Utility of Circulating Tumor DNA to Assess Tumor Response in Patients with Locally Advanced Rectal Cancer Undergoing Neoadjuvant Therapy
Sakti Chakrabarti, Stacey A. Cohen, Antony Tin, Autumn Dangl, Ki Y. Chung, Mohamedtaki A. Tejani, Marwan G. Fakih, Sreenivasa R. Chandana, Colleen A. Donahue, Virgilio George, Midhun Malla, Vasily N. Aushev, Giby V. George, J. Bryce Ortiz, Whitney K. Herter, Arun Nagarajan

TL;DR
This study shows that measuring tumor DNA in the blood can predict cancer recurrence risk in rectal cancer patients, especially those avoiding surgery.
Contribution
The study demonstrates that ctDNA is a strong predictor of recurrence in rectal cancer patients, including those undergoing non-operative management.
Findings
ctDNA positivity after NAT or surgery was strongly correlated with recurrence risk.
Post-NAT ctDNA negativity predicted durable responses in non-operatively managed patients.
ctDNA clearance after surgery was associated with better outcomes in surgical patients.
Abstract
Here, we evaluated whether circulating tumor DNA (ctDNA) measured after neoadjuvant therapy (NAT) or surgery can help to assess tumor response and predict recurrence risk in patients with locally advanced rectal cancer, including those managed non-operatively (NOM). In this large real-world study of 220 patients, ctDNA positivity after NAT or surgery was strongly correlated with recurrence risk. Among the NOM patients, post-NAT ctDNA positivity identified individuals at nearly universal risk of local regrowth, while ctDNA negativity predicted durable responses. In the surgical patients, ctDNA clearance after resection was