Extracorporeal Cytokine Adsorption in Acute Cardiovascular Care: Pathophysiological Insights and Clinical Perspectives
Klevis Mihali, Lukas Harbaum, Birgit Markus, Georgios Chatzis, Nikolaos Patsalis, Styliani Syntila, Bernhard Schieffer, Julian Kreutz

TL;DR
This paper reviews the use of extracorporeal cytokine adsorption in treating severe cardiovascular conditions like cardiogenic shock and post-cardiac arrest syndrome.
Contribution
The paper provides a comprehensive review of cytokine adsorption's pathophysiological basis and clinical evidence in acute cardiovascular care.
Findings
Cytokine adsorption reduces vasopressor demand and improves metabolic stabilization in some patients.
Clinical benefits remain inconsistent, with limited randomized trial data supporting routine use.
Early intervention and phenotype-guided selection may improve outcomes in specific patient groups.
Abstract
Background: Cardiogenic shock (CS) and post-cardiac arrest syndrome (PCAS) are frequently associated with a systemic inflammatory response resulting from ischemia–reperfusion injury, endothelial dysfunction, and microcirculatory impairment. This inflammatory biology may be further amplified by temporary mechanical circulatory support (tMCS) through blood–surface interactions and shear-related hemolysis. Extracorporeal cytokine adsorption has therefore been proposed as an adjunctive strategy to attenuate hyperinflammation and facilitate shock reversal in selected patients. Methods: We conducted a narrative review, guided by a targeted PubMed and Scopus search and reference screening, to summarize the current pathophysiological concepts and clinical evidence on extracorporeal cytokine adsorption in CS-, PCAS-, and tMCS-supported states. Results: Across porous polymer hemoadsorption…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
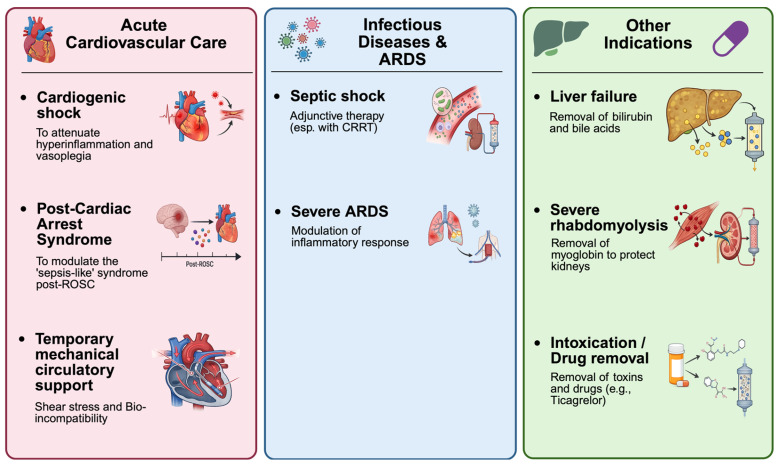 Figure 1
Figure 1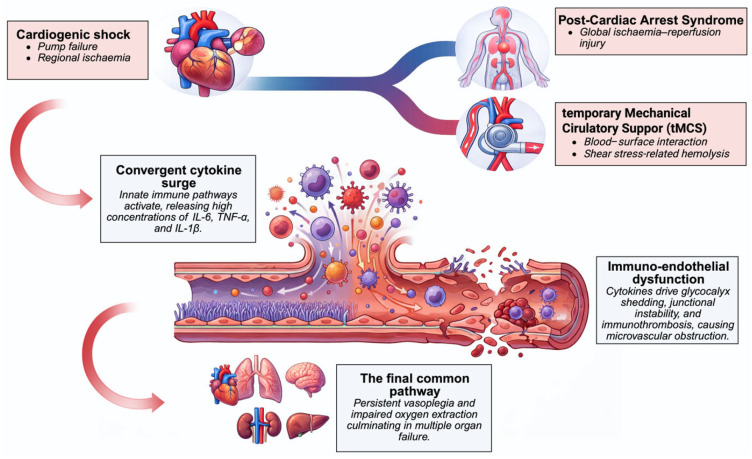 Figure 2
Figure 2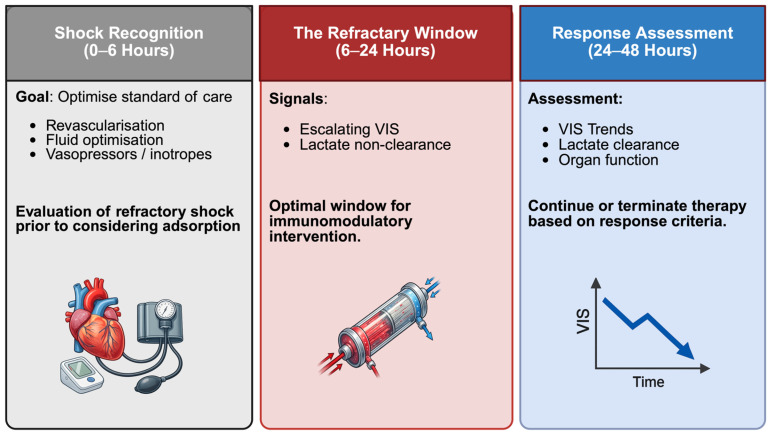 Figure 3
Figure 3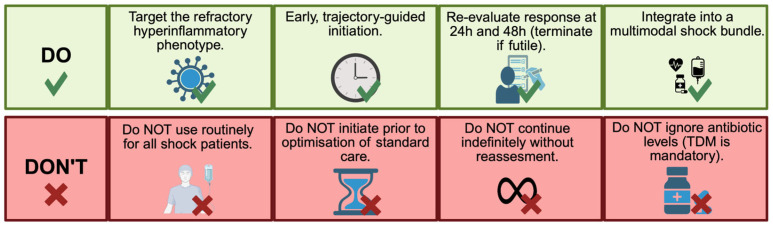 Figure 4
Figure 4- —Open Access Publishing Fund of Philipps-Universität Marburg
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Acute Kidney Injury Research · Cardiac and Coronary Surgery Techniques
