CXCR4: A Promising Novel Strategy for Lung Cancer Treatment
Mengting Liao, Jianmin Wu, Tengkun Dai, Guiyan Liu, Jiayi Zhang, Yiling Zhu, Lin Xu, Juanjuan Zhao

TL;DR
CXCR4 is a key player in lung cancer progression and a potential target for new treatments.
Contribution
This paper reviews CXCR4's role in lung cancer and evaluates therapeutic strategies targeting it.
Findings
CXCR4 promotes tumor growth, metastasis, and resistance to therapy in lung cancer.
Targeting CXCR4 with drugs or imaging agents shows promise in preclinical and early clinical studies.
CXCR4 expression is linked to poor prognosis and could serve as a biomarker for treatment response.
Abstract
Lung cancer remains a major public health challenge due to high incidence and mortality. The chemokine receptor CXCR4 and its ligand CXCL12 (SDF-1) constitute a critical axis in tumor biology, influencing tumor cell proliferation, invasion, angiogenesis, and immune evasion. Aberrant CXCR4 expression is frequently observed in lung cancer and is closely associated with adverse prognosis, enhanced metastatic potential, and therapeutic resistance. Mechanistically, CXCR4 activates signaling pathways including PI3K/AKT, MAPK/ERK, JAK/STAT, and FAK/Src, promoting epithelial–mesenchymal transition, stemness, and survival. The CXCL12/CXCR4 axis also orchestrates interactions with the tumor microenvironment, facilitating chemotaxis toward CXCL12-rich niches (e.g., bone marrow and brain) and modulating anti-tumor immunity via regulatory cells. Regulation of CXCR4 occurs at transcriptional,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
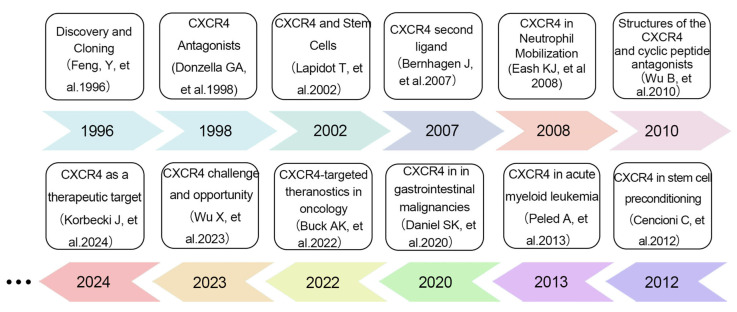 Figure 1
Figure 1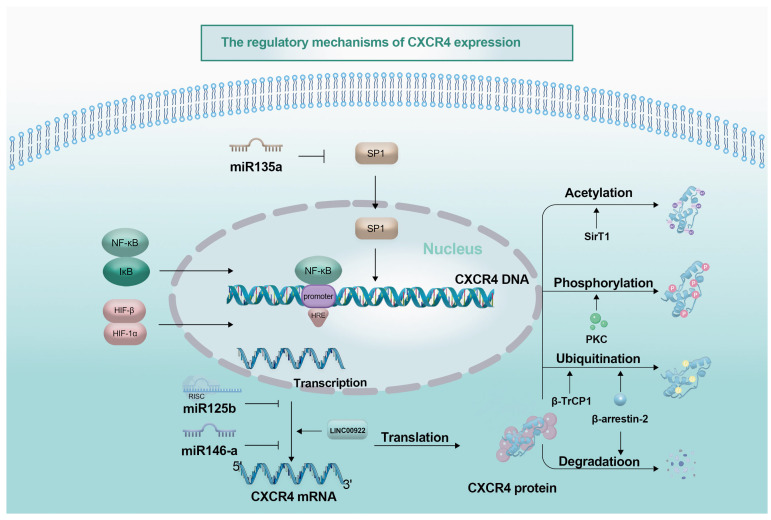 Figure 2
Figure 2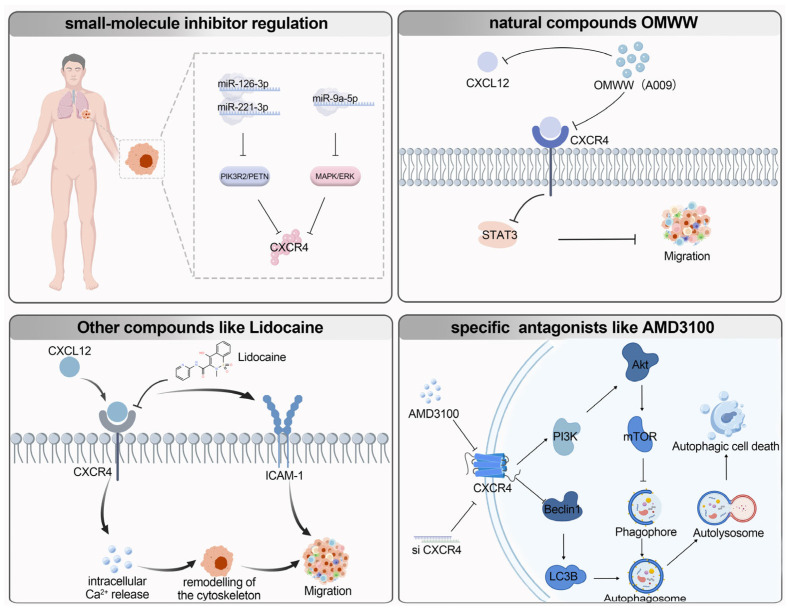 Figure 3
Figure 3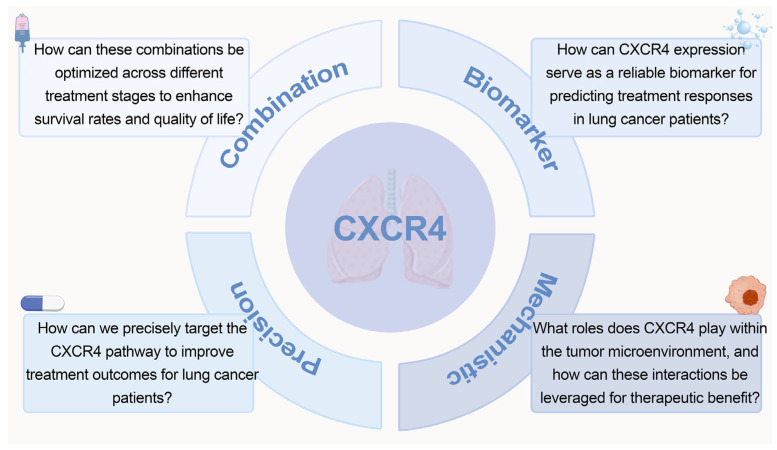 Figure 4
Figure 4- —National Natural Science Foundation of China
- —Innovation Center of Chinese Ministry of Education
- —Laboratory for Cancer Prevention and treatment of Guizhou Province
- —Project of Guizhou Provincial Department of Science and Technology
- —Medical Research Union Fund for High-quality health development of Guizhou Province
- —Program for Excellent Young Talents of Zunyi Medical University
- —“12345 Future Talent Training Plan” of Zunyi Medical University—Future science and technology Elite talent project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemokine receptors and signaling · Cytokine Signaling Pathways and Interactions · Lung Cancer Research Studies
1. Introduction
Lung cancer remains a major global health burden, with incidence and mortality rising worldwide since 2011. According to the 2022 Global Cancer statistics, it was the most prevalent cancer, accounting for approximately 2.5 million new cases (about 12.4% of all cancers) and the leading cause of cancer-related death, responsible for about 1.8 million deaths (18.7%) [1]. Lung cancer is primarily categorized into two major types: non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). NSCLC accounts for approximately 80% to 85% of cases, including