Risk Factors Associated with the Emergence of Multidrug-Resistant Bacteria and Fungal Infections in Walled-Off Pancreatic Necrosis
Michael Fernandez Y Viesca, Alia Hadefi, Lukas Otero Sanchez, Martina Pezzullo, Morgane Van Wettere, Eleni Karakike, Maya Hites, Viviane De Maertelaer, Myriam Delhaye, Marianna Arvanitakis

TL;DR
This study identifies risk factors for multidrug-resistant bacteria in pancreatic infections, finding that antibiotic changes and nutritional support increase the risk.
Contribution
The study identifies independent risk factors for MDR bacteria emergence in infected pancreatic necrosis.
Findings
Antibiotic changes and nutritional support were independently linked to MDR bacteria emergence.
ICU admission rates were higher in patients with IPN and MDR infections.
Fungal infections showed no independent risk factors in this study.
Abstract
Background: Infected pancreatic necrosis (IPN) is a serious complication of moderate-to-severe acute pancreatitis (AP), associated with high morbidity, intensive care unit (ICU) admission, organ failure, and mortality. Initial management relies on antibiotics and drainage of walled-off necrosis (WON). In the context of increasing multidrug-resistant (MDR) bacteria, identifying risk factors for MDR emergence is crucial. The impact of fungal infections (FIs) on outcomes also remains unclear. This study aimed to identify risk factors associated with the emergence of MDR bacteria and FIs during intervention for IPN. Methods: This retrospective study included 71 consecutive patients undergoing intervention for suspected IPN or symptomatic WON. Results: At first intervention, IPN was confirmed in 52 patients (73%), MDR bacteria in 19 (27%), extensively drug-resistant (XDR) bacteria in 4…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
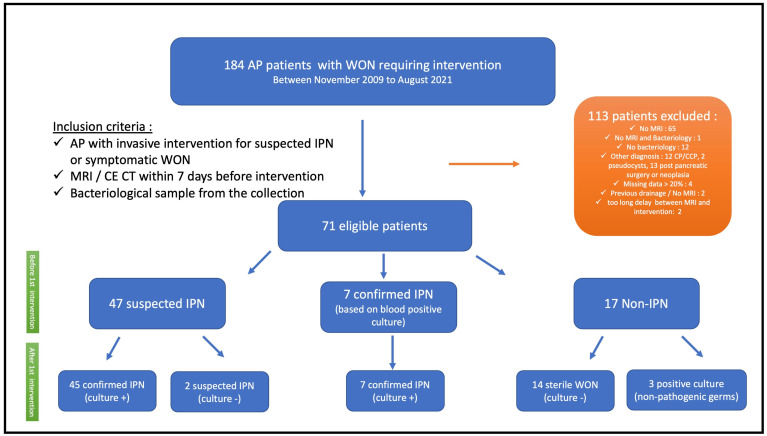 Figure 1
Figure 1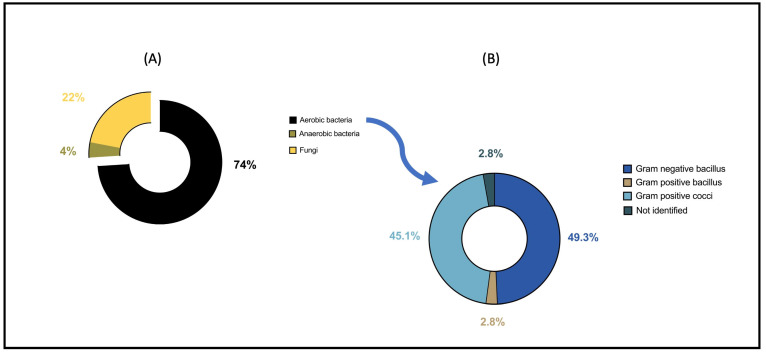 Figure 2