1. Introduction
Cardiogenic shock (CS), post-cardiac arrest syndrome (PCAS), and clinical scenarios requiring temporary mechanical circulatory support (tMCS) represent three closely related yet distinct entities that rank among the most challenging conditions in acute cardiovascular care. Although differing in their underlying pathophysiology, all three share common features of profound hemodynamic instability and frequently coexist in critically ill patients. Despite advances in intensive care, reperfusion strategies, and mechanical support technologies, mortality rates remain high. In CS related to acute myocardial infarction (AMI), 30-day mortality continues to exceed 40–50%, even with early revascularization, as evidenced by contemporary registries and population-based cohorts [1,2,3,4]. These persistently poor outcomes highlight that myocardial pump failure and maladaptive systemic inflammation with macro- and microcirculatory disturbances are both major factors in hemodynamic instability and multiple organ failure [5,6]. PCAS adds an additional layer of complexity: Global ischemia–reperfusion during cardiac arrest and resuscitation triggers a sepsis-like syndrome with profound immune activation, vasoplegia, microvascular dysfunction, and secondary organ injury, often compounded by myocardial stunning and hypoxic–ischemic brain injury [7,8]. Like in refractory CS, tMCS devices, including percutaneous microaxial flow pumps (mAFPs) and veno-arterial extracorporeal membrane oxygenation (VA-ECMO), can contribute to the hemodynamic stabilization and improvement of end-organ perfusion. However, device–blood interactions themselves, complement activation, shear-induced hemolysis, and ischemic complications may exacerbate cytokinaemia and endothelial damage [9,10]. Moreover, extracorporeal cardiopulmonary resuscitation (eCPR) using VA-ECMO is becoming more common in patients with refractory cardiac arrest to restore macrocirculation. However, even after blood flow is normalized, inflammation and downstream endothelial activation may persist. Against this background, interest has grown in adjunctive extracorporeal strategies aimed at attenuating hyperinflammation and its haemodynamic consequences.
