Action Observation and Motor Imagery in Children with Developmental Coordination Disorder: A Systematic Review
Elisa De Masi, Giovanni Morone, Giorgia Bruschi, Maria Paola Colatei, Martina D’Arienzo, Giulia Pezzetta, Irene Ciancarelli, Alex Martino Cinnera

TL;DR
This review examines how action observation and motor imagery might help children with coordination difficulties improve their motor skills and daily activities.
Contribution
The study is the first systematic review to evaluate AO and MI interventions for children with Developmental Coordination Disorder.
Findings
AO and MI interventions showed improvements in motor planning and coordination in children with DCD.
Functional task performance and daily living activities improved with these mental training approaches.
VR-based combinations of AO and MI show promise but require further investigation.
Abstract
Background and Objectives: Children with Developmental Coordination Disorder (DCD) show substantial motor and balance difficulties that affect daily activities. Although action observation (AO) and motor imagery (MI) are effective in other neurological conditions, their impact in DCD remains underinvestigated. This review explores the preliminary evidence of AO- and MI-based interventions for improving motor and functional outcomes in children with DCD. Methods: A systematic search of PubMed, Scopus, and Web of Science identified randomized controlled trials and controlled trials published in the last 15 years evaluating AO and MI interventions in children with DCD. Two independent reviewers conducted the screening of the studies, data extraction, and the risk-of-bias assessment using RoB2 and ROBINS-I. The review followed PRISMA reporting guidelines and was pre-registered on the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
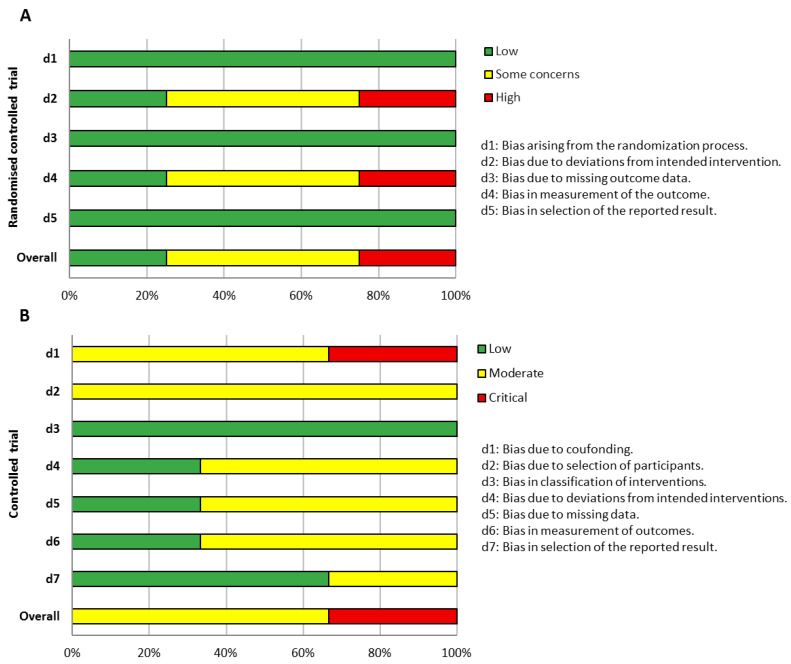 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChildren's Physical and Motor Development · Sport Psychology and Performance · Action Observation and Synchronization
1. Introduction
Children diagnosed with Developmental Coordination Disorder (DCD) exhibit difficulties in acquiring age-appropriate motor skills, despite the absence of any general medical condition, pervasive developmental disorder, or intellectual disability [1]. These motor deficits substantially interfere with the activities of daily living (ADLs) such as hygiene, schoolwork, social participation, and sports [2]. A primary motor control issue in DCD is impaired balance, with reports indicating that up to 87% of affected children experience balance difficulties [3,4]. Motor deficits are often also associated with deficits in motor imagery (MI) in children with DCD [5], especially in complex task constraints [6,7]. MI, which involves the mental simulation of a movement without any physical execution or muscle activation, and action observation (AO), which entails watching another individual perform a movement, both engage brain regions similar to those activated during the actual movement and may play an equivalent role in motor learning [8]. Mirror neurons, first identified in the premotor cortex of monkeys [9], are thought to support a mirror mechanism that maps observed actions onto the neural substrates responsible for their execution [10]. This mechanism enables an experiential understanding of others’ actions through the reactivation of motor representations, a process that also occurs during MI, when movements are mentally reproduced. Increasing neuroscientific evidence suggests that motor simulation techniques share this neural basis and contribute to motor learning. Based on neuroscientific evidence, AO and MI have been widely used as therapeutic interventions to address motor impairments across a range of neurological disorders, with generally positive effects reported. Indeed, recent literature reviews consistently highlight the positive effects of these rehabilitative approaches on motor and functional outcomes, particularly in populations affected by Parkinson’s disease and stroke [11,12,13,14]. Although children with DCD have been shown to present alterations in MI abilities, particularly under complex task constraints, and despite the well-documented effectiveness of AO- and MI-based interventions in other neurological disorders, no systematic reviews have yet evaluated their efficacy as rehabilitative approaches in this population. In fact, current evidence remains limited, with small sample sizes and substantial heterogeneity in intervention protocols and study procedures. The aim of the present systematic review is to explore and summarize the latest findings regarding the use of AO and MI, or their combination, in the treatment of motor, balance, or functional impairment in children diagnosed with DCD.