histological subtypes such as adenocarcinoma and squamous cell carcinoma, while SCLC constitutes the remaining portion [2]. As the most common type of lung cancer, NSCLC exhibits high incidence and mortality rates. Current treatment options primarily include surgical resection, chemotherapy, targeted therapy, and radiation therapy. Despite recent advancements in lung cancer research, the overall prognosis for patients remains grim due to the complex and poorly understood mechanisms of the disease, leading to low five-year survival rates. Consequently, there is an urgent need to explore more effective treatment strategies and identify new clinical treatment approaches.
Recent advancements in biotechnology and interdisciplinary research have led to breakthrough opportunities in the field of lung cancer treatment [3,4,5]. Notably, the advent of gene therapy offers significant potential for the identification and development of novel therapeutic targets [6]. In this context, the C-X-C chemokine receptor 4 (CXCR4) and its ligand CXCL12 have garnered widespread attention. Research indicates that CXCR4 plays a central role in tumor occurrence, development, and metastasis. It regulates cancer cell proliferation, survival, angiogenesis, and invasive capacity, while also influencing the formation and maintenance of the tumor microenvironment. Moreover, CXCR4 participates in the dynamic balance of the immune system by regulating the migration and hematopoietic function of immune cells. Therefore, abnormal overexpression of CXCR4 is closely associated with the occurrence, development, and prognosis of various tumors, including lung cancer, leukemia, breast cancer, prostate cancer, and multiple myeloma.
Given the critical role of CXCR4 in lung cancer progression, researchers have conducted in-depth explorations into its potential as a therapeutic target. Targeting CXCR4 through various intervention strategies is anticipated to provide new treatment options for lung cancer patients, thereby enhancing their survival rates and quality of life. This paper aims to systematically review the expression patterns and mechanisms of action of CXCR4 in lung cancer, as well as summarize the current status and future prospects of its use as a therapeutic target. By doing so, it seeks to offer new perspectives and directions for the precision diagnosis and treatment of lung cancer.
2. Overview of CXCR4
The CXCR4 gene, located on chromosome 2q22.1, is an important member of the G protein-coupled receptor (GPCR) family [7]. It features the characteristic seven transmembrane domain structure and is composed of 352 amino acid residues. This structure includes a highly conserved N-terminal extracellular domain, seven transmembrane α-helical regions (TM1–TM7), and an intracellular loop domain [8,9,10]. CXCR4 is widely expressed in human tissues, particularly showing significant expression patterns in organs such as bone marrow, thymus, stomach, and lungs, highlighting its key critical regulatory role in various physiological and pathological processes [10].
