Current State of the Clinical Applications of Artificial Intelligence in Stroke: A Literature Review
Grant C. Sorkin, Nicholas M. Caffes, John P. Shank, James L. Hershey, Dana E. Knaub, Jillian C. Krebs, Muhammad H. Niazi

TL;DR
This paper reviews how artificial intelligence is currently being used in stroke care, from pre-hospital to recovery, and highlights the lack of strong clinical evidence for its effectiveness.
Contribution
The paper provides a comprehensive literature review on the clinical applications of AI in stroke care, emphasizing the current evidence levels and challenges.
Findings
No randomized controlled trials (RCTs) currently evaluate AI's impact on patient outcomes in stroke care.
AI has commercial applications in acute stroke care, particularly in imaging detection and telestroke assistance.
Early RCTs support AI's use in recovery phase technologies like robotics and brain-computer interfaces.
Abstract
Background: Artificial intelligence (AI) has emerged as a transformative tool in medicine, leveraging rapid analysis of large datasets to accelerate diagnosis, enhance clinical decision-making, and improve clinical workflows. This is highly relevant in stroke care given the time-sensitive nature of the disease process. This review evaluates the current landscape of evidence-based medicine utilizing AI in stroke, with emphasis on its use in phases of clinical care across the stroke continuum, including pre-hospital, acute, and recovery phases. This offers a comprehensive understanding of the current state of AI in both practice and literature. Methods: A review of major databases was conducted, identifying peer-reviewed literature evaluating the use of AI and its level of evidence across the stroke continuum. Given the heterogeneity of study designs, interventions, and outcome metrics…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
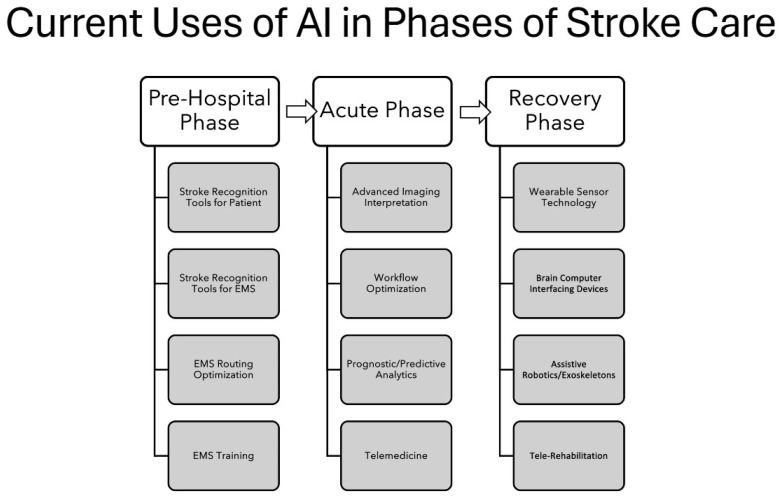 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Stroke Rehabilitation and Recovery · Artificial Intelligence in Healthcare and Education
1. Introduction
Stroke is a leading cause of morbidity and mortality, with improved outcomes associated with expedited diagnosis and treatment [1]. It affects more than 12 million people annually, represents one of the most time-sensitive emergencies in modern healthcare, and starts with primary prevention through risk factor modification and public education [2]. Current strategies for management include time-sensitive identification of large vessel occlusions (LVOs) using advanced imaging techniques, followed by vessel recanalization using systemic thrombolytics and intra-arterial thrombectomy therapies [3,4,5,6,7,8]. The delivery of these time-sensitive treatments becomes more difficult across geographically and socioeconomically diverse healthcare systems spanning urban, suburban, and rural regions, with uneven access to medical resources and advanced therapies [9,10].