associated with favorable outcomes. ctDNA provides a molecular measure of treatment response that complements radiographic and endoscopic assessment. These findings suggest that ctDNA may help to tailor local therapy and surveillance strategies in rectal cancer and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
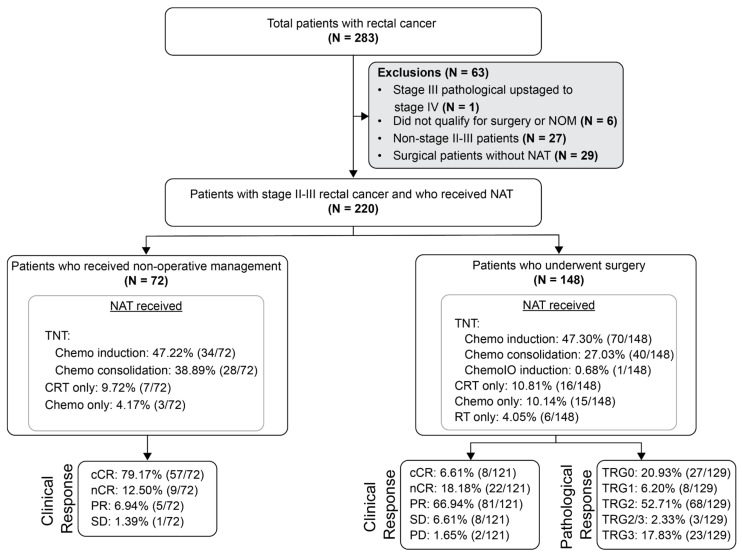 Figure 1
Figure 1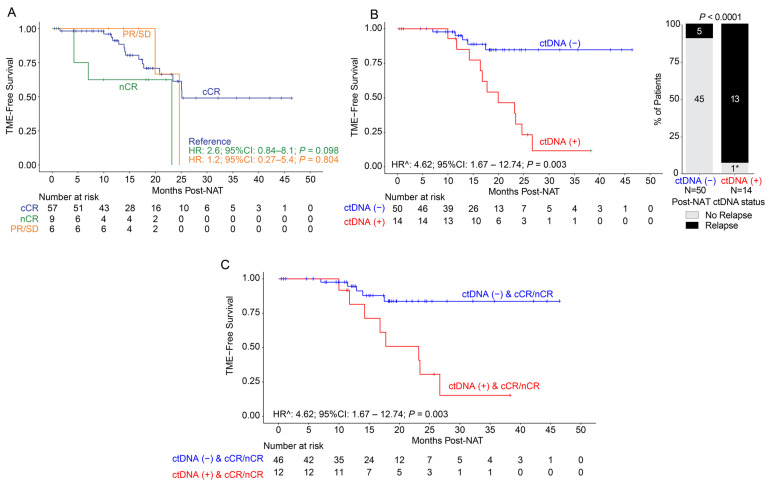 Figure 2
Figure 2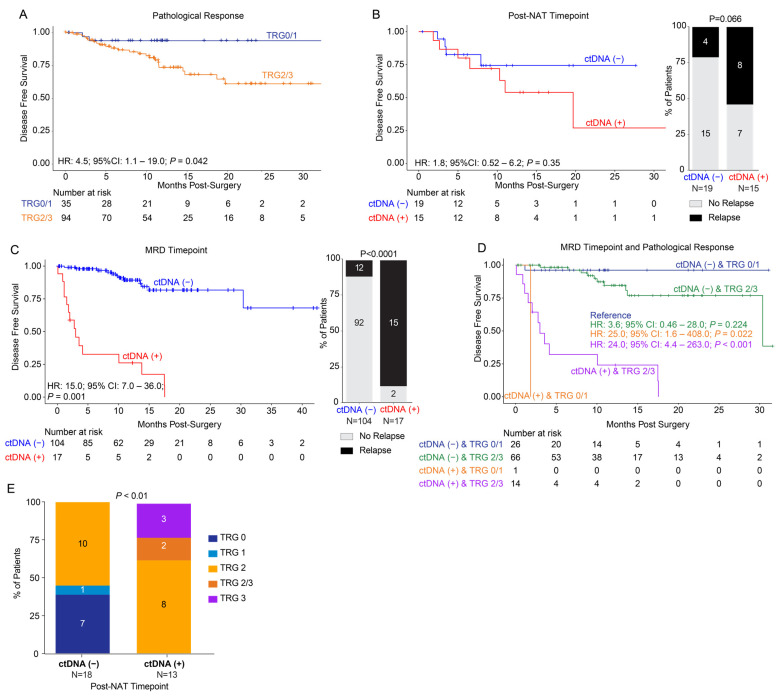 Figure 3
Figure 3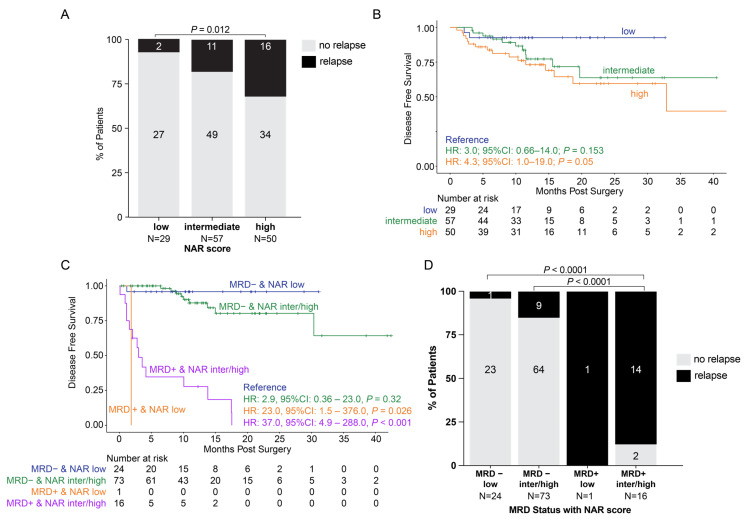 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Genomics and Diagnostics · Cancer Cells and Metastasis · Genetic factors in colorectal cancer
1. Introduction
The management of locally advanced rectal cancer (LARC) is guided primarily by clinical stage [1,2,3]. Standard treatment for stages II–III disease includes neoadjuvant therapy (NAT), followed by surgery for those with residual disease, and selective use of adjuvant chemotherapy. For patients achieving a complete clinical response (cCR) after NAT, as assessed by radiographic and endoscopic evaluation, non-operative management (NOM) is considered [3,4,5]. The options for NAT include chemoradiation (CRT) alone or total neoadjuvant therapy (TNT), in which multiagent chemotherapy and CRT are delivered preoperatively, with TNT increasingly favored [6,7]. Phase III trials have demonstrated that TNT reduces disease-related treatment failure (RAPIDO) and improves overall survival (PRODIGE 23) [8,9,10,11,12]. TNT also increases cCR rates (20–40% vs. 10–20% with CRT), expands opportunities for NOM, and reduces distant metastases [1,8,13,14,15].