2. Materials and Methods
To explore the most recent evidence on the effects of AO and MI training on motor functions in children with DCD, we conducted a systematic search of articles indexed in PubMed, Scopus, and Web of Science (WOS) published over the past 15 years, a time frame chosen to reflect methodological and technological advancements in mental training for this pediatric population (search strategy is available in Table S1). Studies were selected based on the following criteria: (1) participants under 18 years of age; (2) a clinical diagnosis of DCD; (3) intervention based on AO and/or MI therapy; (4) randomized controlled trials (RCTs) or controlled trials (CTs); (5) studies published in English to ensure a wide range of high-impact international scientific literature.
Exclusion criteria were as follows: (1) studies involving adult participants or mixed-age samples without separate pediatric data; (2) studies in which AO or MI was not the primary intervention; (3) non-interventional study designs (e.g., observational studies, case reports, reviews, or expert opinions); (4) articles not available in full text; and (5) articles not published in peer-reviewed journals. All retrieved articles were imported into an online database [15] and independently screened by two reviewers based on title and abstract. Discrepancies were resolved through discussion with a third reviewer to achieve consensus. The same procedure was applied during the full-text evaluation. The reporting followed the PRISMA statement. The protocol was pre-registered on PROSPERO database (CRD420251084196) on 21 January 2025.
2.1. Data Extraction
The data from the selected studies were independently extracted by two authors and organized to provide a clear and structured synthesis of the available evidence. The extracted information was grouped into several key categories. Bibliometric data included the author(s), year of publication, and country of origin. Methodological characteristics comprised the study design and its corresponding level of evidence. Details about the study population were also recorded, including sample size, sex distribution, and participants’ age range. Information related to the intervention covered the duration and nature of the treatment, as well as the composition of both experimental and control groups. Inclusion and exclusion criteria were noted to better understand the population under investigation. Furthermore, details regarding the measurement tools and the timing of outcome evaluations were collected. The measures of effect were reported using statistical significance (p-values) and, when available, effect sizes, including Cohen’s d, r, or η^2^, depending on the metrics provided in the original studies. Finally, the main findings and conclusions reported by the authors were summarized. This comprehensive and structured approach allowed for a thorough overview of each study, facilitating comparison across trials and supporting a critical appraisal of the current body of evidence.
2.2. Risk of Bias Assessment
The risk of bias of included studies was assessed using the Cochrane risk of bias tool version 2 (RoB2) and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I), for RCT and CT, respectively, by two blinded assessors. The overall risk of bias (RoB) for each study was categorized as low, moderate, or high quality based on the number and severity of the identified biases across relevant domains. Studies were classified as low risk (high quality) if all domains were judged to have a low risk of bias; as moderate risk (moderate quality) if at least one domain had unclear or moderate risk but none were high; and as high risk (low quality) if one or more domains were deemed to have a high risk of bias.
