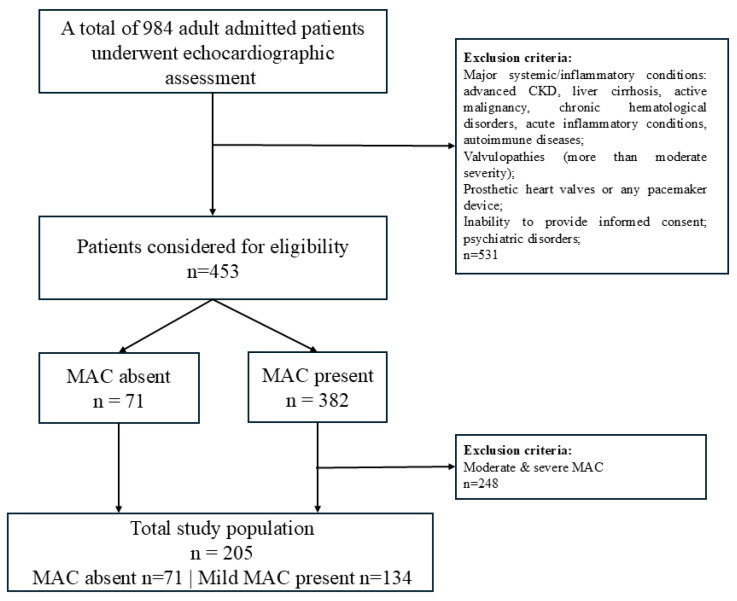 Figure 1
Figure 1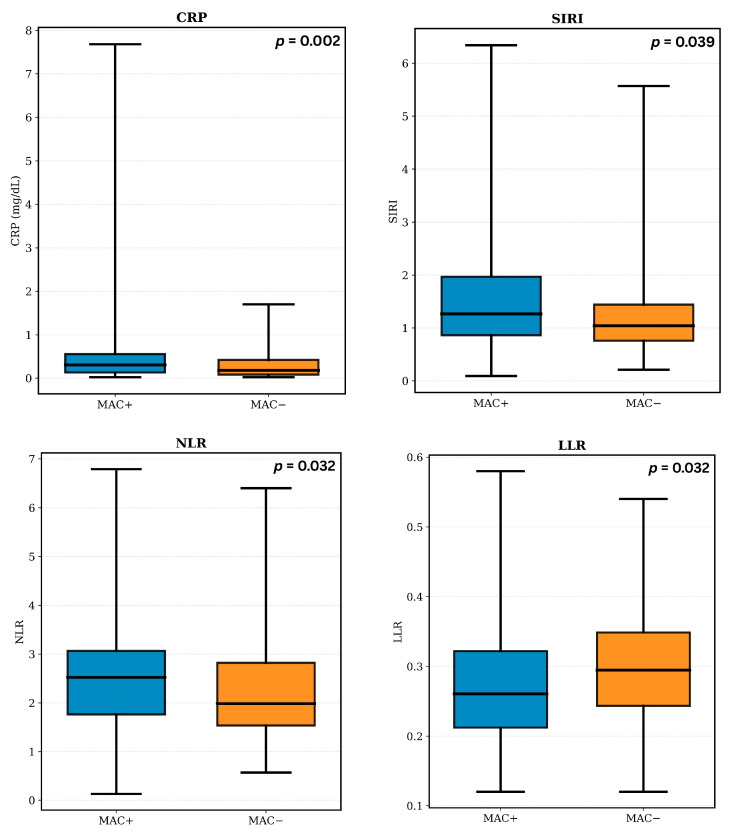 Figure 2
Figure 2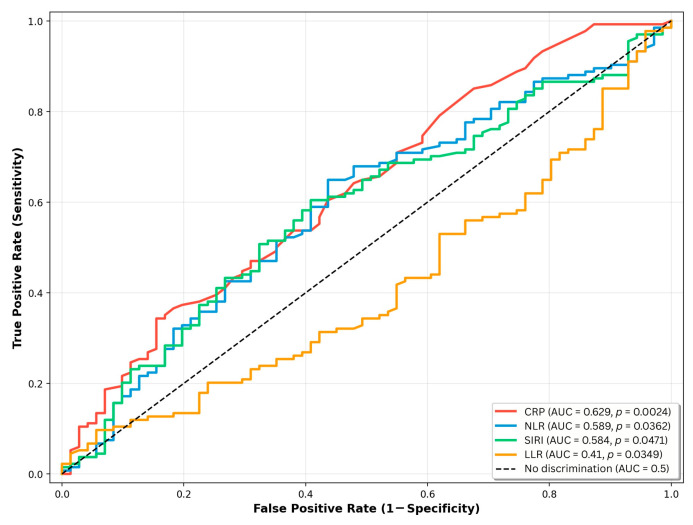 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Cardiac Valve Diseases and Treatments · Inflammatory Biomarkers in Disease Prognosis
1. Introduction
Mitral annular calcification (MAC) is now regarded as a systemic pathological entity rather than a purely localized degenerative alteration [1,2,3]. It shows a strong association with generalized atherosclerotic disease, sharing key cardiovascular risk factors age, obesity, type 2 diabetes (T2D), dyslipidemia, and arterial hypertension. Evidence from pathological and clinical investigations indicates that MAC frequently coexists with carotid, coronary, and aortic atherosclerosis, suggesting the concept that MAC reflects a cardiac manifestation of systemic vascular disease [4,5,6,7,8,9].
Systemic inflammation (SI) represents a central mechanism linking traditional cardiovascular risk factors to atherosclerosis and may also contribute to the development of MAC by promoting leukocyte recruitment, cytokine release, and vascular smooth muscle cell apoptosis, which together facilitate calcium deposition within the fibrous cardiac skeleton [10,11]. Nonetheless, available data remains inconclusive regarding the causal role of inflammation in the development of MAC, the possibility that MAC itself induces a systemic inflammatory response, or whether both phenomena primarily reflect the influence of common cardiometabolic risk factors [12].
In this framework, readily available hematological indices of inflammation, including neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR), have attracted growing interest because of their low cost, ease of assessment, and recognized ability to reflect chronic low-grade systemic inflammation. NLR has been constantly associated with increased cardiovascular morbidity, the presence of arterial calcification, and unfavorable clinical outcomes across diverse patient populations [10,13,14]. Other composite scores like Systemic Inflammation Response Index (SIRI) and the Systemic Immune-Inflammation Index (SII) have been linked to atherosclerosis and cardiometabolic risk. These markers capture low-grade, subclinical SI using routinely available parameters and are increasingly used in cardiovascular research [15,16,17,18].