At the molecular level, the N-terminal extracellular domain of CXCR4 exhibits a high affinity for its ligand, stromal cell-derived factor 1 (SDF-1, also known as CXCL12). Notably, the third intracellular loop of CXCR4 demonstrates a unique structure-function duality: it not only directly engages in ligand recognition and binding through specific amino acid residues but also facilitates G protein-coupled signal transduction via conformational changes. This process precisely regulates the intensity and duration of downstream signaling. During signal transduction, CXCR4 relies on the conserved DRY motif (Asp-Arg-Tyr triplet) in the transmembrane region and requires the coordinated formation of specific spatial conformations among the seven transmembrane domains. Recent studies revealthat the tetrameric conformation of CXCR4, multi-ligand competitive binding, and oligomerization regulation provide new avenues for investigating the co-receptor functional domain and ligand-binding domain, thereby advancing the development of precision-targeted therapeutics in tumor metastasis and related fields [11,12,13].
CXCR4 fulfills numerous roles, such as mediating cellular signal transduction by coupling with inhibitory G proteins to affect cell migration, adhesion, and gene transcription [14]. In hematopoietic stem cell homing, CXCR4 interacts with CXCL12 to regulate the migration of CD34^+^ hematopoietic stem cells within the bone marrow [15]. Additionally, CXCR4 binds with high affinity to CXCL12, facilitating the migration of various cell types [16]. It also plays a crucial role in coordinating innate and adaptive immune responses by regulating leukocyte transport and distribution in peripheral tissues, promoting lymph node tissue formation, stabilizing immune synapses, and maintaining T cell activation [17]. In the context of tumor growth and metastasis, CXCR4 is instrumental in processes such as tumor growth, invasion, angiogenesis, metastasis, and treatment resistance. Moreover, the CXCL12/CXCR4 axis promotes angiogenesis, with signaling molecules stimulating CXCL12/CXCR4 expression [18].
CXCL12 (also known as SDF-1) is the sole ligand for CXCR4, and the CXCR4/CXCL12 axis participates in numerous biological processes by activating pathways such as PI3K-AKT, MAPK/ERK, JAK/STAT, and others to regulate migration, invasion, and metastasis [19]. The axis is prominently expressed across multiple tumor types and plays a significant role in shaping the tumor microenvironment (TME) by modulating immune cell trafficking and function, thereby supporting tumor progression. Specifically, the CXCR4/CXCL12 axis interacts with T cell and B cell receptors (TCR and BCR), in conjunction with CD47, to promote macrophage phagocytosis of tumor cells, an interaction referred to as immune gene surrender (IGS) [8]. Therefore, the CXCR4/CXCL12 axis holds significant promise in tumor immunotherapy. The diversity of the CXCR4/CXCL12 axis is reflected in the different subtypes of its ligand, CXCL12. Currently, seven CXCL12 subtypes have been identified (α, β, γ, δ, ε, θ, and the predicted iso7), with α and β being the most extensively studied forms, consisting of 89 and 93 amino acids, respectively [20,21]. The γ subtype is highly expressed in organs with low vascularization, such as the heart and brain. Although it has lower efficacy, it exhibits the highest binding affinity for CXCR4 and the longest duration of downstream effects [22,23].
In lung cancer, metastasis is the primary cause of poor prognosis and high recurrence rates, while epithelial–mesenchymal transition (EMT) is a key pathological factor in the early metastasis of primary lung cancer. Studies have shown that abnormalities in the CXCL12-CXCR4 signaling axis play a significant role in tumor cell EMT, invasion, and chemotherapy resistance [24]. Beyond tumor cell–intrinsic effects, the axis participates in shaping immune cell infiltration and organ-specific colonization, acting as a guiding, driving, and targeting signal for metastatic spread.