3. Results
After the initial search, 320 records were identified. Following the removal of 89 duplicates, 231 articles were screened by title and abstract. Of these, 223 underwent full-text assessment, and ultimately 7 studies met the inclusion criteria [16,17,18,19,20,21,22] (Figure S1). The included studies were published between 2016 [16] and 2023 [22]. Most studies were conducted in the United Kingdom [20,21,22] and Australia [16,18], of which four are RCTs [16,19,20,22] and three are CTs [17,18,21]. Marked heterogeneity was observed across the included studies, arising from differences in participant characteristics (confirmed versus suspected DCD), intervention dosage (single-session versus cumulative training), control conditions (active, passive, or within-group comparisons), and the use of both proximal and distal outcome measures to assess intervention effects.
3.1. Population
The included studies enrolled a total of 199 (28.4 ± 12.1) children diagnosed with DCD, ranging from a minimum of 8 patients [17] to a maximum of 42 [16]. The included studies involved children with an age range from 5 to 12 years old. In the studies that reported sex among included children [17,18,19,20,22] a balanced distribution was observed (male 52.9%; female 47.1%). All participants met the DSM-5 diagnostic criteria for DCD; two of the included studies also recruited in their trial children with suspected DCD, who were screened before they started the training using measurement tools such as MABC-2 (Movement Assessment Battery for Children Second Edition) and DCDQ (Developmental Coordination Disorder questionnaire) specifically made for assessing children with perturbations of the motor skills or coordination in early ages, before the diagnostic process [20,22]. Yet these children present the same deficits as children with DCD diagnosis, so the choice to include them, at an early stage of the development, into a targeted trial is decisive to prevent or reduce the development of more advanced symptoms (detailed information of included studies is reported in Table 1).
3.2. Intervention
Three studies implemented a single-session intervention in which children completed the trials in predefined blocks [18,20,21]. The remaining studies delivered training over multiple sessions, with frequencies ranging from once per week [16,17] to four times per week [22]. Overall, the total number of sessions varied considerably, from a single session [18,20,21] to sixteen sessions [19,22], with an average of 6.3 ± 6.8 sessions. In studies with multiple sessions, the total study duration ranged from four weeks [22] to nine weeks [17], with a mean duration of 4.1 ± 3.4 weeks across studies [17,19,22]. Among the four studies clearly reporting session length, AO + MI activities lasted between 10 min and 1 h. Across the included studies, MI training typically involved guided internal rehearsal of both functional and sport-related movements. Participants engaged in kinesthetic or visual imagery scripts tailored to everyday tasks (such as shoelace tying, cutlery use, shirt buttoning, and cup stacking) [22] or to broader fundamental motor skills including catching and throwing a tennis ball, striking a softball, jumping to a target, balancing a ball while walking, and placing objects on a form board [16]. In several cases, MI was combined with periods of overt practice to help refine internal motor representations. AO and combined AO + MI approaches used video demonstrations to support motor learning; participants viewed examples of conventional performance strategies [22] or observed first-person videos showing the progression of a novice learning a visual-motor rotation task [20] while simultaneously generating kinesthetic imagery. In AO + MI protocols, observation was systematically followed by physical execution (for example, guiding a stylus-controlled cursor to sequential visual targets) to promote continuous updating of the internal model. Some studies implemented immersive game-based or virtual reality training (VR training) [19], where participants selected interactive games (e.g., mini-baseball, basketball, bowling, soccer) designed to challenge object-control and manipulative skills including throwing, catching, dribbling, kicking, and striking. A structured, multicomponent format was adopted in Adams and colleagues (2017) [17], where each session combined goal setting, third- and first-person action observation, mental rehearsal, overt practice, and alternation between imagery and execution with guided reflection. Specific object-manipulation paradigms were also used [18]; participants grasped and rotated an octagonal dial to match color sequences, either performing the movements directly or first imagining how they would grasp and rotate the object before acting. Finally, Scott and colleagues [21] employed an imitation-based approach in which participants viewed a brief static image followed by a video of a rhythmic action and then reproduced the movement while 3-D kinematics were recorded. Across the included studies, most interventions were preceded by a pre-test phase used to familiarize participants with the task demands and to establish a baseline level of performance. These pre-tests typically involved brief demonstrations, exposure to the task environment, or completion of initial trials to ensure that subsequent training effects could be interpreted relative to a clearly defined starting point.