Artificial intelligence has become increasingly integrated in healthcare, with strong appeal to stroke applications given the need for rapid diagnosis and treatment [11,12,13,14]. Artificial intelligence, an umbrella term incorporating machine learning, neural networks, and deep learning, may accelerate the diagnosis and treatment through interpreting and standardizing imaging, optimizing triage and transfer workflows, and risk stratification with predictive analytics, thereby narrowing geographic and socioeconomic inequalities [15,16,17,18,19]. Conceptually, machine learning is a broad field where computers use data models to learn patterns from human-constructed datasets. When connected, they create neural networks that consist of layers of data with increasing volume and complexity [20]. Deep learning models further connect neural networks into multiple layers, creating datasets so large and complex, with exponentially increasing computational power, that computers recognize patterns independent of human input or identification [20]. The choice of computational models becomes contingent on the complexity of the study question [20]. The presence of intracranial hemorrhage on non-contrast computer tomography might be identified with machine learning models while predictive analytics for stroke outcome and recurrence might require more complex deep learning models [21,22,23,24,25,26].
The existing literature evaluates AI used for stroke, categorized by specific applications including diagnostic imaging/interpretation, predictive analytics, workflow optimizations, and rehabilitation domains. This covers a broad array of topics whose audience spans multiple disciplines that participate directly or indirectly in the care of stroke patients, ranging from clinicians, to researchers, to engineers, to government-sponsored and private industry. This creates a piecemeal understanding of AI in stroke, weighted heavily to technical data and computational application, rather than a more general perspective of its clinical application and body of evidence. This review evaluates the current landscape of evidence-based medicine by organizing AI used in stroke care into clinical phases across the stroke continuum, including pre-hospital, acute, and recovery phases. By evaluating the literature according to clinical phase rather than application function, we hope to achieve a more global understanding of AI’s current implementation and remaining gaps in evidence.
2. Methodology
We conducted a narrative literature review of peer-reviewed published research from 2015 to 2025. Search terms included “artificial intelligence,” “machine learning,” “deep learning,” “neural network,” “stroke,” “community health systems,” “rural,” “telemedicine,” “telestroke,” “pre-hospital,” “stroke recovery,” and “stroke rehabilitation.” Databases including PubMed, Ovid Medline, Embase, and Scopus were searched using “or” as a Boolean operator restricted to title field and abstract, while using medical subject headings and synonym expansion. Inclusion criteria were peer-reviewed articles identified through the search strategy, including systematic, scoping, and narrative reviews; meta-analyses; validation and device trials; expert opinion articles; and original research with small sample sizes. Exclusion criteria included non-peer-reviewed papers, preprints, bench science without clinical relevance, and conference abstracts without full papers. Study selection was determined by agreement of the senior authors (GCS, MHN). Because the studies included were heterogeneous in designs, interventions, and outcomes, spanning multiple disciplines in a rapidly evolving, industry-dependent field, we used a narrative synthesis to provide a global view of the literature, organizing evidence into phases of clinical care across the stroke continuum with level of evidence according to the American College of Cardiology/American Heart Association classification system [27]. Given this review is secondary research of publicly available literature without patient identifiers, it is exempt from local institutional review board approval.
3. Results
3.1. Summary of Types of Existing Literature on AI Used for Stroke Care Across All Phases
The present body of literature evaluating AI for stroke is largely composed of retrospective studies evaluating proof-of-concept algorithms for imaging detecting, patient-level triage, and predictive analytics [13,21,22,23,24,25,26,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75]. This is followed by systematic, scoping, and narrative literature reviews of AI’s specific application in stroke care [11,14,15,16,17,18,76,77,78]. There remains a paucity of prospective studies with no randomized control trials evaluating patient-level outcomes [13,79]. Applying the American College of Cardiology/American Heart Association level of evidence classification system, the body of existing literature is largely composed of Level B-NR, and Level C studies with no Level A and few Level B-R randomized controlled trails [27]. Please refer to Level of Evidence Table 1, Table 2 and Table 3, which are categorized into phases of clinical care.