Although prior studies have reported associations between MAC and inflammatory markers such as NLR and PLR, these findings were largely derived from populations characterized by advanced age and a high burden of cardiometabolic comorbidities, conditions linked to chronic low-grade inflammation [10,19]. Consequently, it remains uncertain whether the reported associations are attributable to inflammatory mechanisms directly related to MAC or merely reflect the inflammatory milieu characteristic of cardiometabolic disease. In this setting, the present study was designed to examine the relationship between MAC and CRP and selected hematological inflammatory indices (including NLR, SIRI, and LLR) among patients with cardiometabolic factors, within the cardiometabolic context in which MAC develops.
2. Materials and Methods
2.1. Study Population and Design
This was a prospective, cross-sectional observational study conducted in the Internal Medicine Clinic of Saint Spiridon County Clinical Emergency Hospital, Iasi, Romania. During the study period (March 2023–August 2024), all consecutive adult patients (≥18 years) attending the clinic for cardiology consultation routinely underwent transthoracic echocardiography as part of standard care, regardless of the underlying diagnosis. From this consecutive series, patients were initially screened for the presence or absence of MAC on two-dimensional echocardiography.
Patients were excluded if they were unable to provide informed consent or if they had hemodynamically significant valvular heart disease (>moderate mitral or aortic regurgitation or stenosis), prosthetic heart valves, temporary or permanent cardiac pacing devices, or a documented psychiatric disorder. To reduce the confounding impact of major SI conditions on hematologic indices and to better characterize low-grade inflammation, individuals with advanced chronic kidney disease (<30 mL/min/1.73 m^2^), liver cirrhosis, active malignancy, chronic hematologic disorders, acute inflammatory conditions, or autoimmune diseases were also excluded. Patients with moderate to severe MAC were not included to ensure a homogeneous study population and avoid the potential hemodynamic consequences of advanced annular calcification on inflammatory markers. Accordingly, the analysis was restricted to patients with mild MAC and those without MAC, allowing a focused evaluation of the relation between early MAC and hematological inflammatory indices in a cardiometabolic risk context.