In acute cardiovascular intensive care, several extracorporeal cytokine adsorption approaches are currently applied to modulate systemic inflammation. These include classical cytokine adsorbers based on porous polymer resins, such as CytoSorb^®^ (CytoSorbents, Princeton, NJ, USA); membrane-based and hybrid filters with cytokine adsorption capacity, such as oXiris^®^ (AN69-oXiris, Baxter/Gambro [Vantive], Europe (Lessines, Belgium)/(Deerfield, IL, USA)); and selective adsorbers targeting other inflammatory mediators, such as PentraSorb^®^ CRP (Pentracor, Kleinmachnow, Germany). These devices can be used as stand-alone hemoperfusion systems or integrated into continuous renal replacement therapy (CRRT) and ECMO circuits. While extracorporeal cytokine adsorption has been extensively studied in sepsis and septic shock, its role in acute cardiovascular syndromes remains comparatively underrepresented and fragmented. In contrast to the large body of sepsis-focused literature, evidence on CS-, PCAS-, and tMCS-supported states is derived predominantly from small observational cohorts and selected randomized pilot trials. By aligning these syndromes within a shared immune–endothelial framework and highlighting device-specific inflammatory drivers, we aim to provide a cardiovascular-centred interpretive lens for patient selection, timing, and trial design. Across CS-, PCAS-, and tMCS-supported states, hemoadsorption has been associated with improved hemodynamic stabilization, reduced vasopressor demand, and modulation of inflammatory and metabolic markers in observational studies [11,12,13]. However, outcome benefits remain inconsistent and are not yet supported by randomized evidence. Accordingly, this narrative review integrates CS-, PCAS-, and tMCS-supported states into a shared immune–endothelial framework and contextualizes extracorporeal cytokine adsorption specifically within acute cardiovascular care. Rather than representing isolated indications, these conditions form a broader clinical continuum of hyperinflammatory critical illness in which extracorporeal cytokine adsorption has been explored across cardiovascular, septic, and toxin-driven contexts (Figure 1).
2. Methods
This article is a narrative review supported by identification of the targeted literature. To inform a concept-driven synthesis of pathophysiological mechanisms and clinical evidence, we consulted PubMed and Scopus (for publications from January 2018–December 2025) and complemented this by a reference screening of key articles and relevant reviews. The search terms were “cardiogenic shock” OR “post-cardiac arrest syndrome” OR “temporary mechanical circulatory support” OR “veno-arterial extracorporeal membrane oxygenation” OR “microaxial flow pump,” combined with “extracorporeal cytokine adsorption,” “hemoadsorption,” “CytoSorb,” “oXiris,” or “PentraSorb.” We focused on evidence from adult populations (≥18 years), reflecting the clinical scope of acute cardiovascular intensive care. Reference lists of key articles and relevant reviews were screened to identify the additional pertinent literature. No formal risk-of-bias assessment or quantitative evidence grading was performed, as these approaches are not appropriate for the integrative, narrative scope of this review.
3. Pathophysiological Basis of Hyperinflammation in Acute Cardiovascular Care
3.1. Cardiogenic Shock
CS is a state of critical end-organ hypoperfusion caused by primary cardiac pump failure, sustained by a maladaptive inflammatory response that disrupts macro- and microcirculatory coupling [14]. In AMI-related CS, regional ischaemia–reperfusion triggers cardiomyocyte necrosis, the release of damage-associated molecular patterns (DAMPs), the activation of innate immune pathways and a surge of cytokines such as tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-6 [15,16]. Downstream, endothelial activation with glycocalyx shedding, junctional instability, and immunothrombosis promotes microvascular obstruction and impaired oxygen extraction, thereby perpetuating vasoplegia and progressive organ dysfunction despite the restoration of epicardial flow [17]. Similar immune–endothelial mechanisms operate in non-ischaemic CS aetiologies, including acute decompensated heart failure, fulminant myocarditis, stress-induced cardiomyopathy, right ventricular failure, and mechanical complications of AMI.
Guideline-directed management prioritizes the rapid identification and definitive treatment of the underlying cause, early revascularisation in AMI with culprit-lesion percutaneous coronary intervention (PCI) or urgent coronary artery bypass grafting (CABG) when indicated, and structured haemodynamic support [18]. In persistent shock, invasive monitoring can support the individualized titration of preload, afterload, and inotropy [19,20,21]. Norepinephrine is the first-line vasopressor to restore mean arterial pressure, while inotropic support with dobutamine or milrinone is used to augment cardiac output, tailored to blood pressure, arrhythmia risk, and renal function [22,23]. The use of tMCS is considered according to shock severity and trajectory, typically following the Society for Cardiovascular Angiography and Interventions (SCAI) shock stages, with escalation from percutaneous left ventricular unloading with mAFPs to VA-ECMO in refractory cases and combined strategies when needed for oxygenation and perfusion alongside ventricular unloading. Current guidelines recommend using mAFPs in selected patients with CS, and recent studies highlight the increasing evidence supporting its use in CS associated with AMI [24,25]. Concomitant therapies include guideline-based antithrombotic treatment, ventilatory optimization, prevention and treatment of arrhythmias, correction of electrolyte and acid-base disturbances, and timely surgery for mechanical complications [26,27]. Alongside these measures, a subset of patients remains vasoplegic with persistent microcirculatory dysfunction, providing the biological rationale for adjunctive inflammation-modulating approaches targeting immune–endothelial dysregulation.