Approximately 10–30% of patients with localized rectal cancer achieve pathological complete response (pCR) [16,17]. Identifying patients with substantial tumor regression after NAT is critical for selecting candidates for organ-preserving strategies while avoiding post-operative morbidity [18]. However, clinical assessment remains imperfect: cCR does not reliably equate to pCR or absence of molecular residual disease (MRD) [19], and patients managed with NOM continue to face substantial risks of local regrowth or distant recurrence [20,21].
In recent years, circulating tumor DNA (ctDNA) assays have emerged as important investigational tools in localized and metastatic colorectal cancer [22,23,24,25]. In early-stage colon cancer, post-operative ctDNA detection is a strong predictor of recurrence [26,27]. Yet, the relevance of ctDNA detection after NAT or surgery in LARC, and its potential role in NOM, remain undefined.
To address this gap, we analyzed real-world data from patients with LARC treated with standard NAT, surgery, or NOM. Our goal was to evaluate the prognostic potential of ctDNA in LARC, including its ability to identify patients at increased risk of recurrence after NAT or surgery and those undergoing NOM.
2. Materials and Methods
2.1. Subjects and Study Design
A total of 283 patients with rectal cancer who underwent testing using a tumor-informed ctDNA assay, Signatera™ (Natera, Inc., Austin, TX, USA), from multiple institutions between April 2018 and July 2024 were eligible for analysis. Tests were ordered commercially according to the provider’s clinical practice, and patients (stages II–III) meeting the inclusion criteria (n = 220, 1572 plasma samples) were identified retrospectively. Criteria for patient inclusion were confirmed stages II–III LARC and receipt of NAT followed by surgical resection or NOM. Post-NAT clinical response used to stratify patients for surgery or for NOM was determined by the ordering physician based on post-NAT MRI, digital rectal exam (DRE), and proctoscopy results.
Patients were assigned to the surgical cohort if they underwent surgery following NAT. For patients in the surgical cohort, the MRD window was defined as 2–12 weeks after surgery prior to the initiation of NAT. Patients were assigned to the NOM cohort if, following NAT, they were initially managed without immediate surgery regardless of whether salvage TME surgery was later performed for local regrowth. Patients achieving complete clinical response (cCR) or near-complete response (nCR) were considered eligible for NOM. A small number of patients with either partial response (PR) or stable disease (SD) were included in the NOM cohort at the provider’s discretion or due to patient choice. Patients who underwent upfront surgery without NAT (N = 29); those who were not eligible for surgery or NOM, declined surgery, or were inoperable despite having gross residual disease post-NAT (N = 6); or who were not stages II–III (N = 27) were excluded (Figure 1).
This study was conducted in compliance with Natera’s Institutional Review Board (IRB)-approved protocol (Salus #21204-02B), the Declaration of Helsinki, Title 21 of the US Code of Federal Regulations (CFR) as applicable, Good Clinical Practice guidelines, and International Conference on Harmonization guidelines. A waiver of the consent process and of the requirement for documentation of informed consent was granted according to 45 CFR 46.116(d) and 45 CFR 46.117(c)(2), respectively.