In summary, as a multifunctional GPCR, CXCR4 exhibits widespread distribution and diverse functions that are important in both normal physiology and disease (Figure 1). Landmark studies over the past three decades have continuously deepened our understanding of its pleiotropic roles. In 1996, Feng et al. published a seminal work in Science that first cloned CXCR4 and identified it as a key coreceptor mediating HIV-1 entry into T cells, laying the fundamental groundwork for subsequent functional explorations of this receptor [25]. Two years later, Donzella et al. reported in Nature Medicine that the small-molecule inhibitor AMD3100 blocks HIV-1 infection by targeting CXCR4, which was the first demonstration of the action mechanism of CXCR4 antagonists and provided critical candidate molecules for anti-HIV drug development [26]. A pivotal breakthrough in deciphering CXCR4 ligand interactions came in 2007, when Bernhagen J et al. identified macrophage migration inhibitory factor (MIF) as a second endogenous ligand for CXCR4, challenging the long-held dogma of exclusive CXCL12-CXCR4 binding and revealing the receptor’s ligand diversity [27]. The molecular underpinnings of CXCR4 function were further elucidated in 2010, when Wu B et al. resolved the first crystal structure of CXCR4 in complex with a small-molecule antagonist, offering an essential structural blueprint for targeted drug design [28]. In the realm of oncology, CXCR4 has steadily emerged as a promising therapeutic target, with accumulating evidence highlighting its involvement in tumor pathogenesis and progression across multiple malignancies. In 2013, Peled et al. demonstrated in Theranostics its critical role in the pathogenesis of acute myeloid leukemia (AML), clarifying its context-specific regulatory mechanisms in hematologic malignancies [29]. In 2019, Daniel et al. expanded this perspective in Seminars in Cancer Biology, revealing that the CXCL12-CXCR4/CXCR7 signaling axis mediates immune resistance in gastrointestinal malignancies and providing novel insights for combining targeted therapy with immunotherapy [30]. Progress in clinical translation was summarized in 2022 by Buck et al. in European Journal of Nuclear Medicine and Molecular Imaging, who systematically reviewed advances in CXCR4-targeted theranostic strategies and accelerated the translation of basic research into clinical practice [31]. Most recently, in 2024, Korbecki et al. further validated the feasibility of CXCR4 as a therapeutic target in AML in a study published in Leukemia, proposing optimized intervention strategies that offer updated support for precision oncology [32]. Against this backdrop of expanding insights into CXCR4-mediated oncogenic pathways across cancer types. In the context of lung cancer, the CXCR4/CXCL12 axis holds considerable potential for understanding tumor occurrence, progression, and metastasis, offering valuable insights for future therapeutic strategies. In the context of lung cancer, the CXCR4/CXCL12 axis holds considerable potential for understanding tumor occurrence, progression, and metastasis, offering valuable insights for future therapeutic strategies.
3. Molecular Regulation of CXCR4 Expression
CXCR4 is a chemokine receptor widely expressed across various cell types, particularly in immune cells, hematopoietic stem cells, and multiple tumor cell types. It is notably overexpressed in diverse tumors, including lung cancer [23]. Beyond facilitating tumor cell migration and invasion, CXCR4 also modulates tumor immune responses by impacting immune cell functions within the tumor microenvironment. Studies highlight that CXCR4 expression is particularly elevated in lung cancer cells, closely linked to its critical roles in tumor cell proliferation, metastasis, and the formation of the tumor microenvironment [37]. High CXCR4 expression is not only associated with tumor initiation and progression but also closely related to patient prognosis, making it clinically significant to thoroughly investigate its expression patterns and regulatory mechanisms. CXCR4 expression is regulated at multiple levels, including transcriptional regulation, post-transcriptional modifications, and post-translational modifications. Together, these multi-level regulatory mechanisms determine the functional changes in CXCR4 under various physiological and pathological conditions.
3.1. Regulation of CXCR4 Transcription Levels
Transcription factors directly control CXCR4 transcription levels by binding to its gene promoter region. For example, c-Myb has been shown to regulate CXCR4 expression, with at least 10 potential c-Myb binding sites identified in the CXCR4 promoter region and regulated by Myb protein [38]. Another study found that SP1 is a frequently binding transcription factor in the core promoter region of CXCR4, with evidence showing that miR-135a can inhibit CXCR4 expression by targeting SP1 [39]. Quintana AM’s team also noted SP1 binding sites in the CXCR4 promoter region and suggested that SP1 may promote CXCR4 transcription by binding to the CXCR4 promoter [40]. Additionally, NF-κB can bind to the CXCR4 promoter region, boosting its transcriptional activity and substantially increasing CXCR4 expression, with this regulatory effect being particularly pronounced in inflammatory and tumor cells [7]. NF-κB can also promote cancer cell migration and invasion through the CXCL12/CXCR4 axis [41]. Furthermore, under hypoxic conditions in vitro, HIF-1α can bind to the CXCR4 promoter region, significantly upregulating CXCR4 expression and thereby enhancing cellular migration capacity [42,43].
Notably, inflammatory signaling pathways form a positive feedback loop to regulate CXCR4 transcription. For instance, in in vitro glioblastoma cell models, TNF-α stimulation increases NF-κB binding to the CXCR4 promoter, leading to upregulation of CXCR4 expression—a mechanism also validated in in vitro NSCLC cell lines [44]. Moreover, downstream signaling pathways activated by CXCR4 can feedback-regulate its transcription: sustained activation of the PI3K-AKT pathway promotes CXCR4 gene transcription by phosphorylating transcription factors such as NF-κB [45].