3.2. Post-Cardiac Arrest Syndrome
PCAS is conceptualized as a composite entity comprising hypoxic–ischaemic brain injury, transient post-arrest myocardial dysfunction, a whole-body ischaemia–reperfusion response, and persistent precipitating pathology [28]. Unlike predominantly regional ischaemia in AMI-related CS, PCAS is triggered by circulatory arrest followed by reperfusion. Together, whole-body hypoxia, disruption of the gut barrier, and resuscitation-related tissue injury trigger the release of DAMPs and endotoxins, activate pattern-recognition receptors and the complement system, and provoke a sepsis-like inflammatory response [29]. Studies have shown a correlation between higher concentrations of IL-6, IL-8, and IL-10 in the early stages, as well as the terminal complement complex, and more severe vasoplegia, lower cardiac output, an increased need for circulatory support, and a higher 30-day mortality rate [30,31]. These findings highlight the significance of the inflammatory response as a prognostic factor. Furthermore, endothelial damage has been shown to be a central mechanism in the pathophysiology of PCAS. Experimental and clinical data further suggest that ischaemia–reperfusion drives immune–endothelial dysfunction and blood–brain barrier injury, thereby linking post-resuscitation vasoplegia to secondary neuronal damage [32,33]. Post-resuscitation care focuses on the rapid identification and treatment of the precipitating cause, restoration and titration of haemodynamics with vasopressors and inotropes, lung-protective ventilation with careful oxygen and carbon dioxide control, fever prevention as part of temperature management, early consideration of tMCS in refractory circulatory failure, and structured neuroprognostication [8]. Within this bundle, patients exhibiting refractory vasoplegia, capillary-leak physiology and biochemical hyperinflammation despite optimized care represent the phenotype in which adjunctive, mechanism-targeted immunomodulation, including hemoadsorption within protocols or trials, may be explored.
3.3. Temporary Mechanical Circulatory Support and eCPR
While tMCS devices stabilize macrocirculation, they also introduce inflammatory drivers specific to the device, including blood–surface interactions, complement activation, and shear-induced hemolysis [34]. In VA-ECMO, non-pulsatile flow and retrograde aortic perfusion alter endothelial mechanotransduction, whereas mAFPs may promote hemolysis due to shear and suction effects [35,36]. Shear stress contributes to the development of acquired von Willebrand factor abnormalities and hemolysis. This releases plasma-free hemoglobin and heme, which scavenge nitric oxide and impair endothelium-dependent vasodilation. With mAFPs, such as the left ventricular Impella (Abiomed, Danvers, MA, USA), the load on the left ventricular wall is reduced and subendocardial blood flow improves. However, shear and suction effects can also cause hemolysis, activate the complement system, and contribute to cytokine release [34]. Combined approaches using VA-ECMO and Impella (ECMELLA) aim to balance oxygen supply and systemic perfusion with active unloading. In the context of refractory cardiac arrest, eCPR with consecutive VA-ECMO cannulation restores global flow but is followed by a pronounced whole-body reperfusion response that overlaps with PCAS biology and may persist despite normalized macrocirculatory parameters [37]. Management in tMCS-supported CS and PCAS focuses on meticulous device optimization and complication prevention. In VA-ECMO, key priorities are adequate anticoagulation, the monitoring and mitigation of hemolysis, ventilatory strategies to limit pulmonary edema, and timely venting or unloading of the left ventricle when pulmonary congestion, distension or intracardiac stasis occur [38]. In mAFP-supported patients, correct positioning, suction avoidance, hemolysis surveillance, and stepwise flow titration are central. In combined ECMELLA configurations, coordinated flow targets seek to balance oxygen delivery with ventricular decompression while minimizing recirculation and limb ischaemia. In these settings, it is clinically important to recognize hyperinflammatory trajectories, particularly when vasoplegia and lactate non-clearance persist despite technically adequate support, as this provides the context in which adjunctive cytokine-modulating strategies may be considered within institutional algorithms or trials.