2.2. Clinical and Laboratory Assessment
Participants underwent a standardized clinical evaluation, including demographic information (age, sex, residential area), cardiovascular history, comorbidities (hypertension, T2D, prediabetes, dyslipidemia, hepatic steatosis, heart failure, atrial fibrillation, prior myocardial infarction, prior stroke), and lifestyle factors (smoking status).
Fasting venous blood samples were obtained from the antecubital vein after a 12 h fast using standard sterile technique. Hematological parameters were measured from EDTA-anticoagulated samples, while biochemical analyses were performed using routine laboratory methods. Renal function was assessed by estimating glomerular filtration rate (eGFR) using the CKD-EPI equation.
Inflammation-related indices were derived from complete blood count parameters, including NLR, PLR, neutrophil-to-monocyte ratio (NMR), and lymphocyte-to-leukocyte ratio (LLR). Two composite indices were also calculated: SIRI, calculated as (neutrophils × monocytes)/lymphocytes, and SII, defined as (neutrophils × platelets)/lymphocytes. These indices were selected due to their availability from routine testing and their established use as markers of low-grade SI in cardiovascular and cardiometabolic research.
Heart failure was defined according to ESC criteria (typical symptoms/signs, elevated natriuretic peptides, and structural or functional cardiac abnormalities) [20]. Both preserved ejection fraction and reduced ejection fraction phenotypes were included. Glucose metabolism status was defined according to contemporary guidelines, with T2D diagnosed by a documented history, fasting plasma glucose ≥ 126 mg/dL, HbA1c ≥ 6.5%, or glucose-lowering treatment. Prediabetes was defined as fasting plasma glucose 100–125 mg/dL and/or HbA1c 5.7–6.4%, in the absence of antidiabetic treatment. Hepatic steatosis was diagnosed by abdominal ultrasonography, based on increased liver echogenicity compared with the renal cortex and vascular blurring.
2.3. Echocardiographic Evaluation and MAC Definition
All patients underwent comprehensive transthoracic echocardiographic evaluation using a Samsung ultrasound system (Samsung Medison, Seoul, Republic of Korea) in accordance with current recommendations. Standard M-mode, two-dimensional, and Doppler imaging techniques were applied. Left ventricular end-systolic and end-diastolic volumes, as well as ejection fraction (LVEF), were calculated using the biplane Simpson’s method from apical four-chamber and apical two-chamber views. Left atrial volumes were assessed according to current echocardiographic recommendations. Valvular regurgitation and stenosis were evaluated using color Doppler imaging, complemented by pulsed- and continuous-wave Doppler recordings.
All examinations were performed by a single experienced operator to minimize interobserver variability, and each measurement was obtained twice in the same view to reduce intraobserver variability.
MAC was defined as a localized, highly echogenic structure at the junction between the atrioventricular groove and the base of the mitral valve leaflets, visualized consistently in the parasternal long-axis, parasternal short-axis, and apical four-chamber views. Only mild MAC was considered for analysis, defined as a focal calcific deposit with maximal thickness < 5 mm, involving less than 1/3 of the annular circumference and confined to the annulus, without extension into the left ventricular inflow tract or onto the leaflets or adjacent myocardium [21]. Calcification thickness was measured from the leading to the trailing edge at the site of greatest echo-density.
2.4. Ethical Considerations
The study protocol was approved by the Ethics Committee of the Saint Spiridon Emergency Clinical Hospital (no. 28/9 March 2023) and by the Ethics Committee of the Grigore T. Popa University of Medicine and Pharmacy, Iasi (no. 303/16 May 2023). All participants provided informed consent prior to enrollment, in accordance with the principles of the Declaration of Helsinki.