DNA methylation also significantly influences CXCR4 expression as a key epigenetic modification. For example, in peripheral blood mononuclear cells from patients with chronic hepatitis B-related liver fibrosis/cirrhosis, hypomethylation of the CXCR4 promoter region was significantly associated with increased CXCR4 expression levels [46]; whereas in pancreatic cancer, hypermethylation of the CXCR4 promoter was associated with low expression. In normal pancreatic tissue, the 5′ CpG island of the CXCR4 gene is unmethylated, whereas hypermethylation of the promoter region was detected in 45% of pancreatic cancer cell lines and 46% of primary pancreatic adenocarcinomas, with a significant negative correlation between methylation and CXCR4 mRNA expression levels [47]; Additionally, in hepatocellular carcinoma, downregulation of UHRF1 activates the CXCR4/AKT-JNK/IL-6/Snail signaling axis, thereby increasing tumor malignancy [48]. Other studies have also indicated a negative correlation between DNA methylation and CXCR4 expression, with high methylation of the CXCR4 gene promoter region inhibiting its transcription. Analyzing the DNA methylation status of the CXCR4 promoter region in gastric cancer cells found that high methylation was significantly associated with CXCR4 expression downregulation [49]. These factors influencing CXCR4 expression provide important references for the diagnosis and treatment of lung cancer.
In addition to transcription factors and epigenetic modifications, the tumor microenvironment regulates CXCR4 transcription via paracrine mechanisms. Immune-suppressive cells such as tumor-associated macrophages (TAMs) and regulatory T cells (Tregs) secrete cytokines like CXCL12 and IL-6, inducing tumor cells to upregulate CXCR4 expression. Meanwhile, growth factors secreted by tumor-associated fibroblasts (CAFs), such as EGF and bFGF, enhance CXCR4 transcriptional activity through downstream signaling pathways [50]. This microenvironment-mediated regulation tightly links CXCR4 expression to the tumor’s immunosuppressive state and stromal remodeling processes.
Ligand-receptor interaction and co-receptor crosstalk also contribute to transcriptional regulation of CXCR4. As the high-affinity ligand of CXCR4, CXCL12 binds specifically to CXCR4 to trigger conformational changes in the receptor’s intracellular domain, initiating G protein coupling and signal cascades. Sustained CXCL12 stimulation further upregulates CXCR4 expression on tumor cell surfaces, forming a positive feedback loop that amplifies its oncogenic functions [30,51]. CXCR7, another functional receptor for CXCL12, modulates CXCR4 activity through dual mechanisms: forming heterodimers with CXCR4 to synergistically enhance downstream PI3K-AKT and MAPK/ERK signaling, or competitively binding CXCL12 to regulate local ligand concentrations and indirectly affect CXCR4-mediated chemotaxis [30,52].
3.2. Post-Transcriptional Regulation
Post-transcriptional regulation of CXCR4 plays a critical role in various cellular functions and disease processes. Recent studies have revealed that non-coding RNAs (including miRNAs and lncRNAs) significantly affect the post-transcriptional regulation of CXCR4, influencing its expression levels and functional activity through complex regulatory networks.
3.2.1. miRNA Regulation of CXCR4
Direct targeting regulation: Studies have shown that miR-125b [53], miR-146a [51], miR-155 [54], and miR-21 [55] can inhibit CXCR4 translation by directly binding to its mRNA 3′UTR region. For instance, miR-146a is induced by the LMP1 protein in EB virus-infected cells. LMP1, an EB virus-encoded protein, activates multiple intracellular signaling pathways, including the NF-κB signaling pathway, thereby inducing the expression of miR-146a. miR-146a then binds to the 3′UTR region of CXCR4 mRNA, inhibiting CXCR4 translation, forming an LMP1-miR-146a-CXCR4 regulatory axis, ultimately affecting cellular proliferation and metastasis capacity [53,56]. In breast cancer cells, miR-146 can directly target CXCR4, inhibiting its expression, suppressing NF-κB activity, and reducing the cells’ metastatic potential. In colorectal cancer, miR-125b, induced by the CXCL12/CXCR4 axis, can bind to CXCR4 mRNA 3′UTR, enhancing autophagy, thereby promoting the invasion of colorectal cancer cells while conferring resistance to 5-fluorouracil. Furthermore, miR-9a-5p can directly target and downregulate CXCR4 expression, thus inhibiting MAPK pathway activation and alleviating lung injury in rats [57,58].
Notably, miRNA-mediated regulation of CXCR4 exhibits tumor-specific and functional diversity. In colorectal cancer, miR-126 expression is significantly reduced, and it directly targets the 3′UTR of CXCR4 to suppress its expression, thereby blocking the RhoA signaling pathway and reducing tumor cell migration, invasion, and epithelial–mesenchymal transition (EMT) processes; patients with low miR-126 expression have poorer prognosis [59,60,61]. In hepatocellular carcinoma, activation of the CXCL12/CXCR4 axis induces miR-125b expression, which in turn enhances CXCR4 activity, forming a positive feedback loop that promotes tumor stemness and resistance to 5-fluorouracil (5-FU) chemotherapy [51]. Additionally, miR-372 expression is downregulated in hepatocellular carcinoma tissues, and it directly targets CXCR4 mRNA to inhibit cell proliferation, EMT, and anti-apoptotic capacity [62]. miR-9a-5p also directly targets the CXCR4 3′UTR, reducing MAPK/ERK pathway activity by 42% [44]. Moreover, miR-126-3p/miR-221-3p inhibits PIK3R2/PTEN, thereby blocking the CXCR4/AKT signaling axis with an inhibition efficiency of 68% [44].