3.3. Control
Across the selected studies, several control conditions were used, including no intervention, typically developing controls, and alternative rehabilitative approaches. Other studies used active but non-specific controls, for example, children played games that were unrelated to the targeted ADLs to match engagement and screen time without training the target skills [22]. A commonly used sensory-control was viewing neutral video content [20]; participants watched clips of a nature documentary that contained no human motor content, with clip duration chosen so total viewing time equaled that of the AO + MI videos. Finally, some studies compared interventions to structured alternatives such as CO-OP (Cognitive orientation to daily occupational performance; goal-directed training), which typically included goal discussion and planning, practice using the Goal-Plan-Do-Check framework, and homework/parent guidance [17]. Several studies therefore balanced time, attention, and physical practice across groups to isolate the specific effects of AO, MI, or AO + MI.
3.4. Outcome
Assessment tools encompass a range of proximal and distal motor outcomes, which can be mapped on key IMD processes (i.e., predictive control, forward modeling, motor planning, and end-state comfort). Standardized tests such as the MABC and MABC-2, as well as the DCDQ, were most frequently used (Table 2). The MABC/MABC-2 evaluates global motor coordination, including manual dexterity, reaching/grasping, and balance, representing distal functional outcomes, whereas the DCDQ, a parent-report questionnaire, served both as a screening tool for motor difficulties and for group allocation. Several studies employed tasks specifically targeting proximal IMD-related processes such as motor imagery and action planning. More specifically, these processes included the hand rotation task to assess mental rotation and internal action representation; anticipatory action planning tasks to evaluate predictive control and to sequence with respect to end-state comfort; and rapid online control tasks to measure forward modeling and adaptive corrections during goal-directed actions. Performance-based measures further included assessments of ADLs, evaluating both execution quality and movement technique, as well as completion time and target-locking scores in visuomotor tasks, thereby bridging proximal IMD processes and distal functional skills. Some studies additionally analyzed movement kinematics using three-dimensional motion capture to quantify spatial and temporal parameters of movement, offering more accurate insights into underlying control mechanisms. Complementary instruments, such as the MIQ-C and MCQ, assessed imagery ability and perceived motor competence, while the NDI evaluated neuromuscular development in younger children. Together, these measures allowed a comprehensive evaluation of motor function, spanning internal representations, predictive planning, and forward control mechanisms through to overall coordination and performance in everyday activities.
3.5. Evidence Synthesis
Across multi-session intervention studies [16,17,19,22] (three RCTs and one CT), statistically significant improvements were observed on a range of motor outcomes compared to control or baseline conditions. In standardized motor assessments, intervention groups showed greater pre–post gains compared to controls (p = 0.03; r = 0.70–0.84), corresponding to large effect sizes, but with no significant differences between active interventions (p = 0.95) [16]. Similarly, significant group × time interactions were found for MI (p = 0.039, η^2^ = 0.16) and action planning (p = 0.027, η^2^ = 0.17), with the experimental group outperforming the control group at post-test and follow-up. Significant interaction effects were also reported for online anticipatory action control, total time on target (p < 0.001, η^2^ = 0.47), consecutive time on target (p < 0.001, η^2^ = 0.44), and distance from target (p = 0.001, η^2^ = 0.22), indicating improvements in the experimental group from pre- to post-test that were maintained at follow-up [19]. Significant group × time interactions, pre–post comparison and retention were observed for functional motor tasks, including shoelace tying (p = 0.018; post-test p = 0.045, technique p = 0.002, retention p = 0.011), and cup stacking (post-test p = 0.008, retention p = 0.01) [22]. Within-group significant results were also observed in the shirt buttoning (post-test: p = 0.002, retention: p = 0.001), and cutlery use (post-test: p = 0.026, retention: p = 0.001). Finally, based on descriptive statistics of Adams and colleagues (2017) [17], clinically meaningful improvements were also observed on the MABC-2 scores in both the experimental and active control groups.
Across single-session imagery-based investigations [18,20,21], significant improvements were reported on various motor and predictive control outcomes. Increases in movement efficiency and reductions in suboptimal strategies were observed (p ≤ 0.014) [18]. Significant group × time interactions were observed for completion time (p = 0.009) and target-locking scores (p ≤ 0.012), confirming better post-test performance in the AO-MI group compared with control group [20]. Finally, imitation performance improved following combined imagery-based instructions compared with motor imagery alone (p = 0.021). However, differences relative to simple imitation in children with DCD were not consistently significant (p = 0.236) [21].