3.2. Summary of AI Use in Pre-Hospital Phase of Care
AI is increasingly applied to pre-hospital workflows to minimize delays in the recognition and treatment of acute ischemic stroke [76,77,78]. It has the potential to enhance the recognition of symptomatology by the patient as well as enhancing paramedic evaluation and triage in facilitating transfer to thrombectomy centers [82,126]. AI tools currently being evaluated in this phase of care can be broadly categorized into stroke recognition tools, Emergency Medical Services (EMS) tools, and novel strategies, all of which are in early stages of evaluation rather than commercially available [12]. Stroke recognition tools include wearable devices like watches, fitness bands, and rings to assess motor and gait characteristics, as well as smart tablets/devices and televisions that incorporate AI recognition of facial and speech patterns to identify stroke symptomatology [83,90,91,92,127]. EMS tools currently being evaluated use AI for (1) speech pattern recognition to assist EMS dispatchers, (2) optimizing ground and air ambulance routing for more efficient activation, and (3) enhancement of personnel training and competency [80,81,84,86,87,88,89,128]. Novel strategies of noninvasive and portable versions of EEGs, TCDs, or headsets that study electrical impedance of brain tissue remain at early stages of study, while telemedicine-enabled ambulances using AI-assisted recognition software demonstrate potential to overcome the limitations of scalability of mobile stroke units [85,129,130,131]. While such tools demonstrate feasibility and promise in their application, more research is required to achieve commercial availability.
3.3. Summary of AI Use in the Acute Phase of Care
The acute phase of care, defined as the index hospitalization for a stroke event encompassing emergency, perioperative, and postoperative care through discharge, is the most extensively represented phase in the current AI stroke literature [11,14,15,16,17,18,77,78]. The progress made in this domain has resulted in several commercial platforms currently available on national and global scales, having achieved 510 (k) or full Food and Drug Administration clearance, as of this paper [132,133,134,135,136,137,138]. These AI applications largely apply to advanced stroke imaging acquisition, automation, and interpretation, which can be customized to healthcare systems depending on stroke program infrastructure. These include LVO detection on computer tomography angiography, computer tomography perfusion mapping, magnetic resonance imaging diffuse weight imaging analysis, automated intracranial hemorrhage detection and classification, and Alberta Stroke Program Early CT Score automation [14,15,16,17,77,78,79,98,99,100,101,102,103,104,105,106,107,108]. Because these tools promote faster diagnosis by AI interpretation and imaging cue prioritization, they have the potential to streamline workflows and reduce both medical and surgical treatment delays [93,94,95,109]. They also have potential to improve emergency department stroke workflows and help bridge gaps in specialty coverage in systems lacking neurology or neuroradiology [14,15,16,17,18,77,78,95]. This phase of care derives the most benefit from AI-supported telemedicine platforms that allow remote neurologists to triage patients by immediate imaging interpretation, independent of radiology workflows, thereby reducing time to medical and revascularization treatment [94,95,96,97,110,111]. These platforms now incorporate physician communication capabilities which show promise in improving stroke alert activation time, tele-neurology activation time, and neurointerventional consultation times [96]. Lastly, this phase of care has the highest concentration of AI use for predictive analytics in stroke care [18]. These analytic tools have been used to assess functional outcomes after stroke [28,29,30,31,32], reperfusion therapy outcomes [33,34,35], stroke etiology and risk recurrence [36,37,38,39,40,41,42,43,62,63,64,65,66], extracranial carotid artery risk factors [21,44,45,46], and comorbidity complication outcomes including pneumonia and acute kidney injury [67,68,69,70].
3.4. Summary of AI Use in the Recovery Phase of Care
There has been rapid increase in the body of literature describing the use of AI for stroke rehabilitation over the last 10 years, with most studies being small, single-center and pilot feasibility studies using robotic integrated AI [117,119]. Motor applications include wearable sensors, AI-integrated robotics and exoskeletons that provide adaptive services, and AI virtual reality environments that can be customized to offer patient specific recovery experiences [112,117,119,121,124,125]. Neurocognitive applications include AI-driven apps with personalized adaptive algorithms and natural language processing-based analyses for speech, cognitive, and executive function training [120,122,123]. These tools, in combination with AI-enabled wearable technology that provides real-time feedback and predictive analytics, can help facilitate remote tele-rehabilitation services [112,117,119,121,124,125,139,140,141]. Brain–computer interfaces represent a growing area of investigation in stroke care, translating electrical, magnetic, or metabolic brain activity into control signals for external devices capable of replacing, restoring, or supplementing neurological function. Their use may serve as an adjunct to both motor rehabilitation and assistance in stroke patients for acute and chronic neurological deficits [113,114,115,116,118]. In the current literature, AI use in tele-rehabilitation and brain–computer interfaces represent the strongest evidence for AI in stroke care across clinical phases, with multiple small randomized controlled trials achieving Level B-R evidence [114,122,123]. While such tools demonstrate feasibility and early benefit in their application, more research is required to demonstrate benefit and achieve commercial availability.