Figure 2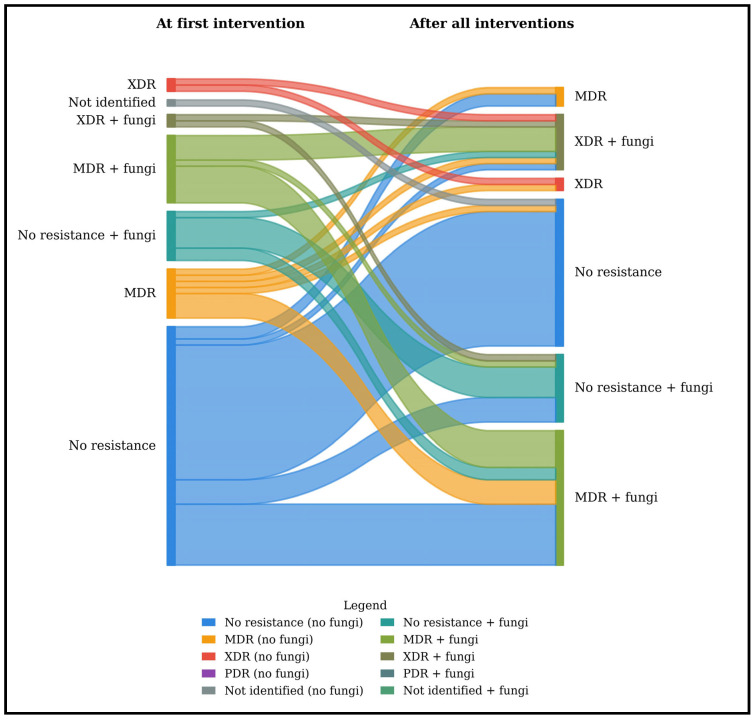 Figure 3
Figure 3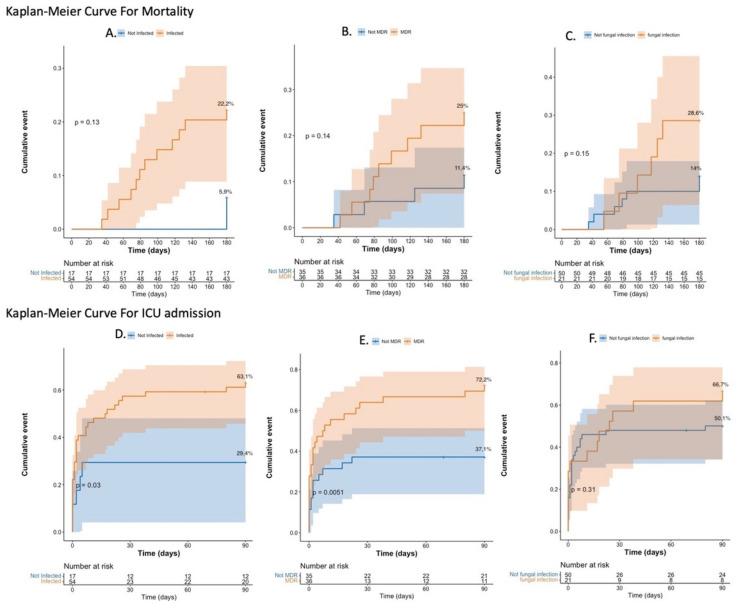 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Amoebic Infections and Treatments · Streptococcal Infections and Treatments
Key Summary:
Established knowledge of the subject
Significant and/or new findings of this study
1. Introduction
Acute pancreatitis (AP) is a common condition worldwide, and most patients have a rapidly favorable outcome [1,2]. However, 20% of patients will develop moderate-to-severe disease associated with the presence of necrotic pancreatic tissue [3]. These patients have a high risk of necrotic infection (up to 70%) [4]; two-thirds will need intervention [5], one-third will develop organ failure [6], and 15%–20% will die [7]. Infected pancreatic necrosis (IPN) results from disruption of the intestinal mucosal barrier, leading to increased permeability and bacterial/fungal translocation into pancreatic and peripancreatic necrotic tissue [8]. According to international guidelines, IPN requires management with antibiotics and minimally invasive interventions, including endoscopic and radiological drainage of collections (walled-off necrosis (WON)) [9,10,11]. Antibiotics play an important role in the conservative management of suspected and confirmed IPN [5]. However, the efficacy of previous antibiotic therapy for sterilizing infected collections or avoiding intervention is not well known [5,12]. Moreover, there are no clear recommendations concerning the type or duration of first-line antibiotic therapy nor the use of concomitant antifungal therapy [9,10,11]. In the era of multidrug-resistant bacteria (MDR) due to antibiotic overuse, microbiological data are of significant interest [13,14]. Also, although they are less frequent, the impact of fungal infections (FIs) on clinical outcomes has recently been highlighted, with reported incidences ranging from 7 to 46% in previous studies [15,16].