3.6. Methodological Reporting Adherence
In the assessment of reporting quality, adherence to the intervention and the measurement of variability in participant outcomes were the domains most frequently identified in the RCTs (Figure 1A). Item-level analysis indicated that these aspects were commonly related to the allocation to the experimental group and to the implementation of blinding procedures, reflecting characteristics of the experimental designs employed. Notably, a high risk of bias in these domains suggests that deviations from intended interventions and potential bias in outcome assessment may have influenced the results, limiting confidence in the observed effects and supporting a cautious interpretation of the findings.
For the CT studies, most investigations were classified as having an elevated overall risk of bias (Figure 1B). Across the included studies, there was limited control of confounding factors, such as age, severity of DCD, and comorbidities, and variability in adherence to the intervention and heterogeneity in outcome measures were observed. These issues reflect the lack of randomization and differences in participant selection procedures, which may have led to an overestimation of the reported intervention effects.
4. Discussion
The present systematic review explored the preliminary evidence of the effects of AO and MI therapies in the improvement of motor functions in children with DCD. The results suggest that mental training, particularly MI and its combination with AO, may be feasible and potentially beneficial for enhancing motor planning, coordination, and execution in ADL compared with control conditions. However, the heterogeneity across experimental procedures and the potential risk of bias impose caution when interpreting the magnitude of effects. Moreover, compared to active control interventions, effects were generally not statistically significant, suggesting that these approaches may be considered as add-on treatments.
Nevertheless, while preliminary and heterogeneous, the results suggest that motor simulation techniques may contribute to reducing motor control and coordination difficulties by engaging mechanisms potentially related to the mirror neuron system, thereby facilitating the reactivation of motor representations that could partially compensate for difficulties in generating internal forward models during physical execution.
However, these findings should be interpreted with caution. Although the findings are broadly consistent with the IMD framework, suggesting that mental training may influence aspects of predictive motor control in children with DCD [16,20], the current evidence does not support causal inferences, and the IMD rationale should be regarded as a plausible interpretative model rather than a definitively established explanatory mechanism. MI alone can support MP by encouraging children to use the end-state-comfort strategy more and enhance their motor skills, as shown in some included studies [16,18]. Indeed, when combining AO and MI, the benefits seem to increase, not only in the imitation of everyday actions (e.g., in the ADLs) [21,22] but also in adapting the visual system and neuro-motor system during complex tasks [20]. Therefore, combining AO and MI appears to offer potential benefits beyond those of single modalities (AO or MI). In fact, the simultaneous observation of an external guide to the internal kinesthetic simulation leads to a more robust internal model and to an improvement of the eye–hand coordination. The studies included in this review support the hypothesis that DCD rehabilitation should extend beyond physical practice to incorporate strategies aimed at strengthening internal motor representations and addressing deficits in internal modeling. Nevertheless, evidence on the combined use of AO and MI remains speculative due to the limited number of direct comparisons. Regarding distal outcomes, the most positive effects reported were observed through standardized measurement tools such as the MABC (or MABC-2) and DCDQ, which assess motor skills while providing a practical, everyday perspective on children’s difficulties in their environmental context. Other improvements were also registered through less standardized tools such as general motor performances in everyday tasks (ADLs) and imitation skills [17,21,22].
The present review suggests that AO and MI interventions in addition to conventional training are feasible and they might be delivered in various settings: clinical (inpatient, outpatient) and environmental (e.g., school, home) with a caregiver [17,19]. Interestingly, AO and MI might be delivered through virtual reality scenarios or exergaming, offering the possibility to increase the engagement and the participation [23]. Although explorative, the use of virtual reality can provide augmented sensory feedback (which plays a key role in functional changes associated with neuroplasticity) [24], and enhances the embodiment and allocentric perception of movement in children affected by neurodevelopmental disorders [25].