Despite distinct initiating triggers, these syndromes converge on a shared hyperinflammatory end stage characterized by cytokinaemia, immune–endothelial dysfunction, microvascular failure, and progressive organ injury, forming a common biological substrate for adjunctive immunomodulatory strategies (Figure 2).
4. Rationale for Extracorporeal Cytokine Adsorption in CS, PCAS and tMCS
In the context of persistent immune–endothelial dysregulation despite macrocirculatory stabilization, extracorporeal cytokine adsorption has been proposed as an extracorporeal adjunct aimed at attenuating hyperinflammation rather than blocking individual signalling pathways [39]. The therapeutic goal is to mitigate endothelial activation and microvascular dysfunction, thereby improving vascular reactivity and macro–microcirculatory coupling by reducing the circulating concentrations of key mediators (e.g., IL-6, TNF-α, and IL-1β) as well as chemokines and alarmins [40]. In principle, this may translate into reduced vasoplegia, improved lactate clearance, and earlier de-escalation of vasoactive therapy; however, consistent effects on patient-centred outcomes have not been demonstrated [41]. Several blood purification approaches have been explored, including high-volume hemofiltration, high-cut-off membranes, plasmapheresis, and endotoxin-directed adsorption. Hemoadsorption is particularly attractive in cardiovascular intensive care medicine because it can be used as a stand-alone procedure or easily integrated into existing extracorporeal platforms, such as CRRT and VA-ECMO. It also covers a broad spectrum of cytokines and related mediators central to the biology of CS-, PCAS-, and tMCS-supported conditions [42].
5. Principles and Mechanisms of Extracorporeal Adsorption Therapies
The sorbent material, pore architecture, and surface functionalization of hemoadsorption systems differ, and together determine molecular breadth and adsorption kinetics [43]. In acute cardiovascular and intensive care medicine, the most used adsorbents are non-selective porous adsorption resins, such as CytoSorb. These cartridges typically contain cross-linked polystyrene–divinylbenzene beads with a hydrophilic coating and preferentially adsorb predominantly hydrophobic, mid-molecular-weight mediators (approximately 5–60 kDa) [44]. In addition to inflammatory mediators such as interleukins and TNF-α, resin cartridges can adsorb other clinically relevant solutes, including myoglobin and bilirubin, and may co-adsorb protein-bound medications [45]. This broad, concentration-dependent adsorption profile underlies their use in hyperinflammatory states and in device-supported shock, but it also necessitates careful consideration of drug exposure and dosing when adsorption is applied.
Membrane and hybrid designs expand the therapeutic spectrum for targeted applications. The oXiris^®^ membrane (Baxter, Deerfield, IL, USA) combines high-flow hemofiltration with coated adsorption surfaces, allowing for the simultaneous removal of cytokines and endotoxins [46].
PentraSorb^®^-CRP (PentraSorb GmbH, Kleinmachnow, Germany) is a highly selective adsorbent that targets the removal of C-reactive protein (CRP) to limit excessive complement activation and tissue damage [47].
Across platforms, clearance follows the rules of concentration and contact time. In acute cardiovascular care, integration into tMCS circuits and CRRT allows for early treatment. Outside of cardiovascular applications, hemoadsorption has been studied for use in septic shock, acute respiratory distress syndrome (ARDS) requiring venovenous extracorporeal membrane oxygenation (VV-ECMO), and in liver failure, rhabdomyolysis, and certain types of intoxication.
6. Clinical Evidence for Extracorporeal Cytokine Adsorption
6.1. Extracorporeal Cytokine Adsorption in CS- and tMCS-Supported Conditions
Beyond haemodynamic compromise, patients with CS frequently develop a systemic inflammatory response that contributes to vasoplegia, microcirculatory dysfunction, and secondary organ failure, providing the rationale for adjunctive extracorporeal immunomodulation.
In this setting, non-selective cytokine adsorption using CytoSorb has been most thoroughly studied. Across observational and propensity-matched cohorts of tMCS-supported CS, integration into VA-ECMO and/or CRRT has been associated with early improvements in haemodynamics and metabolic markers, including reductions in vasoactive–inotropic score (VIS), lactate, and inflammatory/organ injury markers such as CRP and procalcitonin (PCT) [11,48,49] (Table 1).