This study aimed to identify risk factors associated with the emergence of MDR bacteria during minimally invasive interventions for IPN and to identify factors associated with FI during the initial intervention for IPN. Secondary endpoints were to identify overall risk factors for IPN and to describe our local microbial epidemiology; the antibiotic therapy administered; and the natural course of selection towards MDR, extensively drug-resistant (XDR), and pan-drug-resistant (PDR) bacteria and their impact on disease outcomes (mortality and ICU admission rates).
2. Results
2.1. Characteristics of the Population
From November 2009 to August 2021, 184 patients with WONs requiring intervention for suspected IPN or other indications (e.g., pain and organ compression) were assessed for eligibility, and 71 patients were included in the study (Figure 1). The mean age was 51 ± 16 years, and the majority of patients were men (72%). Alcohol abuse and gallstones were the leading causes of AP in 38% and 33%, respectively. According to the Atlanta Classification, 45% were considered severe and 55% moderate. All patients underwent a first intervention with a median of 36 days (24–69) from the onset of symptoms, and endoscopic drainage was performed in all 71 patients. After the first intervention, fifty-two patients (73%) were considered to have confirmed IPN, including 7 patients with positive blood cultures without any other documented extra-pancreatic infection and 45 patients with positive cultures of fluid/necrosis collected during the first intervention. Two patients had suspected IPN (clinic/imaging suggestive of IPN but first culture negative), and seventeen patients (24%) had non-IPN (Figure 1). The characteristics of the included patients are detailed in Table 1.
2.2. Microbiological Culture and Antibiotics Before and After Intervention
Table 2 summarizes the results of microbiological and antibiotic characteristics of the population before the first intervention. In 56 patients (79%), antibiotics had been initiated for a median duration of 7 days (2–18) prior to the first drainage (92 periods of antibiotics: 67 cases (73%) were treated empirically and 25 (27%) based on a positive culture (e.g., blood culture)). Among these 56 patients, 29 patients (52%) and 27 patients (48%) received one or more than one antibiotic, respectively. Thirty-one patients (44%) were free from antibiotics for at least seven days before the first intervention. Of the remaining 40 patients who received antibiotics within seven days before the first intervention, five patients (12.5%) had sterile collections. The most frequently administered antimicrobial category was antipseudomonal penicillin + ß-lactamase inhibitor (33%), followed by penicillin + ß-lactamase inhibitor (28%) and carbapenem (15%). Other combinations of different classes of antibiotics are detailed in Table 2. Six patients received concomitant antifungal therapy before the first intervention, of whom one patient showed fungi in the culture obtained during the initial intervention.
Figure 2A,B and Supplementary Table S3 show the different microbiological agents isolated from the sample at the time of the first intervention. Among aerobic bacteria, Gram-negative bacilli (GNB) and Gram-positive cocci (GPC) represented 49% and 45% of the isolates, respectively. Among anaerobes, five strains were isolated (Fusobacterium nucleatum n = 2, Lactobacillus gasseri n = 1, Prevotella buccae n = 1, and Veillonella parvula n = 1). Fungi were isolated in 21 patients, mainly Candida albicans (n = 17, 81%), followed by Candida glabrata (n = 3, 14%) and Candida krusei (n = 1, 5%). Regarding antifungal susceptibility, all Candida albicans isolates were susceptible to fluconazole, except for one strain that was resistant to fluconazole and other triazoles (itraconazole, voriconazole, and posaconazole) but remained susceptible to caspofungin. Two of the three Candida glabrata isolates showed intermediate susceptibility to fluconazole but were susceptible to other antifungal classes. The Candida krusei isolate was resistant to fluconazole and itraconazole.
After the first intervention, all but one (99%) patient received antibiotics. Initial treatment mainly consisted of penicillin + ß-lactamase inhibitors (34%), antipseudomonal penicillin + ß-lactamase inhibitors (31%), and carbapenem (17%). The first-line antibiotic regimen was adequate according to bacterial susceptibility in 51/70 patients (73%). The only patient who did not receive antibiotics at the time of the first drainage had a negative culture. During follow-up, antifungal therapy was administered in 31/70 patients (44%) and always in combination with antibiotics. Antibiotic regimens were frequently modified according to microbiological results and clinical evolution, with a median of 2 adaptations (range 1–4) per patient. Overall, patients received a median of 4 (2–6) different antimicrobial agents, with a mean total duration of antibiotic therapy of 43 ± 30 days. These results are summarized in Table 3.