Indirect pathway regulation: Recent studies highlight that in macrophages, the absence of miR-301a can diminish cell migration and phagocytic capacity through the YY1/CXCR4 pathway [63]. In colorectal cancer, miR-1269a targets PCDHGA9, activating CXCR4 and β-catenin signaling pathways, promoting tumor cell invasion and metastasis [64]. miR-1910-5p influences angiogenesis by regulating CXCR4 function through MMRN2, thereby affecting vascular permeability [65]. miR-1910-5p regulates vascular permeability via the MMRN2/CXCR4 pathway; additionally, studies have shown that miR-9a-5p alleviates lung injury through the CXCR4/MAPK pathway.
3.2.2. Long Non-Coding RNAs Participate in CXCR4 Regulation Through the Formation of Complex ceRNA Networks
Liang et al. found that CXCR4 is upregulated in lung cancer cells, with LINC00922 promoting lung cancer progression through the miR-204/CXCR4 signaling axis. Experimental evidence shows that overexpression of LINC00922 significantly upregulates CXCR4 expression levels and enhances the migration and invasion capabilities of lung cancer cells. Clinical correlation analysis indicates that this mechanism is associated with poor patient outcomes [66].
An interesting finding is that lncRNA NORAD exhibits cell-type-specific regulation of CXCR4. In the NSCLC cell line A549 cells, lncRNA NORAD can downregulate CXCR4 levels, significantly inhibiting cell proliferation, migration, and invasion [67]. However, this regulatory mechanism is controversial, as other studies report minimal basal CXCR4 expression in A549 cells, yet NORAD overexpression enhances tumor spheroid formation, proliferation, and EMT progression, suggesting CXCR4 fosters a more invasive tumor phenotype [68]. These seemingly contradictory findings may reflect the complexity of the CXCR4 regulatory network, suggesting that its function may be highly dependent on the cellular microenvironment or specific pathological states. Further investigation into the dynamic regulatory mechanisms of CXCR4 in different cell types and disease progression could not only clarify its dual role in tumorigenesis but also provide new theoretical basis and therapeutic strategies for targeted interventions.
Additional lncRNAs and circular RNAs (circRNAs) have been identified as key regulators of CXCR4 through ceRNA networks. In hepatocellular carcinoma, high expression of lncRNA HULC specifically binds to miR-372, releasing its targeted suppression of CXCR4 and thereby promoting cell proliferation, EMT, and anti-apoptotic processes [62]. In breast cancer, loss of lncRNA MEG3 is common; MEG3 directly binds to the chromatin regulator CTCF, preventing CTCF from binding to the CXCR4 promoter and inhibiting its transcription. Overexpression of MEG3 significantly reduces breast cancer cell migration [69]. Moreover, hormonal regulation via the ERβ/circ-TMX4/miR-622 pathway upregulates CXCR4 expression through epigenetic modifications: circ-TMX4 acts as a sponge for miR-622, alleviating its inhibitory effect on CXCR4 mRNA and enhancing lung cancer cell invasion capacity by 2.3-fold [70,71,72]. Additionally, CXCR4-modified mesenchymal stem cell-derived exosomes can carry miR-320, which suppresses VEGF/IGF-1 signaling to regulate pathological angiogenesis in diabetes-associated tumors, indirectly influencing CXCR4-mediated angiogenic functions [50,73].
These findings reveal the high complexity of post-transcriptional regulation of CXCR4: (1) regulatory mechanisms exhibit cell type and disease specificity; (2) they form multi-layered regulatory networks, including miRNA-lncRNA interactions; (3) they engage in cross-talk with multiple signaling pathways, such as MAPK and Wnt/β-catenin. Elucidating these regulatory mechanisms provides new targets for precision therapy in related diseases, particularly those involving CXCR4 overactivation, such as tumors and inflammatory conditions. Future research should further investigate the synergistic interactions among different regulatory elements and their dynamic changes under various pathological conditions.
3.3. Post-Translational Modification
Post-translational modification of CXCR4 mainly includes multiple processes such as phosphorylation, glycosylation, and ubiquitination. Regarding phosphorylation, studies have shown that the lack of phosphorylation hinders ligand-induced receptor endocytosis and cytoskeletal rearrangement, but does not significantly affect cell adhesion and chemotaxis [74]. CXCR4 can be phosphorylated by multiple kinases, affecting its coupling with G proteins and the activation of downstream signaling pathways [75]. Structural studies have also indicated that phosphorylation of serine/threonine residues in the intracellular loop and carboxy-terminal region of CXCR4 can regulate the recruitment of β-arrestin and signal transduction [76]. Additionally, protein kinase C (PKC) phosphorylates the Ser-324/5 site of CXCR4, matching PKC’s phosphorylation recognition sequence, activated post-CXCL12 stimulation, regulating CXCR4 endocytosis and degradation. G protein-coupled receptor kinase 6 (GRK6) plays a crucial role in CXCR4 phosphorylation at multiple sites. Under CXCL12 stimulation, GRK6 rapidly phosphorylates the Ser-324/5 site on CXCR4, delays Ser-330 phosphorylation, and rapidly phosphorylates the Ser-339 site, regulating CXCR4 signaling [77]. Meanwhile, GRK2 and GRK3 also participate in the phosphorylation process of CXCR4, phosphorylating the Ser-346/347 sites of CXCR4 and affecting the coupling of CXCR4 with G proteins, thereby regulating signal transduction such as calcium ion release [77]. These studies underscore the complexity and dynamic nature of CXCR4 phosphorylation, involving multiple kinases’ cooperation to finely regulate its signal transduction and cellular functions by phosphorylating different CXCR4 sites [74].