2.2. Personalized ctDNA Assay Workflow
For all patients, blood specimens (two 10 mL Streck tubes) were collected at the discretion of the ordering physician, with an average of 7 samples per patient (range: 1–28). All biological specimens were processed according to a CLIA-validated standard operating procedure at Natera, Inc. ctDNA analysis was performed using a clinically validated, personalized, and tumor-informed 16-plex PCR next-generation sequencing (NGS) assay (Signatera™, Natera, Inc., Austin, TX, USA) in patients undergoing commercial ordering as previously described [28]. Briefly, whole-exome sequencing (WES) was performed on formalin-fixed and paraffin-embedded tumor tissue, along with matched normal DNA blood samples from each patient. Based on the WES results, a personalized assay consisting of multiplex PCR (mPCR) primers was designed for 16 high-ranked patient-specific somatic single-nucleotide variants (SNVs) for each patient. The mPCR assay was then utilized in the associated patients’ plasma-derived cfDNA to detect and track ctDNA. Plasma cfDNA samples with ≥2 SNVs above a predefined algorithmic confidence threshold were considered ctDNA-positive. ctDNA concentration (levels) was quantitatively reported as mean tumor molecules (MTMs) per mL of plasma.
2.3. Statistical Analyses
For surgical patients, the primary outcome was disease-free survival (DFS), defined as the time from surgery to endoscopic or radiological recurrence (locoregional or distant) or death, and censored at last follow-up or death. For NOM patients, the primary outcome was TME-free survival, measured as time from NAT completion to salvage surgery or death. Survival analysis was performed using the Kaplan–Meier method and R software (v4.3.1; RRID:SCR_000432). To account for immortal time bias, we applied a landmark analysis, restricting post-operative MRD assessment to the 2–12-week window after surgery and only including patients who were alive and event-free until ≥12 weeks after surgery. A multivariable Cox proportional hazards model was used to assess the most significant prognostic factor associated with DFS. To account for variability in the timing and frequency of ctDNA sampling during surveillance, ctDNA status was modeled as a time-varying covariate in a time-dependent Cox regression for some analyses. All p-values were based on two-sided testing and considered significant at p ≤ 0.05. Time-dependent Cox regression evaluated serial ctDNA analysis during surveillance.
3. Results
3.1. Patient Cohort
A total of 1572 plasma samples were collected from 220 patients with stages II–III rectal cancer (median age: 59 years [range: 32–89 years]). Specific details regarding tumor type, pathologic stage, and treatment are described in Table 1. In total, 32.9% (72/220) received non-operative management (NOM) after NAT, and 67.12% (148/220) of the patients underwent surgery following NAT (Figure 1). NAT included total neoadjuvant therapy (TNT), chemotherapy alone, and chemoradiation/radiation alone.
For the surgical cohort, ctDNA at the post-NAT timepoint was collected at a median of 1.4 months (range: 0.5–6.3 months) after the completion of planned NAT, prior to surgery, with a median length of time between completion of NAT and surgery of 68 days (range: 6–270 days). For the NOM cohort, the first timepoint collected was at a median of 2.9 months (range: 0–40 months) after completion of planned NAT. All serial post-NAT ctDNA timepoints from the completion of NAT up to the time of recurrence or last follow-up, if no relapse, were evaluated. In the NOM cohort, 32 patients had their first available ctDNA within 3 months post-NAT; 6.3% (2/32) were ctDNA-positive, both of whom experienced local recurrence. Of the remaining 30 ctDNA-negative patients, 20% (6/30) converted to ctDNA-positive during serial testing, and all subsequently developed local recurrence, and none developed distant metastatic recurrence.
3.2. NOM Cohort: Post-NAT Association of Clinical Response and ctDNA Status with DFS
Of the 72 patients pursuing NOM after NAT, 79.1% (57/72) showed cCR, 12.5% (9/72) showed near-complete response (nCR), 6.9% (5/72) showed partial response (PR), and 1.4% (1/72) showed stable disease (SD). Of the six patients with PR or SD, three eventually achieved cCR without additional treatment intervention. The median follow-up post-NAT was 17 months (range: 1–48). When evaluating TME-free survival by clinical response, no statistically significant differences were observed between responses (Figure 2A).
By ctDNA status, 92.0% (46/50) of the ctDNA-negative patients showed cCR/nCR compared to 85.7% (12/14) of ctDNA-positive patients. Regardless of post-NAT ctDNA status, the clinical response status (cCR/nCR vs. PR/SD) between the ctDNA-negative or positive group was not statistically different, p = 1. However, when comparing relapse to non-relapse patients between the post-NAT ctDNA-negative and -positive groups, the difference was statistically significant, p < 0.0001 (Figure 2B), suggesting that, in NOM-eligible patients, post-NAT ctDNA can identify the patients who will eventually relapse.