Although mortality remains high in refractory CS, in some cohorts, observed mortality was lower than predicted by risk scores; these descriptive comparisons are hypothesis-generating and cannot imply a causal treatment effect, and consistent survival benefit has not been demonstrated [45]. Feasibility and safety in complex extracorporeal settings have also been supported by broader single-centre experience and ECMO-focused reviews discussing implementation, controversies, and challenges [53,54,55]. Selected case reports further illustrate use in inflammatory cardiomyopathies and biventricular failure [56].
oXiris has been evaluated as an alternative adsorption platform in tMCS-supported CS, particularly in VA-ECMO populations. Evidence is limited to small, randomized studies showing transient reductions in inflammatory activity and vasoactive requirements (e.g., IL-6, VIS), without improvements in ECMO duration, weaning, organ dysfunction scores, or short-term survival [50,51]. Overall, current data do not support routine use of oXiris in tMCS-supported CS.
Selective C-reactive protein apheresis with PentraSorb has mainly been studied in cases of AMI cohorts. Although this method allows for quick and targeted removal of circulating CRP and shows biological effectiveness, clinical evidence is limited [52,57]. Its importance for the wider group of tMCS-supported CS patients seems minimal compared to non-selective cytokine adsorption strategies.
6.2. Extracorporeal Cytokine Adsorption in PCAS
Clinical evidence for cytokine adsorption in PCAS remains limited and inconsistent. Across available studies, non-selective adsorption with CytoSorb has been technically feasible and generally safe, both as stand-alone hemoperfusion and when integrated into VA-ECMO circuits during eCPR [13] (Table 2). In some cohorts, treatment was associated with reductions in inflammatory mediators, most notably IL-6, indicating biological activity [58]. Mechanistic data from eCPR populations further suggest that hemoadsorption may modulate leukocyte and platelet activation pathways, supporting target engagement beyond cytokine kinetics [59]. However, these signals have not translated into consistent improvements in haemodynamics, neurological recovery, or survival. Importantly, available observational data and randomized trials suggest that indiscriminate early use in unselected PCAS populations may be ineffective, and some datasets report an association with worse outcomes [60]. A plausible explanation is phenotype mismatch and timing: very early routine use in unselected patients may dilute any effect, whereas late initiation in advanced multiorgan failure may be biologically too late to modify outcomes. Registry-based analyses reported higher short-term mortality with early routine application, and randomized trials in eCPR patients did not demonstrate benefits in vasopressor requirements, markers of organ injury, or survival (Table 2). Taken together, current evidence supports feasibility and biological activity in selected patients but does not provide a consistent indication of clinical benefit on neurological outcomes or survival.
6.3. Extracorporeal Cytokine Adsorption in Septic Shock, Acute Respiratory Distress Syndrome, Rhabdomyolysis and Cardiac Surgery
Beyond acute cardiovascular syndromes, extracorporeal adsorption has been most extensively studied in sepsis and septic shock. In this context, CytoSorb has the most comprehensive clinical evidence and has been associated with reproducible short-term physiological effects, while a consistent survival benefit has not been demonstrated [61,62,63] (Table 3). Evidence for membrane-based adsorption systems such as oXiris is largely confined to septic shock with concomitant acute kidney injury during CRRT; small randomized and observational studies report reductions in inflammatory markers and vasopressor demand, but effects on mortality and duration of organ support remain inconsistent [64,65] (Table 3). Data supporting oXiris in ARDS are limited and have not shown robust clinical benefit beyond short-term physiological signals [66,67].
For rhabdomyolysis, registry data from the international prospective COSMOS registry suggest effective and safe reduction in very high myoglobin levels with CytoSorb, with concomitant improvement in creatinine and no serious device-related adverse events [78].
Selective CRP removal using PentraSorb has primarily been evaluated in cardiovascular indications; outside this context, extracardiac evidence remains scarce and has not demonstrated an impact on clinically relevant endpoints.
Other platforms (e.g., HA330/380 resin cartridges, endotoxin-directed adsorption, and pathogen-binding filters such as Seraph^®^ 100) show biological activity in selected sepsis-related cohorts, but robust outcome data are lacking.