2.5. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA). Data distribution was assessed using the Shapiro-Wilk test. Continuous variables are presented as mean ± standard deviation for normally distributed variables and as median with interquartile range (IQR) for non-normally distributed variables. Categorical variables are expressed as frequencies and percentages. Group comparisons between patients with and without MAC were conducted using appropriate parametric and non-parametric tests: the independent samples t-test for normally distributed continuous variables and the Mann-Whitney U test for non-normal variables. Categorical variables were compared using the chi-square (χ^2^) test. Trends toward significance were noted for p-values between 0.05 and 0.10. Receiver operating characteristic (ROC) curve analysis was used to descriptively assess the ability of inflammatory markers to differentiate between patients with and without MAC, with calculation of the area under the curve (AUC) and corresponding 95% confidence intervals (CIs). Correlations between inflammatory markers and selected clinical and cardiometabolic variables were evaluated using Spearman’s rank correlation coefficients. Multivariable binary logistic regression analyses were performed to assess the association between inflammatory markers and MAC after accounting for relevant cardiometabolic and clinic covariates. To avoid multicollinearity between mathematically related inflammatory indices, separate regression models were constructed, each including only one inflammatory marker at a time. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test. All tests were two-sided, and a p-value < 0.05 was considered statistically significant.
3. Results
After applying the inclusion and exclusion criteria, 205 patients were retained for analysis, comprising 134 individuals with mild MAC and 71 individuals without MAC, who formed the MAC and non-MAC groups (Figure 1). The results below summarize clinical and cardiometabolic characteristics, followed by the relationship between MAC and inflammatory indices.
3.1. Baseline Characteristics of the Study Population
Baseline clinical, cardiovascular, cardiometabolic, echocardiographic, and laboratory characteristics stratified by MAC status are summarized in Table 1. Patients with MAC were significantly older than those without MAC (66.5 vs. 58.0 years, p < 0.001) and exhibited a higher systolic BP (149.1 ± 22.3 mmHg vs. 138.1 ± 17.8 mmHg, p < 0.001), as well as a marked prevalence of arterial hypertension (96.3% vs. 69.0%, p < 0.001). Measures of adiposity, including waist circumference (103.0 cm vs. 97.0 cm, p = 0.021) and BMI (30.7 ± 5.5 kg/m^2^ vs. 28.7 ± 5.3 kg/m^2^, p = 0.013) were also significantly greater in the MAC group, while sex distribution and smoking status did not differ between groups (p = 0.203 and p = 0.365, respectively).
From a cardiometabolic perspective, disturbances in glucose metabolism were more frequent among patients with MAC, with a higher prevalence of both prediabetes (54.5% vs. 43.7%, p = 0.004) and T2D (16.4% vs. 5.6%, p = 0.004). Heart failure was substantially more common in the MAC group (91% vs. 53.5%, p < 0.001), whereas the prevalence of coronary artery disease and atrial fibrillation was comparable between groups.
Echocardiographic assessment revealed significant differences in patients with MAC, including increased interventricular septum thickness (p = 0.049), larger left atrial volume (p < 0.001), greater right atrial diameter (p = 0.030), and increased right ventricular basal diameter (p = 0.014). LVEF did not differ between groups, while left ventricular volumes showed only borderline differences.
Laboratory analyses demonstrated higher levels of HbA1c (5.85% vs. 5.60%, p < 0.001), triglycerides (113.5 mg/dL vs. 81.0 mg/dL, p < 0.001), and NT-proBNP (116.0 pg/mL vs. 85.0 pg/mL, p = 0.031) in the MAC group, accompanied by lower HDL-cholesterol concentrations (45.0 mg/dL vs. 53.0 mg/dL, p < 0.001). Renal function, assessed by eGFR, as well as LDL-cholesterol and global hematological parameters, including hemoglobin, total leukocyte count, and platelet count, were similar between groups.
Inflammatory indices (Figure 2) showed modest but statistically significant differences between patients with and without MAC. Patients with MAC exhibited higher NLR (2.52 vs. 1.99, p = 0.032) and SIRI values (1.27 vs. 1.04, p = 0.039) and lower LLR values compared to those without MAC (0.26 vs. 0.29, p = 0.032). In parallel, serum CRP levels were also elevated in the MAC group (0.31 mg/dL vs. 0.18 mg/dL, p = 0.002), whereas NMR, PLR, and SII did not differ significantly between groups.