2.3. Risk Factors Associated with Emerging MDR
Figure 3 summarizes the distribution of bacterial resistance profiles at the first intervention and during follow-up in patients with WON. At the first intervention, the proportion of MDR and XDR bacteria was 26.8% and 5.6%, respectively, and this rose to 35.2% and 15.5%, respectively, during the follow-up intervention. No PDR bacteria were observed in this cohort. In logistic regression, risk factors associated with the emergence of MDR bacteria during the natural course of AP were analyzed (Table 4). In univariate analysis, prior exposure to antibiotics, the number of changes in antibiotics, ICU admission, size of the WON (length and width), the need for NS, AP duration, albumin levels, and total number of interventions ≥ 5 were associated with the emergence of MDR during the natural course of the disease. In multivariate analysis, only the number of changes in antibiotics (b, 1.70; 95% CI, 1.18–2.43; p = 0.004) and the need for NS (b, 5.69; 95% CI, 1.52–20.50; p = 0.010) were independently associated with the emergence of MDR bacteria.
2.4. Risk Factors Associated with FI
Figure 3 also presents the dynamics of fungal detection during the primary intervention and thereafter, during the course of the disease. Of the 21 patients identified to have an FI during the first intervention, four (19%) were resistant to fluconazole. A logistic regression to determine potential risk factors associated with FI at the first intervention was performed (Table 5). In univariate analysis, only the total number of interventions was significantly associated with FI (OR, 3.43; 95% CI, 1.2–10.22; p = 0.023).
Among the 42 patients with positive fungal cultures after all interventions, antifungal therapy was administered to 26 (62%), whereas five patients were treated while no fungi were detected.
2.5. Risk Factors Associated with Overall IPN
After a logistic regression, the two independent factors associated with the overall occurrence of IPN were prior exposure to antibiotics (b, 26.41; 95% CI, 1.90–366.38; p = 0.015) and prealbumin levels (b, 0.77; 95% CI, 0.63–0.94; p = 0.012) (Table 6)
2.6. Mortality and ICU Admission Rate Analysis
The observed mortality rate in this cohort was 18% (13 patients), all but one of them with IPN. The 180-day mortality rate (Figure 4A–C) was not significantly different between IPN and non-IPN patients: 22.2% (95% CI, 10.3%–32.6%) vs. 5.9% (95% CI, 0%–16.4%), p = 0.130; between MDR and non-MDR: 25% (95% CI, 9.4%–37.9%) vs. 11.4% (95% CI, 0.24%–21.4%), p = 0.140; and between FI and non-FI (at the first drainage): 28.6% (95% CI, 6.4%-45.5%) vs. 14% (95% CI, 3.8%–23.1%), p = 0.150. The 90-day cumulative ICU admission rate (Figure 4D–F) was significantly different between the IPN and non-IPN groups: 63.1% (95% CI, 47.7%–74%) vs. 29.4% (95% CI, 4.1%–48.1%), p = 0.030, and between MDR and non-MDR: 72.2% (95% CI, 53%–83.6%) vs. 37.1% (95% CI, 19%–51.3%), p = 0.005, but not significant between FI and non-FI (at the first drainage): 66.7% (95% CI, 39%–81.8%) vs. 50.1% (95% CI, 34.1%–62.2%), p = 0.310.
3. Discussion
To our knowledge, this is the first study to demonstrate a dynamic progression of the emergence of MDR bacteria throughout the course of subsequent interventions in IPN patients. Unlike previous studies that provide only a single-timepoint snapshot of MDR prevalence [14,17,18,19,20], these data show a clear temporal evolution: the incidence of MDR and XDR in IPN increased from 26.8% to 35.2% and from 5.6% to 15.5%, respectively, between the first and the final interventions.
These high incidences remain comparable to those reported in the most recent retrospective studies, where MDR rates range from 29.5% to 57.5% [14,17,18,19,20]. One explanation for these high incidence rates could be that these patients were treated in a tertiary center, specialized in treating this type of severe AP that requires multidisciplinary care. Another explanation could be that the severity of disease in our population was greater than that of other published cohorts, supported by the cumulative ICU admission rates, which were significantly higher in patients with IPN and MDR bacteria than in those with non-IPN and non-MDR bacteria. Moreover, ICU settings themselves may contribute to the emergence of MDR organisms due to factors such as prolonged antibiotic exposure, invasive procedures, and increased selective pressure in critically ill patients [18].