In addition, hemoadsorption has been investigated in perioperative cardiac surgery during cardiopulmonary bypass (CPB), where contact activation can trigger a SIRS-like inflammatory response and vasoplegia. However, across a pilot RCT and subsequent observational data, intraoperative CytoSorb integrated into the CPB circuit has shown inconsistent effects on cytokine kinetics and has not translated into reproducible improvements in clinically relevant endpoints [79,81]. The largest randomized evidence in active infective endocarditis surgery (REMOVE trial) was neutral for postoperative organ dysfunction and 30-day mortality despite lower cytokine levels at the end of CPB [80].
Overall, extracardiac and perioperative data reinforce that adsorption therapies exert measurable biological effects, yet clinical relevance is indication- and phenotype-dependent and does not support routine use.
7. Practical Aspects in Extracorporeal Cytokine Adsorption: Patient Selection, Timing, and Dosing
In acute cardiovascular care, hemoadsorption should be used as a time-critical, phenotype-guided adjunct within an optimized shock bundle. Candidate selection is trajectory-based: persistent vasoplegia with lactate non-clearance despite correction of the precipitating cause, technically adequate tMCS support, and optimized ventilation and volume strategy. A pragmatic treatable phenotype includes escalating vasoactive–inotropic requirements, metabolic non-clearance, and objective inflammatory activation. Initiation should be early after refractory shock persistence is recognized and competing causes have been excluded (e.g., bleeding, tamponade, inadequate unloading/flows, uncontrolled infection source, limb ischaemia). Treatment is typically provided in brief cycles involving standardized cartridge exchanges. Continued treatment depends on an early physiological response. Assessment of the response should be explicit and time-bound. This trajectory-based framework conceptualizes treatment as a sequence of defined therapeutic phases—initiation, early response assessment, and discontinuation—rather than a fixed-duration intervention (Figure 3). Meaningful response is suggested by a clear reduction in vasoactive support accompanied by improved lactate/acid-base status and stabilization of fluid balance and urine output within 24–48 h; in the absence of such a signal, early discontinuation should be favoured. Given the potential co-adsorption of hydrophobic/protein-bound drugs, protocols should address antimicrobial exposure and critical antiplatelet/anticoagulant/sedative dosing, including timing around cartridge changes and therapeutic drug monitoring when feasible [82]. The extent of clinically relevant drug removal is variable and remains incompletely characterized across settings, highlighting the need for therapeutic drug monitoring with feasible and standardized pharmacokinetic reporting in future trials. Safety monitoring should include circuit function and clotting, bleeding risk, hemolysis markers, and platelet trends. Since thrombocytopenia and hypoalbuminemia have been reported during extracorporeal therapies, platelet counts, and serum albumin levels should be monitored regularly [83].
8. Limitations
As a narrative review, this work is inherently selective and does not aim to be exhaustive. The current literature on extracorporeal hemoadsorption in acute cardiovascular intensive care is constrained primarily by study design and interpretability. Most data originate from retrospective, single-centre cohorts with small sample sizes. Propensity-based comparisons in these studies remain vulnerable to residual confounding factors and treatment selection effects, particularly in device-supported shock. Co-interventions in this setting vary substantially and may dominate outcomes. Even when short-term physiological signals are reported, randomized evidence in closely related settings such as eCPR/PCAS has not shown consistent benefit on patient-centred endpoints and has raised concern for harm when applied indiscriminately in unselected populations. Moreover, extracorporeal cytokine adsorption is not a single class intervention: CytoSorb, oXiris, and PentraSorb differ fundamentally in adsorption spectrum, kinetics, and circuit integration, limiting cross-device extrapolation and complicating synthesis across studies. Mechanistic studies support biological target engagement, but these signals remain only loosely linked to durable clinical outcomes.
Finally, the net clinical effect is difficult to quantify because non-selective adsorption may alter exposure to anti-infectives and other protein-bound drugs, and extracorporeal therapies may coincide with thrombocytopenia and hypoalbuminemia; standardized pharmacokinetic reporting, safety signal adjudication, and validated enrichment strategies (biomarker thresholds or composite phenotype definitions) are still lacking, limiting reproducibility and the precise identification of patients most likely to benefit. Future studies should predefine and report drug classes at risk (e.g., anti-infectives, antiplatelets, sedatives), timing relative to cartridge exchanges, and—where feasible—therapeutic drug monitoring to enable comparability and safety interpretation.