On evaluating TME-free survival stratified by ctDNA status, the ctDNA-positive patients demonstrated significantly inferior outcomes compared to the ctDNA-negative patients (time-dependent HR: 4.62, 95% CI: 1.67–12.74, p = 0.003; Figure 2B). Due to the nature of serial testing and variable frequency of plasma collection for monitoring, the post-NAT analysis included ctDNA testing from the completion of NAT up to the time of recurrence or until the last clinical follow-up for patients who did not recur. Among the NOM patients with ctDNA available after completion of NAT (N = 64), 78.1% (50/64) were ctDNA-negative and 21.9% (14/64) were ctDNA-positive. Furthermore, 92.9% (13/14) of the ctDNA-positive post-NAT patients relapsed or progressed compared to only 10% (5/50) of the ctDNA-negative patients. The one remaining patient with ctDNA positivity post-NAT had multiple ctDNA-positive samples accompanied by a suspicious imaging 1 month after turning ctDNA-positive. This patient ultimately relapsed 8 months after the data cut-off. Among the five post-NAT ctDNA-negative patients who relapsed, one patient only had one post-NAT ctDNA draw that was taken 310 days prior to relapse, and another eventually experienced ctDNA positivity immediately after clinical recurrence 154 days later. We observed that the median time to molecular recurrence post-NAT was 8.9 months (range: 0.32–27.8) and the median time to clinical recurrence post-NAT was 13.5 months (range: 8.1–25.1) post-NAT.
Of note, among the 13 post-NAT ctDNA-positive patients who relapsed, all 13 (100%) had local regrowth or local recurrence, except one had both local and lung recurrence. Interestingly, when utilizing clinical response as an adjunct to ctDNA status post-NAT, among the patients who achieved cCR/nCR, ctDNA-positive status remained significantly associated with inferior TME-free survival (time-dependent HR: 4.62, 95% CI: 1.67–12.74, p = 0.003; Figure 2C).
3.3. Surgical Cohort: Association of ctDNA Status with Pathological Response and DFS
A total of 148 patients underwent surgical resection, and, of these, pathological response to neoadjuvant therapy was available for 129 patients. The median clinical follow-up post-surgery was 11 months (range: 0–44). For patients with pathological response data available, 20.9% (27/129) had a TRG 0 score, 6.2% (8/129) were TRG 1, 52.7% (68/129) were TRG 2, 2.3% (3/129) were TRG 2/3, and 17.8% (23/129) were TRG3. Upon evaluating DFS stratified by pathological response, patients with TRG scores 2–3 showed inferior outcomes when compared to patients with TRG scores 0–1 (pathological response: HR: 4.5, 95% CI: 1.1–19.0, p = 0.042; Figure 3A).
On stratifying patients with available ctDNA (N = 34) at the post-NAT timepoint, patients with ctDNA positivity showed worse DFS compared to ctDNA-negative patients (HR: 1.8, 95% CI: 0.52–6.2, p = 0.35), with relapse rates of 53% (8/15) and 21% (4/19) for the ctDNA-positive and -negative groups, respectively. However, this finding was not statistically significant (Figure 3B). The median follow-up for these 34 patients was 11 months (range: 0–27). Of note, at the post-operative MRD timepoint (N = 121), patients with ctDNA positivity showed a significantly inferior DFS (HR: 15.0; 95% CI: 7.0–36.0, p = 0.001. Figure 3C), with a relapse rate of 11.5% (12/104) for ctDNA-negative patients and 88% (15/17) for ctDNA-positive patients (p < 0.0001). Of the surgical patients who were ctDNA-positive at the post-NAT timepoint (n = 15), 80% (12/15) also had available ctDNA timepoints during the MRD window. Of these, three were ctDNA-positive in the MRD window, while nine were ctDNA-negative. All three patients with ctDNA positivity had distant recurrences. Of the nine patients who were ctDNA-negative, six remained relapse-free and three eventually relapsed (two distant and one local), with two of these turning ctDNA-positive prior to recurrence during surveillance.