Limitations
A major limiting factor in the studies here reviewed is the small sample size, with only three adopting active control conditions, which ensured better comparability. The use of mixed samples, with unclear proportions of formally diagnosed children in some studies, also introduces diagnostic uncertainty that may affect internal validity and limit generalizability [20,22]. Moreover, the effects of studies implementing a single training session were combined with those using cumulative interventions, and in studies including typically developing children as a control group, effects were primarily estimated from within-group changes. In studies with multiple experimental groups, changes in the AO and MI groups were primarily compared with control groups rather than with other experimental conditions. Outcomes combined both proximal measures (e.g., motor planning, imagery, task performance) and distal measures (e.g., overall coordination, ADLs), which may affect the distinction between direct intervention and broader functional effects. Moreover, the inclusion of different study designs (RCTs and CTs) further limits confidence in causal inferences and the robustness of the observed effects, thereby weakening the strength of the conclusions. Overall, the risk of bias across studies was moderate-to-high, mainly due to outcome measurement, deviations from intended interventions, confounding, and participant selection. Future research should address these issues through blinded assessments, stricter intervention adherence, improved control of confounders, and clearer participant selection criteria. Finally, gray literature and unpublished studies were not included in the present review, which may increase the risk of publication bias, as studies with non-significant or negative results are less likely to be published, potentially leading to an overestimation of the reported intervention effects.
5. Conclusions
This systematic review indicates that AO and MI, whether applied individually or in combination, are feasible and may support motor planning, coordination, and execution in children with DCD. Their combination appears to offer a complementary approach that could further facilitate recovery by enhancing imitation, visuomotor integration, and eye–hand coordination. These interventions can be implemented in clinical or naturalistic settings and may be integrated with other technologies, including virtual reality, to promote improvements in both proximal and distal outcomes, such as motor skills and activities of daily living (ADL). However, evidence remains limited and heterogeneous. Small sample sizes, varying intervention designs, and the high risk of bias can reduce confidence in the results. Consequently, while motor simulation techniques appear promising as adjunctive interventions, current evidence is still preliminary. Further trials are required to support their effectiveness and to clarify optimal delivery strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adams I.L. Lust J.M. Wilson P.H. Steenbergen B. Compromised motor control in children with DCD: A deficit in the internal model?—A systematic review Neurosci. Biobehav. Rev.20144722524410.1016/j.neubiorev.2014.08.01125193246 · doi ↗ · pubmed ↗
- 2Blank R. Barnett A.L. Cairney J. Green D. Kirby A. Polatajko H. Rosenblum S. Smits-Engelsman B. Sugden D. Wilson P. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder Dev. Med. Child Neurol.20196124228510.1111/dmcn.1413230671947 PMC 6850610 · doi ↗ · pubmed ↗
- 3Verbecque E. Johnson C. Rameckers E. Thijs A. van der Veer I. Meyns P. Smits-Engelsman B. Klingels K. Balance control in individuals with developmental coordination disorder: A systematic review and meta-analysis Gait Posture 20218326827910.1016/j.gaitpost.2020.10.00933227605 · doi ↗ · pubmed ↗
- 4Macnab J.J. Miller L.T. Polatajko H.J. The search for subtypes of DCD: Is cluster analysis the answer?Hum. Mov. Sci.200120497210.1016/S 0167-9457(01)00028-811471397 · doi ↗ · pubmed ↗
- 5Barhoun P. Fuelscher I. Kothe E.J. He J.L. Youssef G.J. Enticott P.G. Williams J. Hyde C. Motor imagery in children with DCD: A systematic and meta-analytic review of hand-rotation task performance Neurosci. Biobehav. Rev.20199928229710.1016/j.neubiorev.2019.02.00230753855 · doi ↗ · pubmed ↗
- 6Williams J. Thomas P.R. Maruff P. Wilson P.H. The link between motor impairment level and motor imagery ability in children with developmental coordination disorder Hum. Mov. Sci.20082727028510.1016/j.humov.2008.02.00818384899 · doi ↗ · pubmed ↗
- 7Noten M. Wilson P. Ruddock S. Steenbergen B. Mild impairments of motor imagery skills in children with DCD Res. Dev. Disabil.2014351152115910.1016/j.ridd.2014.01.02624636024 · doi ↗ · pubmed ↗
- 8Mulder T. Motor imagery and action observation: Cognitive tools for rehabilitation J. Neural Transm.20071141265127810.1007/s 00702-007-0763-z 17579805 PMC 2797860 · doi ↗ · pubmed ↗