Ubiquitination modification significantly impacts CXCR4 function. Studies indicate that CXCR4 undergoes K63- and K48-specific ubiquitination. Inhibition of its ubiquitination reduces protein stability, cell surface expression, and signal transduction capacity, thereby restricting cell migration [78]. The E3 ubiquitin ligase β-TrCP1 regulates CXCR4 stability, modulating CXCR4-dependent signaling and HIV-1 entry. Interaction between β-TrCP1 and CXCR4 leads to decreased CXCR4 protein levels [79]. Freedman NJ et al. [80] found that β-arrestin-2 regulates CXCR4 ubiquitination and degradation, impacting its cell surface expression.
Glycosylation modifications also hold significance. Absence of glycosylation in CXCR4 reduces receptor stability, lowers its surface expression, and affects ligand binding and signal transduction [81]. Further research indicates that N-glycosylation (a ubiquitous post-translational modification process of proteins) is crucial for maintaining CXCR4’s normal folding, stability, and surface expression, with glycosylation site mutations impairing its function [82].
CXCR4 also undergos acetylation, influencing its G protein binding and downstream signaling pathway activation, thereby affecting cellular chemotaxis and migration [83]. Research suggests Sirt1-dependent CXCR4 acetylation impacts CXCR4 co-receptor activity [84]. Additionally, CXCR4 nitrosylation alters its conformation, affecting ligand binding and signal transduction, thereby regulating cellular immune responses and HIV-1 invasion [85].
Notably, downstream signaling pathways of CXCR4 also regulate its function through post-translational modifications. The MAPK/ERK pathway enhances CXCR4 protein stability by regulating post-translational modifications, reducing its degradation [45]. Furthermore, during CXCR4-mediated EMT, activation of transcription factors such as Snail and Twist can conversely upregulate CXCR4 expression, forming a “signaling pathway—transcription factor—CXCR4” feedback loop that sustains the malignant phenotype of tumor cells [50].
CXCR4 expression is regulated at multiple levels, including transcriptional, post-transcriptional, and post-translational modifications (Figure 2). These regulatory mechanisms collectively influence the onset, progression, and outcome of tumors. In-depth investigation of the expression patterns and regulatory mechanisms of CXCR4 not only helps elucidate its role in tumors such as lung cancer but also offers potential opportunities for developing new targeted therapeutic strategies. Targeting CXCR4 and associated regulatory factors (such as miRNAs and lncRNAs) enables the design of precise treatments to inhibit tumor cell migration, invasion, and metastasis, improving patient outcomes.
4. The Dual Role of CXCR4 in Lung Cancer Progression and the Tumor Microenvironment
4.1. Significant Heterogeneity in the Relationship Between CXCR4 Expression and Clinical Prognosis
As an important member of the chemokine receptor family, CXCR4 plays multiple biological roles in the development and progression of malignant tumors. Studies have shown that CXCR4 exhibits significantly high expression in both primary and metastatic lesions of NSCLC [86]. This expression pattern is closely associated with various clinical and pathological characteristics of lung cancer. Notably, CXCR4 expression varies significantly between histological subtypes. Meta-analysis data reveal that the positive expression rate of CXCR4 in lung adenocarcinoma is 51.8% (337/650), compared to 50.3% (224/445) in lung squamous cell carcinoma, with a statistically significant difference between the two. Interestingly, other studies have found an even stronger association of CXCR4 expression with lung squamous cell carcinoma.
As an important biomarker for NSCLC, CXCR4 expression levels and their relationship with clinical prognosis have become major research foci. Extensive clinical evidence indicates that the overexpression of CXCR4 in NSCLC tissue is significantly positively correlated with early tumor metastasis and poor clinical outcomes. However, there remains some heterogeneity in the assessment of the prognostic value of CXCR4 across different studies. Based on existing research data, multiple meta-analysis results indicate that high CXCR4 expression is an independent risk factor for poor prognosis in NSCLC patients. Notably, histological subtype analyses have identified significant gene mutation differences between patients with high and low CXCR4 expression in lung squamous cell carcinoma and lung adenocarcinoma [24]. Additionally, CXCR4 expression levels exhibit distinct specificity concerning histological subtypes. Zhu et al. found that in the specific pathological subtype of adenocarcinoma–squamous cell carcinoma (ASC), high CXCR4 expression is significantly associated with aggressive clinical features such as lymph node metastasis (pN^+^) and advanced TNM staging (stages III-IV). Moreover, patients with high CXCR4 expression have significantly lower 5-year disease-free survival (DFS) and overall survival (OS) rates, findings that remain statistically significant in multivariate Cox regression analysis [24,57,87].