Furthermore, upon assessing DFS based on ctDNA status in conjunction with pathological response, ctDNA-negative patients showed improved DFS regardless of TRG score. By contrast, ctDNA-positive patients with a TRG score of 0/1 (HR: 25.0; 95% CI: 1.6–408.0; p = 0.02) or a TRG score of 2/3 (HR: 24.0; 95% CI: 4.4–263.0, p < 0.001) displayed significantly inferior DFS (Figure 3D). Additionally, at the post-NAT timepoint, none of the ctDNA-negative patients showed TRG scores 2/3-3, while, among the ctDNA-positive patients, none had a TRG score 0/1. Each category of TRG score was statistically significantly different between the ctDNA-positive and -negative groups (p < 0.01; Figure 3E).
3.4. Surgical Cohort: NAR Score and Association with ctDNA Status and Outcomes
In our study, we observed that patients with high NAR scores exhibited a significantly higher recurrence rate of 32% (16/50) when compared to patients with low NAR scores (7% [2/29], p = 0.012. Figure 4A). Additionally, we observed that patients with high (HR: 4.3, 95% CI: 1.0–19.0, p = 0.05) and intermediate (HR: 3.0, 95% CI: 0.66–14.0, p = 0.153) NAR scores exhibited inferior DFS when compared to patients with low NAR scores (Figure 4B). When assessing ctDNA status at the post-op MRD timepoint in conjunction with the NAR score, we found that patients with high NAR scores were more frequently ctDNA-positive (27% [14/51]) than patients with intermediate (11% [6/54], p = 0.05) and low (4% [1/25], p = 0.02) NAR scores.
When evaluating DFS, we found that the use of ctDNA status at the MRD window enhances the predictive utility of the NAR score. While patients with intermediate or high NAR scores had a worse prognosis than those with low NAR scores, the majority of intermediate and high NAR scores did not recur (81% and 68%, respectively). When coupled with ctDNA status at the MRD window, ctDNA can further stratify the NAR low, intermediate, and high patients and predict relapse. As shown in Figure 4C, regardless of NAR score, patients who were ctDNA-positive in the MRD window had inferior outcomes compared to patients who were ctDNA-negative (ctDNA-positive with low NAR: HR: 23.0, 95% CI: 1.5–376.0, p = 0.026; ctDNA-positive with intermediate/high NAR: HR: 37.0, 95% CI: 4.9–288.0, p < 0.001). There was no statistically significant difference between ctDNA-negative patients with low and intermediate/high NAR scores. Finally, the relapse rates were higher in patients who were ctDNA-positive when compared to patients who were ctDNA-negative regardless of NAR score (p < 0.0001 for all comparisons. Figure 4D).
4. Discussion
ctDNA has emerged as a prognostic biomarker and shows the potential to transform response assessment and recurrence risk stratification in patients with LARC, particularly as treatment paradigms shift toward organ preservation. In this largest-to-date real-world study of ctDNA in LARC, we demonstrate the clinical relevance of ctDNA testing at both post-neoadjuvant and post-surgical timepoints across patients managed with surgery or NOM. Our findings reveal that ctDNA positivity robustly predicts recurrence, even among patients with radiographic or endoscopic complete response, highlighting its value in informing critical treatment decisions.
Importantly, this study offers real-world insights on the utility of ctDNA in the management of LARC. Among the surgical patients, particularly those achieving cCR, post-NAT ctDNA negativity may identify candidates for treatment de-escalation and less intensive surveillance. Conversely, in the NOM patients, post-NAT ctDNA positivity was strongly associated with local regrowth, suggesting a role for treatment escalation or earlier salvage surgery. Serial ctDNA testing during surveillance may refine risk stratification, distinguishing durable responders from patients at increased risk of recurrence. Additionally, ctDNA negativity may help to identify patients who are suitable for less intensive surveillance, while ctDNA positivity may inform risk stratification and consideration of closer monitoring or alternative management strategies. However, prospective interventional trials are underway and will be required before ctDNA-guided treatment escalation or de-escalation can be adopted in routine clinical practice. Collectively, these findings support the role of ctDNA as a complementary tool to imaging and endoscopy and provide a rationale for prospective trials evaluating ctDNA-guided management strategies in LARC.