Although this study did not demonstrate any statistically significant difference in mortality between patients with and without MDR bacteria, as in the aforementioned studies [14,17,18,19,20,21], there was, nonetheless, a trend toward higher mortality in the MDR group.
Two independent risk factors associated with the emergence of MDR bacteria in IPN were identified—the number of antibiotic changes and the need for NS (enteral and/or parenteral nutrition)—whereas no independent risk factors were identified regarding the occurrence of FI at the first intervention.
In 2022, Lu et al. published a retrospective study analyzing 124 MDR and 143 non-MDR bacterial isolates from patients with IPN and identified the presence of extra-pancreatic infections, procalcitonin (PCT) level at admission, and the degree of pancreatic necrosis as independent risk factors for MDR bacteria isolation in IPN [14]. In contrast to our study, none of the patients were treated endoscopically, which does not represent current practice [4].
The results of this study highlight the importance of antibiotic selective pressure on the emergence of MDR pathogens [13,14] and preventing and treating malnutrition during ANP to avoid infection [22,23]. Regarding antibiotic pressure, Boxhoorn et al. showed in a recent randomized study that there was no advantage to immediate drainage in patients with suspected IPN compared to initial treatment with antibiotic therapy and postponed drainage, after which a third of patients improved with antibiotics alone [5]. However, targeted treatment could reduce the selective pressure of antibiotics on the emergence of resistant strains [14]. It is worth noting that patients with MDR and XDR infections required the greatest number of antibiotic changes, as treatments had to be continuously adapted according to microbiological culture results. This raises the question of causality—whether repeated antibiotic modifications contribute to the selection of resistance or, conversely, simply reflect the presence of already resistant infections. Moreover, the potential role of antibiotic-related toxicity, which may have prompted therapy changes in certain cases, should not be overlooked, as it could also have influenced the overall number of antibiotic switches [24]. These findings may support a more cautious and individualized approach to antibiotic therapy, potentially favoring early discontinuation when WONs are well drained and patients are hemodynamically stable, with only limited peri-interventional antibiotic use, and the acquisition of bacteriological documentation during interventions.
Regarding the nutritional aspect, several meta-analyses have shown that NS is a cornerstone of managing patients with AP [25,26]. Enteral nutrition (EN) is superior to parenteral nutrition (PN) in reducing mortality, persistent organ dysfunction, and systemic infection, as well as preserving mucosal integrity and intestinal motility [25,26], and therefore preventing bacterial translocation and secondary IPN [27]. In this study, NS was necessary in almost two-thirds of patients. The fact that the need for NS was identified as an independent risk factor for the emergence of MDR in IPN probably reflects a more severe and prolonged course of the disease related to malnutrition requiring NS and not a direct effect of NS.
Although the rate of FI doubled between the first intervention and the last one, our study did not identify any independent risk factors associated with FI at the first intervention. The decision to investigate risk factors of FI only at the first intervention, rather than across all interventions, was based on the fact that no previous studies have examined risk factors of FI at the time of the initial drainage, which can be more of a surrogate marker for overall disease severity. Indeed, the absence of a mortality difference between patients with and without FI at the first intervention indicates that FI may represent a marker of disease progression rather than a direct determinant of outcome. These findings are consistent with recent data from the United States supporting the idea that FI in AP may emerge as secondary events rather than primary complications [15]. Unlike some previous studies, prior antibiotic exposure did not appear to play a decisive role [28]. The variability in antifungal therapy observed across studies underlines the current lack of consensus regarding treatment indications in this setting [4,15]. Taken together, our results emphasize the need for clearer diagnostic criteria and evidence-based therapeutic guidelines for managing FI in IPN.
From an epidemiological perspective, this study showed that aerobic bacteria are predominant compared to anaerobic bacteria, as previously reported [4,29], with GNB and GPC the most represented [30,31,32]. From an antibiotic standpoint, the main classes administered before and after the initial intervention were predominantly penicillin + ß-lactamase inhibitors, antipseudomonal penicillin + ß-lactamase inhibitors, and carbapenem. Although robust evidence to guide empirical antibiotic selection is lacking [9,10,11], agents with good penetration into pancreatic necrosis are generally recommended. These include broad-spectrum penicillins, third- and fourth-generation cephalosporins, carbapenems, or fluoroquinolones with anaerobic coverage such as metronidazole [29,33,34,35,36]. Although the duration of antibiotics may appear prolonged in this study (43 days), current evidence does not clearly define the optimal length of antibiotic treatment in patients with IPN undergoing multiple drainage or necrosectomy procedures [13]. Ongoing antimicrobial stewardship initiatives aim to rationalize antibiotic use, and it is likely that future recommendations will emphasize shorter, more targeted therapy for IPN.