3.2. ROC Analysis of Hematological Inflammatory Markers
In ROC curve analysis (Figure 3), CRP demonstrated the highest AUC at 0.629 (95% CI: 0.543–0.713), followed by NLR (AUC 0.589; 95% CI: 0.503–0.672) and SIRI (AUC 0.584; 95% CI: 0.500–0.668). In contrast, the LLR displayed an AUC below 0.5 (0.419; 95% CI: 0.330–0.493), consistent with lower values observed in the MAC group.
3.3. Inflammatory Markers in Relation to Clinical and Cardiometabolic Variables
Because inflammatory indices may be influenced by age, adiposity, glucose metabolism, cardiac dysfunction, and renal impairment, we further explored their relationship with selected clinical and biochemical variables.
Correlations between inflammatory markers and selected clinical variables are presented in Table 2. Spearman correlation analysis showed statistically significant associations between age and all four inflammatory markers, including CRP, NLR, LLR, and SIRI. CRP demonstrated significant correlations with BMI, waist circumference, and NT-proBNP levels. NLR was weakly correlated with eGFR, while LLR showed a significant positive correlation with eGFR and a negative correlation with age. SIRI was significantly correlated with age, NT-proBNP, and eGFR.
Given the known influence of glucose metabolism on inflammatory markers, we further examined their distribution according to glycemic status (Table 3). Median values and interquartile ranges of CRP, NLR, LLR, and SIRI are shown for participants without dysglycemia, with prediabetes, and with T2D. Statistically significant differences across glycemic categories were observed for CRP, NLR, and SIRI, whereas LLR showed no significant overall differences between groups.
To assess whether the associations observed in univariable analyses persisted after accounting for relevant clinical and cardiometabolic factors, multivariable logistic regression models were constructed with MAC status as the dependent variable (Table 4, Table 5, Table 6 and Table 7). Each model included a single inflammatory marker (CRP, NLR, LLR, and SIRI) together with clinically relevant covariates selected a priori, including age, measures of adiposity, glucose metabolism status, NT-proBNP levels, and renal function, as applicable.
After multivariable adjustment, none of the inflammatory markers demonstrated a statistically significant association with the presence of MAC. In contrast, age remained significantly associated with MAC in the NLR-, LLR-, and SIRI-based models, with ORs ranging from 1.056 to 1.063 per year increase (all p ≤ 0.001). Abnormalities of glucose metabolism were consistently associated with MAC, with prediabetes showing ORs between 2.43 and 3.63 and T2D showing ORs between 5.91 and 6.19 across applicable models (all p ≤ 0.004). Renal function, expressed as eGFR, was additionally associated with MAC in the NLR- and SIRI-based models (OR 1.03 per 1 mL/min/1.73 m^2^ increase; p = 0.022 and p = 0.029, respectively).
4. Discussion
In this cross-sectional study of patients with cardiometabolic risk factors, several inflammatory biomarkers derived from routine hematological testing (including CRP, NLR, SIRI, and LLR) showed significant differences between patients with and without mild MAC in unadjusted analyses. However, these associations were no longer evident after multivariable adjustment for age, abnormalities of glucose metabolism, and other relevant cardiometabolic covariates. By contrast, age and disturbances in glucose metabolism, particularly prediabetes and T2D, remained robustly and independently associated with the presence of mild MAC.
The observed pattern of results is compatible with at least three interpretations, which our cross-sectional design cannot distinguish. First, inflammatory markers may primarily reflect the cardiometabolic burden (particularly dysglycemia, obesity, and their metabolic consequences) that accompanies MAC, rather than representing MAC-specific inflammatory processes. This interpretation is supported by the consistent associations we observed between inflammatory indices and cardiometabolic variables and by the strong independent associations of MAC with age and glucose metabolism disorders. Second, both MAC and increased levels of inflammatory markers may arise as parallel consequences of shared cardiometabolic derangements, particularly chronic hyperglycemia and insulin resistance, rather than reflecting a direct causal relationship between inflammation and MAC. Third, the absence of independent associations in multivariable models may be explained by limited statistical power to detect small, independent inflammatory effects on MAC after adjustment for strongly correlated cardiometabolic variables. The relatively modest between-group differences in inflammatory markers suggest that any independent contribution of inflammation, if present, is likely minor and would require larger study populations to be reliably identified.