A significant proportion of patients in the current study underwent NOM. Our study provides critical insight into the significance of post-NAT ctDNA status in this group. NOM, first popularized by Habr-Gama et al., is increasingly used for select patients with LARC [5]. A previous study reported baseline ctDNA combined with positive MRI extramural venous invasion to predict response [29]. Here, we found that post-NAT ctDNA status was strongly prognostic of outcomes among NOM patients (time-dependent HR: 4.62, 95% CI: 1.67–12.74, p = 0.003) independent of clinical response (cCR/nCR p = 0.003). Post-NAT ctDNA negativity was associated with remaining relapse-free, whereas ctDNA-positive patients had a high recurrence rate (13/14, 92.9%), suggesting that these patients may not be suitable for a non-operative approach. It is important to note that the one (7.1%; 1/14) remaining patient who was post-NAT ctDNA-positive recurred 8 months after the data cut-off. Therefore, even among patients with cCR/nCR, those who were ctDNA-positive had a 100% recurrence rate (PPV). Notably, all the ctDNA-positive patients had local recurrences, including the patient who recurred after data lock, with one patient having an additional lung recurrence.
Among the patients in the surgical cohort, we found that post-NAT ctDNA status correlated with pathological response, suggesting that it may serve as a surrogate for pathological response. An earlier phase 2 randomized trial reported improved 3-year DFS (71.6%) with adjuvant FOLFOX among patients with post-operative stages II–III disease and high-risk features following preoperative chemoradiotherapy [30]. Since then, several studies have demonstrated ctDNA positivity post-NAT to be associated with an increased risk of recurrence among patients with rectal cancer [25,31]. Here, we found that the prognostic performance of ctDNA differed depending on the timing of assessment in surgical patients. While ctDNA positivity at the post-NAT pre-surgical timepoint was associated with inferior DFS, this association did not reach statistical significance, likely reflecting the residual tumor heterogeneity prior to resection, variable timing of sampling, and limited sample size at this timepoint. In contrast, ctDNA status during the post-operative MRD window was a highly robust and statistically significant predictor of recurrence, consistent with the concept that definitive surgical clearance establishes the most informative biological context for MRD assessment. These findings suggest that ctDNA testing after surgical resection represents a reliable prognostic window for recurrence risk stratification in surgically managed patients with LARC.
Consistent with the published data [25,31,32,33], we found ctDNA positivity during the MRD window (2–12 weeks post-surgery) to be associated with poor outcomes (HR: 15.0, 95% CI: 7.0–36.0, p = 0.001). As previously described, the neoadjuvant rectal (NAR) score, calculated using the clinical tumor stage and pathological nodal and tumor stage, can be used as a composite short-term assessment of NAT response [34,35]. We observed that MRD ctDNA status was associated with NAR score, thereby substantiating our previous findings. When used as an adjunct to the NAR score, MRD ctDNA status was found to be the main driver of DFS when compared to the NAR score alone. These patients may benefit from ctDNA-specific clinical trials to address biochemical recurrence. Finally, it is worth noting that local relapse was more frequent among the NOM patients, whereas distant relapse predominated in the surgical cohort.