Our study has some limitations: First, it is retrospective and monocentric and has a limited number of patients. Second, this study was carried out in a tertiary center that is referenced for the treatment of complex cases; therefore, it does not fully represent all hospital settings. Moreover, we did not study the role of PCT, as we do not routinely measure it in daily practice; nevertheless, it could be a useful parameter to diagnose IPN by helping to differentiate patients who need antibiotics from those who present with an AP-related inflammatory reaction, especially during the first period of the disease [37]. Finally, the absence of independent risk factors for FI may be explained by the limited number of cases and the low proportion of immunocompromised patients in our cohort, which reduced the statistical power of the analysis.
Further studies should focus on improving the diagnosis of IPN, specifically using DWI-MRI and PCT to optimize when to initiate antibiotic therapy. This approach may help to better identify patients who need minimally invasive interventions with subsequent use of pathogen-directed antibiotics and thereby prevent the emergence of increasingly resistant bacteria. Another issue is determining the type and duration of antibiotic and antifungal therapy and how and when to prescribe them while limiting their duration.
4. Materials and Methods
4.1. Study Population
This was a retrospective study that included data on seventy-one patients with moderate-to-severe acute pancreatitis according to the Atlanta Classification 2012 [38], admitted between November 2009 and August 2021 to HUB-Erasme Hospital in Brussels. All consecutive patients who underwent a minimally invasive intervention for WON following ANP (for suspicion of infection, pain or extrinsic compression of surrounded organs) with a documented bacteriological culture from the WON and both contrast-enhanced computed tomography scan (CE-CT scan) and magnetic resonance imaging (MRI), including diffusion-weighted (DW) acquisition within a maximum of seven days before the first intervention, were included. Exclusion criteria were as follows: the presence of chronic pancreatitis, no CE-CT, MRI without specific DW-MRI sequences before the first intervention, or no bacteriological culture performed during the first intervention. MRI with DWI was considered a prerequisite for inclusion due to the concomitant goal to assess the diagnostic yield of DWI to confirm the presence of IPN [39], which will be reported in a separate study. Collected data for each patient are presented in Supplementary Table S1. The last follow-up was defined as either the date of the last documented clinical encounter (e.g., outpatient consultation) or the date of death.
4.2. Definitions
The patient was classified as having confirmed IPN if they had a positive culture of fluid/necrosis collected during the first drainage intervention for the WON or, in the case of positive blood cultures, without any other documented extra-pancreatic infection [40].
The patient was classified as having suspected IPN in the following situations: sustained septic shock, sepsis, or SIRS (at least 2 criteria); persistent (>3–5 days) or new onset of fever and elevated CRP levels and WBC without any other documented extra-pancreatic infection; imaging suggestive of infection by CE-CT (gas configurations within the WON) [41] or MRI with DWI (presence of thick wall and restriction of diffusion) [39]; or clinical and imaging features consistent with IPN despite negative cultures.
Non-IPN was defined by the absence of any pathogenic microorganism in the culture obtained during the initial intervention, along with no clinical or radiological evidence of infection. A sterile collection was defined by the absence of any microorganism in the culture obtained during the initial intervention.
FI was defined by the presence of fungi in the WON culture obtained during the first or subsequent interventions.
4.3. Microbiological Cultures and Antibiotics
Microbiological data collected for each patient, as well as definitions regarding in vitro antimicrobial susceptibility testing, are presented in Supplementary Table S2 [42].
4.4. Primary Endpoint
The primary endpoint was to identify risk factors associated with the emergence of MDR bacteria (aerobes/anaerobes) and FI (at the first drainage) in IPN.
4.5. Secondary Endpoints
Secondary endpoints included defining risk factors of overall IPN (including non-MDR, MDR, XDR, and PDR bacteria), characterizing local epidemiology of bacterial isolates from WONs, reporting the antibiotic and antifungal therapy administered, assessing adequacy of the first antibiotic choice based on the first bacteriological culture (defined as the in vitro susceptibility of the microorganism(s) isolated from the first positive culture to the initial empiric antibiotic regimen administered), and comparing survival and cumulative ICU admission rates between patients with IPN/non-IPN, MDR/non-MDR bacteria, and FI/non-FI.