4. Discussion
In the paradigm of therapy for LVOs, healthcare delivery required realignment to rapidly identify stroke, followed by vessel recanalization using systemic and intra-arterial therapies [3,4,5,6,7,8]. AI represents another realignment in healthcare delivery, offering accelerated diagnosis, predictive analytics, and treatment. These are synergistic with goals of time-dependent stroke workflows. By structuring the literature according to phases of stroke care, our review provides a more holistic understanding of AI’s application in clinical practice.
Existing reviews of AI in stroke care are narrowly focused, most often addressing AI-assisted LVO detection or workflow augmentation to expedite revascularization, with limited attention beyond the acute phase of stroke management [11,14,15,16,17,18,142]. This is demonstrated by the larger body of evidence in the acute phase (Table 2), compared to the pre-hospital (Table 1) or recovery phases (Table 3). Stroke care is a spectrum that encompasses a continuous, coordinated process beginning with primary prevention through risk factor modification and public education, extending through long-term recovery and, when appropriate, palliative care. Once stroke occurs, rapid pre-hospital recognition and triage are critical to ensure timely transport to stroke centers capable of providing diagnostic and revascularization therapies. The remaining acute care then becomes dedicated to etiologic evaluation, prevention of early complications, and initiation of secondary prevention strategies using antithrombic therapy for cardiovascular risk factor optimization. Rehabilitation then becomes an integral component of care, transitioning from the acute to recovery phase, emphasizing functional recovery through multidisciplinary therapy in addressing intermediate and long-term needs. Organizing the literature by these phases, as illustrated in Figure 1, offers a clearer, more clinically relevant view of current AI applications in stroke care.
The acute phase of care is the most represented in the current body of literature, with a concentration in imaging detection and interpretation, telemedicine and workflow augmentation, and predictive analytics. Despite consisting of non-randomized, Level B evidence (Level B-NR), to our knowledge, this is the only phase of care that has reached commercial application and scalability. However, the pre-hospital and recovery phases of care remain as important as the acute phase at the patient-level and should offer similar potential for research, innovation, and industry-sponsored collaboration. This is supported by several prospective RCTs that provide the strongest evidence to date for AI in the recovery phase of care, specifically evaluating its use in tele-rehabilitation [122,123] and brain–computer interfaces (Level B-R) [114].
Despite its immense potential, substantial challenges with AI integration in stroke care remain. Commercial availability of AI-enabled stroke tools in the acute phase of care and widespread clinical adoption should not be interpreted as evidence of proven patient-level benefit. Several platforms have achieved regulatory approval and become integrated into clinical workflows; however, randomized controlled trials and Level A evidence demonstrating improvement in functional outcomes or mortality remain lacking and no governing society has incorporated AI into stroke guideline statements to date [143]. Accordingly, the current evidence primarily supports operational and workflow efficiencies rather than definitive clinical efficacy. These are dependent on phase of care, local infrastructure, and institutional resources, thereby limiting broad standardization. Variability in data quality, imaging protocols, and industry vendors can affect algorithm performance and generalizability, particularly when tools are deployed outside of the environment in which they were developed. This compounds concern regarding algorithm bias and transparency [11,15,17,19]. There also remain ethical and regulatory questions about data equity, ownership, and protection, which, in summation, hinders trust among end users and results in hesitancy of clinician adoption [11,15,17,19]. Lastly, while AI’s use can narrow a geographic divide, care must be taken to prevent the widening of socioeconomic disparities in infrastructure involving availability of broadband or cloud computing resources, availability of neurology, neuroradiology or neurointerventional specialties, availability of telemedicine resources, availably of on-site information technology resources, and availability of electronic health record resources [10,144]. These components require significant capital expenditure without dedicated reimbursement, thereby contributing to delay in adoption by smaller or rural healthcare systems [10,144].