Our study has several limitations inherent to its real-world retrospective design. The treatment approaches varied across sites, including differences in NAT regimens and NOM implementation. ctDNA testing was performed at the discretion of the treating physicians, resulting in variability in timing and frequency of sampling. This may introduce selection bias as testing may have been preferentially performed in patients perceived to be at higher risk or with equivocal clinical responses. Moreover, while this heterogeneity may introduce confounding, it also reflects contemporary clinical practice and enhances the generalizability of our findings. In some instances, ctDNA results may have influenced clinical decisions in real time, which we acknowledge could affect outcome associations; however, this feature underscores the relevance of ctDNA in routine practice rather than diminishing its potential utility. The follow-up duration was relatively short, which may explain the predominance of local, rather than distant, recurrences observed. An additional limitation relates to the timing of post-NAT ctDNA assessments. Since this was not a prospectively designed study, only a small subset of patients underwent ctDNA testing at standardized timepoints post-NAT, precluding statistically meaningful subgroup analyses for clinical decision-making at the time of NOM consideration. Additionally, the median follow-up after surgery was relatively short, which may preferentially capture early local recurrences and underestimate the incidence of later distant metastases. Longer follow-up will be important to fully define the temporal relationship between the ctDNA dynamics and patterns of recurrence in this population. Despite these limitations, our study results are hypothesis-generating and represent the largest-to-date real-world cohort of patients with LARC undergoing NOM or surgery with serial ctDNA testing. The consistent associations we observed across multiple analyses support the robustness of our findings and highlight the potential of ctDNA to inform both surveillance and treatment decision-making.
5. Conclusions
In this large real-world cohort of patients with LARC, ctDNA status at both post-NAT and MRD timepoints correlated with clinical response, pathological response, and recurrence outcomes. ctDNA testing may offer significant value for real-time clinical decision-making, particularly in selecting patients for NOM or intensified post-operative surveillance. Future prospective studies are warranted to validate these findings and to evaluate ctDNA-guided management strategies in clinical trials.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu S. Jiang T. Xiao L. Yang S. Liu Q. Gao Y. Chen G. Xiao W. Total Neoadjuvant Therapy (TNT) versus Standard Neoadjuvant Chemoradiotherapy for Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis Oncologist 202126 e 1555 e 156610.1002/onco.1382433987952 PMC 8417863 · doi ↗ · pubmed ↗
- 2Scott A.J. Kennedy E.B. Berlin J. Brown G. Chalabi M. Cho M.T. Cusnir M. Dorth J. George M. Kachnic L.A. Management of locally advanced rectal cancer: ASCO guideline J. Clin. Oncol.2024423355337510.1200/JCO.24.0116039116386 · doi ↗ · pubmed ↗
- 3Keller D.S. Berho M. Perez R.O. Wexner S.D. Chand M. The multidisciplinary management of rectal cancer Nat. Rev. Gastroenterol. Hepatol.20201741442910.1038/s 41575-020-0275-y 32203400 · doi ↗ · pubmed ↗
- 4Yang Y. Huang A. Sun Z. Hong H.-P. Kim N.K. Gu J. “Watch and wait” strategy after neoadjuvant chemoradiotherapy in rectal cancer: Opportunities and challenges Holist. Integr. Oncol.20232410.1007/s 44178-023-00024-1 · doi ↗
- 5Habr-Gama A. São Julião G.P. Vailati B.B. Castro I. Raffaele D. Management of the complete clinical response Clin. Colon Rectal Surg.20173038739410.1055/s-0037-160611629184475 PMC 5703663 · doi ↗ · pubmed ↗
- 6Zwart W.H. Hotca A. Hospers G.A. Goodman K.A. Garcia-Aguilar J. The multimodal management of locally advanced rectal cancer: Making sense of the new data Am. Soc. Clin. Oncol. Educ. Book 20224211410.1200/EDBK_35141135561302 · doi ↗ · pubmed ↗
- 7Schrag D. Shi Q. Weiser M.R. Gollub M.J. Saltz L.B. Musher B.L. Goldberg J. Al Baghdadi T. Goodman K.A. Mc Williams R.R. Preoperative treatment of locally advanced rectal cancer N. Engl. J. Med.202338932233410.1056/NEJ Moa 230326937272534 PMC 10775881 · doi ↗ · pubmed ↗
- 8Verheij F.S. Omer D.M. Williams H. Lin S.T. Qin L.X. Buckley J.T. Thompson H.M. Yuval J.B. Kim J.K. Dunne R.F. Long-term results of organ preservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy: The randomized phase II OPRA trial J. Clin. Oncol.20244250050610.1200/JCO.23.0120837883738 PMC 11578087 · doi ↗ · pubmed ↗