4.6. Statistical Analysis
Continuous variables are described as means ± standard deviation (SD) or medians and interquartile range (IQR) in cases of non-normally distributed variables. Categorical variables are reported as counts and percentages. A logistic dichotomous dependent variable was used to identify factors associated with the emergence of MDR bacteria, FI at the first drainage, and IPN. A multivariable model was subsequently built using a stepwise procedure by introducing to the multivariate analyses only factors that reached significance in the univariate analysis.
The Kaplan–Meier approach was used to assess the survival rate incidence at 180 days and the cumulative rate of ICU admission at 90 days following AP diagnosis.
Data for patients were censored at 180 days for mortality or at 90 days for ICU admission.
A p-value < 0.05 was required for significance for the multivariable model.
Statistical analyses were performed using SPSS for macOS (version 28) and R for macOS (version 2023.06.1 + 524). Data processing and visualization, including the generation of Sankey diagrams, were performed using Python (version 3.11) with the pandas and matplotlib libraries.
5. Conclusions
The emergence of MDR bacteria in patients with IPN who required invasive procedures was observed in an alarming proportion of this cohort (51% of patients with MDR or XDR bacteria). The emergence of MDR bacteria was related to the number of antibiotic changes and the need for NS. In contrast, no independent factors for FI at first drainage were identified. Although this study did not demonstrate a significant difference in mortality between MDR and non-MDR IPN, the cumulative ICU admission rate was significantly higher in the MDR group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iannuzzi J.P. King J.A. Leong J.H. Quan J. Windsor J.W. Tanyingoh D. Coward S. Forbes N. Heitman S.J. Shaheen A.A. Global Incidence of Acute Pancreatitis Is Increasing Over Time: A Systematic Review and Meta-Analysis Gastroenterology 202216212213410.1053/j.gastro.2021.09.04334571026 · doi ↗ · pubmed ↗
- 2Petrov M.S. Yadav D. Global epidemiology and holistic prevention of pancreatitis Nat. Rev. Gastroenterol. Hepatol.20191617518410.1038/s 41575-018-0087-530482911 PMC 6597260 · doi ↗ · pubmed ↗
- 3Sahu S.K. Giri S. Das S. Patro C.D. Praharaj D.L. Mallick B. Nath P. Panigrahi S.C. Anand A.C. Approach to the Diagnosis and Management of Infected Pancreatic Necrosis: A Narrative Review Cureus 202517 e 8302010.7759/cureus.8302040421342 PMC 12104691 · doi ↗ · pubmed ↗
- 4Shah J. Fernandez Y.V.M. Jagodzinski R. Arvanitakis M. Infected pancreatic necrosis-Current trends in management Indian J. Gastroenterol.20244357859110.1007/s 12664-023-01506-w 38625518 · doi ↗ · pubmed ↗
- 5Boxhoorn L. van Dijk S.M. van Grinsven J. Verdonk R.C. Boermeester M.A. Bollen T.L. Bouwense S.A.W. Bruno M.J. Cappendijk V.C. Dejong C.H.C. Immediate versus Postponed Intervention for Infected Necrotizing Pancreatitis N. Engl. J. Med.20213851372138110.1056/NEJ Moa 210082634614330 · doi ↗ · pubmed ↗
- 6Hu W.M. Hua T.R. Zhang Y.L. Chen G.R. Song K. Pendharkar S. Wu D. Windsor J.A. Prognostic significance of organ failure and infected pancreatic necrosis in acute pancreatitis: An updated systematic review and meta-analysis J. Dig. Dis.20232464865910.1111/1751-2980.1324338037512 · doi ↗ · pubmed ↗
- 7Podda M. Pellino G. Di Saverio S. Coccolini F. Pacella D. Cioffi S.P.B. Virdis F. Balla A. Ielpo B. Pata F. Infected pancreatic necrosis: Outcomes and clinical predictors of mortality. A post hoc analysis of the MANCTRA-1 international study Updates Surg.20237549352210.1007/s 13304-023-01488-636899292 PMC 10005914 · doi ↗ · pubmed ↗
- 8Li X.Y. He C. Zhu Y. Lu N.H. Role of gut microbiota on intestinal barrier function in acute pancreatitis World J. Gastroenterol.2020262187219310.3748/wjg.v 26.i 18.218732476785 PMC 7235204 · doi ↗ · pubmed ↗