5. Limitations of This Review
This is a narrative synthesis rather than a full systematic review with defined search strings and independent double screening. While this was chosen to accommodate a broad scope of literature that spanned disciplines, topics, and outcomes, it can increase susceptibility to selection bias and incomplete coverage of relevant studies. The absence of formal risk-of-bias assessments, and reproducible methodology for the literature search, study selection, and data extraction limits the ability to critically appraise the quality of included studies, which is particularly important in AI research where heterogeneity in datasets, algorithms, and validation methods can be common. These limitations reduce transparency and make it difficult to draw robust conclusions about clinical effectiveness or generalizability. While narrative reviews are valuable for providing conceptual overviews and identifying emerging themes in a rapidly evolving field such as AI in stroke, they offer weaker evidentiary support than systematic reviews when informing clinical practice or policy decisions. Lastly, given the field’s rapidly evolving nature, driven in part by industry-sponsored collaboration, new high-quality trials, registries, and proprietary data continue to emerge, thereby creating an expiration date on a review discussing current state.
6. Conclusions
Spanning early symptom recognition by patients and EMS, rapid identification and treatment of large vessel occlusions, and AI-supported tele-rehabilitation and robotics, AI is positioned to impact all phases of stroke care. While key challenges remain regarding transparency, generalizability, and external validation, AI will continue to play an important role in healthcare realignment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Saver J.L. Time is Brain-quantified Stroke 20063726326610.1161/01.STR.0000196957.55928.ab 16339467 · doi ↗ · pubmed ↗
- 2Tsao C.W. Aday A.W. Almarzooq Z.I. Anderson C.A.M. Arora P. Avery C.L. Baker-Smith C.M. Beaton A.Z. Boehme A.K. Buxton A.E. Heart disease and stroke statistics—2023 update: A report from the American Heart Association Circulation 2023147 E 93E 62110.1161/CIR.000000000000112336695182 PMC 12135016 · doi ↗ · pubmed ↗
- 3Berkhemer O.A. Fransen P.S.S. Beumer D. van den Berg L.A. Lingsma H.F. Yoo A.J. Schonewille W.J. Vos J.A. Nederkoorn P.J. Wermer M.J.H. A randomized trial of intraarterial treatment for acute ischemic stroke N. Engl. J. Med.2015372112010.1056/NEJ Moa 141158725517348 · doi ↗ · pubmed ↗
- 4Goyal M. Demchuk A.M. Menon B.K. Eesa M. Rempel J.L. Thornton J. Roy D. Jovin T.G. Willinsky R.A. Sapkota B.L. Randomized assessment of rapid endovascular treatment of ischemic stroke N. Engl. J. Med.20153721019103010.1056/NEJ Moa 141490525671798 · doi ↗ · pubmed ↗
- 5Saver J.L. Goyal M. Bonafe A. Diener H.C. Levy E.I. Pereira V.M. Albers G.W. Cognard C. Cohen D.J. Hacke W. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke N. Engl. J. Med.20153722285229510.1056/NEJ Moa 141506125882376 · doi ↗ · pubmed ↗
- 6Campbell B.C.V. Mitchell P.J. Kleinig T.J. Dewey H.M. Churilov L. Yassi N. Yan B. Dowling R.J. Parsons M.W. Oxley T.J. Endovascular therapy for ischemic stroke with perfusion-imaging selection N. Engl. J. Med.20153721009101810.1056/NEJ Moa 141479225671797 · doi ↗ · pubmed ↗
- 7Jovin T.G. Chamorro A. Cobo E. de Miquel M.A. Molina C.A. Rovira A. San Román L. Serena J. Abilleira S. RibóM. Thrombectomy within 8 hours after symptom onset in ischemic stroke N. Engl. J. Med.20153722296230610.1056/NEJ Moa 150378025882510 · doi ↗ · pubmed ↗
- 8Goyal M. Menon B.K. van Zwam W.H. Dippel D.W.J. Mitchell P.J. Demchuk A.M. Dávalos A. Majoie C.B.L.M. van der Lugt A. de Miquel M.A. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials Lancet 20163871723173110.1016/S 0140-6736(16)00163-X 26898852 · doi ↗ · pubmed ↗