9. Conclusions and Future Perspectives
Extracorporeal cytokine adsorption is a biologically plausible adjunct in acute cardiovascular shock syndromes in which immune–endothelial dysregulation contributes to vasoplegia and impaired tissue perfusion despite macrocirculatory stabilization. Across CS-, PCAS-, and tMCS-supported states, the available literature supports feasibility and short-term physiological effects in selected patients but does not justify routine use because consistent benefit on patient-centred outcomes has not been demonstrated. Accordingly, extracorporeal cytokine adsorption should be considered only as a selective, time-limited adjunct within multimodal shock care, guided by a clearly defined refractory, hyperinflammatory phenotype and continued only when an early, measurable physiological response is observed. In clinical practice, these principles translate into a structured set of indications and boundaries that emphasize selective use, early reassessment, and avoidance of indiscriminate application (Figure 4). Neutral or negative trial results may reflect phenotype mismatch, timing outside a therapeutic window (too early in unselected patients or too late in irreversible multiorgan failure), competing drivers of shock (e.g., inadequate unloading/flows, bleeding, ongoing ischemia), and variability in treatment “dose” and circuit integration. Future adequately powered, phenotype-enriched randomized trials are needed to define optimal timing and dosing and to evaluate clinically meaningful endpoints, including safety and drug-exposure effects.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berg D.D. Bohula E.A. Van Diepen S. Katz J.N. Alviar C.L. Baird-Zars V.M. Barnett C.F. Barsness G.W. Burke J.A. Cremer P.C. Epidemiology of Shock in Contemporary Cardiac Intensive Care Units Circ. Cardiovasc. Qual. Outcomes 201912 e 00561810.1161/CIRCOUTCOMES.119.00561830879324 PMC 11032172 · doi ↗ · pubmed ↗
- 2Hunziker L. Radovanovic D. Jeger R. Pedrazzini G. Cuculi F. Urban P. Erne P. Rickli H. Pilgrim T. the AMIS Plus Registry Investigators Twenty-Year Trends in the Incidence and Outcome of Cardiogenic Shock in AMIS Plus Registry Circ. Cardiovasc. Interv.201912 e 00729310.1161/CIRCINTERVENTIONS.118.00729330943781 · doi ↗ · pubmed ↗
- 3Sterling L.H. Fernando S.M. Talarico R. Qureshi D. van Diepen S. Herridge M.S. Price S. Brodie D. Fan E. Di Santo P. Long-Term Outcomes of Cardiogenic Shock Complicating Myocardial Infarction J. Am. Coll. Cardiol.20238298599510.1016/j.jacc.2023.06.02637648357 · doi ↗ · pubmed ↗
- 4Lüsebrink E. Binzenhöfer L. Adamo M. Lorusso R. Mebazaa A. Morrow D.A. Price S. Jentzer J.C. Brodie D. Combes A. Cardiogenic shock Lancet 20244042006202010.1016/S 0140-6736(24)01818-X 39550175 · doi ↗ · pubmed ↗
- 5Kologrivova I. Kercheva M. Panteleev O. Ryabov V. The Role of Inflammation in the Pathogenesis of Cardiogenic Shock Secondary to Acute Myocardial Infarction: A Narrative Review Biomedicines 202412207310.3390/biomedicines 1209207339335587 PMC 11428626 · doi ↗ · pubmed ↗
- 6Dettling A. Weimann J. Sundermeyer J. Beer B.N. Besch L. Becher P.M. Brunner F.J. Kluge S. Kirchhof P. Blankenberg S. Association of systemic inflammation with shock severity, 30-day mortality, and therapy response in patients with cardiogenic shock Clin. Res. Cardiol.202411332433510.1007/s 00392-023-02336-837982862 PMC 10850174 · doi ↗ · pubmed ↗
- 7Nolan J.P. Neumar R.W. Adrie C. Aibiki M. Berg R.A. Böttiger B.W. Callaway C. Clark R.S. Geocadin R.G. Jauch E.C. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication Resuscitation 20087935037910.1016/j.resuscitation.2008.09.01718963350 · doi ↗ · pubmed ↗
- 8Stub D. Bernard S. Duffy S.J. Kaye D.M. Post cardiac arrest syndrome: A review of therapeutic strategies Circulation 20111231428143510.1161/CIRCULATIONAHA.110.98872521464058 · doi ↗ · pubmed ↗