Chronic low-grade inflammation is a well-recognized feature of T2D and the broader cardiometabolic syndrome, conditions that are strongly age-dependent and characterized by sustained exposure to hyperglycemia, excess free fatty acids, and insulin resistance [22,23]. These metabolic disturbances promote inflammatory signaling within the vascular wall and have been consistently linked to both arterial and valvular calcification [23,24]. Experimental and human studies suggest that in this metabolic context, vascular smooth muscle cells undergo phenotypic changes resembling endochondral ossification, with loss of calcification inhibitors and acquisition of osteochondrogenic markers [23,25].
Importantly, accumulating evidence indicates that hyperglycemia may also promote calcific remodeling through local, tissue-level mechanisms, such as advanced glycation end-product accumulation, oxidative stress, and osteogenic signaling [26]. In addition to hyperglycemia, insulin resistance may further contribute to calcific remodeling by attenuating protective metabolic signaling pathways. Under physiological conditions, insulin exerts anti-calcific effects through the regulation of calcification inhibitors; these mechanisms are impaired in insulin-resistant states, favoring osteogenic signaling and phenotypic transformation of the interstitial cells [27]. Such metabolic alterations provide a plausible link between abnormalities of glucose metabolism and valvular calcification that may occur independently of circulating systemic inflammatory markers.
Our results situate MAC within the broader continuum of metabolically driven calcific conditions. The consistent and robust associations between MAC and abnormalities of glucose metabolism—particularly prediabetes and T2D—across all analytical models, together with the attenuation of inflammatory marker associations after multivariable adjustments, support the interpretation that MAC represents a manifestation of chronic metabolic dysfunction, with inflammation reflecting an accompanying feature of the underlying metabolic milieu rather than an independent driver [28].
Our results both confirm and build upon previous observations in the literature. Varol et al. reported an association between NLR and MAC in a small cohort, demonstrating that NLR was significantly elevated in patients with MAC [10]. Yayla et al. reported that PLR was significantly higher in MAC and independently associated with MAC after adjusting for conventional risk factors such as age, hypertension, LDL-cholesterol, and triglycerides [19]. In our study population, inflammatory biomarkers differed between groups in crude analyses; however, these associations were no longer evident after thorough adjustment for cardiometabolic confounders. The divergence from previous reports may be attributed to the strict population selection, restriction to mild MAC, and extensive cardiometabolic adjustment, which together may have attenuated the independent inflammatory signal. Furthermore, the relatively limited sample size may have reduced the ability to detect modest inflammatory effects once full adjustment was performed. Taken together, these factors indicate that the relationship between inflammatory markers and MAC may be complex and may vary according to disease severity, population characteristics, and the extent of underlying cardiometabolic dysfunction.
A strength of this study is its prospective design, with systemic echocardiographic and laboratory assessment of consecutively evaluated patients, allowing consistent characterization of their cardiometabolic profile. Nevertheless, several limitations should be acknowledged. First of all, the cross-sectional, single-center design in a tertiary-care referred population precludes any causal inference regarding the temporal relationship between inflammation and MAC and may introduce potential selection bias, limiting generalizability to broader settings. Whether elevated inflammatory indices precede MAC development or simply reflect the underlying cardiometabolic milieu cannot be determined in this cross-sectional study and requires longitudinal investigation. Second, the strict exclusion criteria and deliberate focus on mild MAC mean that patients with advanced MAC or major inflammatory comorbidities were not represented, so the findings may not apply across the full spectrum of MAC. Third, the unequal distribution of patients with and without MAC, inherent to the consecutive enrollment strategy, may have limited the statistical power to detect modest independent associations after multivariable adjustment. Although propensity score matching could have been considered, its application would have substantially reduced the effective sample size and restricted the analysis to a highly selected subgroup. Given the cross-sectional, observational design, the absence of an assigned exposure or intervention and the study’s focus on association rather than causality, multivariable regression was considered the most appropriate analytical approach.
The loss of significance of inflammatory markers after adjustment highlights the predominant influence of age and impaired glucose metabolism in mild MAC. Although low-grade inflammation may plausibly mediate the link between dysglycemia and MAC, formal mediation analysis was not undertaken due to the cross-sectional study design, which precludes reliable temporal inference. Moreover, the inflammatory indices assessed are indirect hematological surrogates rather than specific molecular mediators, limiting their appropriateness for mediation modeling. Accordingly, the focus of this study was on independent associations rather than causal or mechanistic pathways. Our approach was designed to capture predominantly low-grade, subclinical inflammation using simple hematological indices derived from the routine complete blood count; however, we did not assess cytokines or other molecular inflammatory markers. Therefore, the absence of independent associations should be interpreted in the context of early-stage MAC within a cardiometabolic population.
5. Conclusions
In this cross-sectional study of patients with cardiometabolic risk factors and mild MAC, we found that while inflammatory indices showed unadjusted differences between patients with and without MAC, these associations did not persist after accounting for age and metabolic factors, particularly glucose metabolism abnormalities. These findings are most compatible with inflammatory markers primarily reflecting the cardiometabolic milieu in which MAC occurs. Age and disturbances in glucose metabolism emerged as the dominant factors independently associated with MAC, reinforcing the importance of metabolic dysfunction in MAC pathogenesis. Whether targeted anti-inflammatory strategies beyond optimal metabolic control might prevent or modify MAC development remains an important unanswered question requiring prospective interventional studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abramowitz Y. Jilaihawi H. Chakravarty T. Mack M.J. Makkar R.R. Mitral Annulus Calcification J. Am. Coll. Cardiol.2015661934194110.1016/j.jacc.2015.08.87226493666 · doi ↗ · pubmed ↗
- 2Cavalcanti L.R.P. SáM.P.B.O. PerazzoÁ.M. Escorel Neto A.C. Gomes R.A.F. Weymann A. Zhigalov K. Ruhparwar A. Lima R.C. Mitral Annular Calcification: Association with Atherosclerosis and Clinical Implications Curr. Atheroscler. Rep.202022910.1007/s 11883-020-0825-332034516 · doi ↗ · pubmed ↗
- 3Massera D. Trivieri M.G. Andrews J.P.M. Sartori S. Abgral R. Chapman A.R. Jenkins W.S.A. Vesey A.T. Doris M.K. Pawade T.A. Disease Activity in Mitral Annular Calcification Circ. Cardiovasc. Imaging 201912 e 00851310.1161/CIRCIMAGING.118.00851330712363 PMC 6366554 · doi ↗ · pubmed ↗
- 4Willner N. Burwash I.G. Beauchesne L. Chan V. Vulesevic B. Ascah K. Coutinho T. Promislow S. Stadnick E. Chan K.L. Natural History of Mitral Annular Calcification and Calcific Mitral Valve Disease J. Am. Soc. Echocardiogr.20223592593210.1016/j.echo.2022.05.00735618253 · doi ↗ · pubmed ↗
- 5Wang T.K.M. Griffin B.P. Xu B. Rodriguez L.L. Popovic Z.B. Gillinov M.A. Pettersson G.B. Desai M.Y. Relationships between Mitral Annular Calcification and Cardiovascular Events: A Meta-analysis Echocardiography 2020371723173110.1111/echo.1486132949217 · doi ↗ · pubmed ↗
- 6Kohsaka S. Jin Z. Rundek T. Boden-Albala B. Homma S. Sacco R.L. Di Tullio M.R. Impact of Mitral Annular Calcification on Cardiovascular Events in a Multiethnic Community JACC Cardiovasc. Imaging 2008161762310.1016/j.jcmg.2008.07.00619356491 PMC 2847358 · doi ↗ · pubmed ↗
- 7Moradi M. Jahromi A.S. Prognostic Value of Mitral Annular Calcification in Coronary Atherosclerotic Disease Assessed by Coronary Computed Tomographic Angiography J. Res. Med. Sci.202429310.4103/jrms.jrms_53_2338524747 PMC 10956555 · doi ↗ · pubmed ↗
- 8Babul Mia M. Rezaul Karim M. Hossain N. Jahurul Haque M. Ahmed Chowdhury T. Hoque S. History A. Mitral annular calcification: A marker of severe coronary artery disease in patients under 60 years old Med. Res. Chron.20229496504