Otsuka’s pioneering research in 2011 found that CXCR4 was overexpressed in 78% of NSCLC tissues and significantly associated with shorter overall survival in stage IV patients (HR = 1.89, p < 0.01), with the effect being more pronounced in male patients [88]. However, Fung’s recent research presents a different perspective: Although CXCR4 expression levels increase with disease progression (Stage I: 1729 ± 1083 vs. Stage IV: 2640 ± 1541), it is relatively low in early-stage patients, with no significant association between CXCR4 expression and recurrence-free survival (p = 0.60) or overall survival (p = 0.30), and no observed gender differences. Notably, a co-expression pattern of CXCR4 in both the nucleus and cell membrane was observed in advanced-stage patients [89], aligning with findings from Qiu’s team [90]. These findings further confirm that the CXCR4 signaling pathway is a key molecular mechanism mediating tumor cell–matrix interactions and promoting tumor growth and metastasis.
4.2. Multiple Mechanisms by Which CXCR4 Promotes Tumor Progression
CXCR4 is critically involved in numerous pathways that facilitate tumor progression, acting through a diverse array of mechanisms.
4.2.1. Epithelial–Mesenchymal Transition (EMT) and Tumor Progression
One of the key processes promoted by CXCR4 is epithelial–mesenchymal transition (EMT), a pivotal event in cancer metastasis. CXCR4 orchestrates EMT through dual mechanisms: classical signaling pathways and autocrine loops. In the classical pathway, the activation of the CXCL12/CXCR4/β-catenin/PPARδ axis leads to an increase in β-catenin nuclear translocation, significantly inducing changes in EMT marker expression (upregulation of N-cadherin and downregulation of E-cadherin) [91]. These changes facilitate the cellular transitions necessary for enhanced metastatic potential.
In addition to these pathways, a novel autocrine signaling loop has been identified in CXCR4-overexpressing lung cancer A549 cells. Here, the Macrophage Migration Inhibitory Factor (MIF), a less typical ligand for CXCR4 compared to CXCL12, is secreted at levels 4.5 times higher, establishing an MIF-CXCR4 positive feedback loop. This loop dramatically enhances the tumor’s spheroid formation capacity [92]. Intriguingly, experimental interventions that disrupt this feedback mechanism can reverse EMT and curtail cell migration [93], underscoring this loop’s therapeutic potential.
4.2.2. CXCR4 and the Immunosuppressive Tumor Microenvironment
Beyond promoting EMT, CXCR4 plays a key role in shaping the immunosuppressive microenvironment. In lung adenocarcinoma, CXCR4 expression is correlated with a complex immune landscape: it exhibits a moderate negative correlation with tumor purity and a moderate positive correlation with the infiltration of various immune cells, including B cells, CD4^+^ and CD8^+^ T cells, macrophages, and dendritic cells. This distinct expression pattern implies that CXCR4 is integral to the crosstalk between tumors and the immune system, impacting tumor-immune interactions significantly. Furthermore, CXCR4’s expression level is of substantial clinical prognostic value.
In NSCLC patients, high CXCR4 expression on tumor cells is strongly associated with poor prognosis and high response rates to immunotherapy [57,58,94,95,96,97]. Studies have shown that in mouse transplanted tumor models in vivo CXCR4^+^ cells promote myeloid-derived suppressor cell (MDSC) recruitment, suppress cytotoxic T cell function, and activate Treg cells. This orchestrated action contributes to the establishment of an immunosuppressive milieu [98,99].
The results demonstrate that within the CXCR4-high expressing subpopulation of MICs, cells concurrently exhibit high PD-L1 expression, suggesting a significant positive correlation between high CXCR4 expression status and high PD-L1 expression. Notably, despite the concomitant high PD-L1 expression (generally considered to mediate immune evasion), this subpopulation exhibits markedly enhanced sensitivity to immunotherapy, resulting in a 3.2-fold increase in immunotherapy response rate [57]. This observation has spurred the development of targeted therapeutic strategies. For instance, CXCL12 inhibitors have been shown to enhance T cell infiltration in mouse transplanted tumor models in vivo. Moreover, when these inhibitors are combined with PD-1 blockers, there is a notable extension in survival in mouse models, showcasing promising translational potential [100,101].
4.3. Small Cell Lung Cancer
CXCR4 can mediate the migration and adhesion of SCLC cells to mesenchymal cells. Some studies have found that it is precisely due to the migration of cancer cells to mesenchymal cells mediated by CXCR4 and integrin that cancer cells escape necrosis caused by chemotherapy [102]. The team found through Kaplan–Meier survival analysis that the level of CXCR4 expression significantly affects patients’ DFS (p = 0.005). with patients in the high CXCR4 expression group exhibiting reduced DFS. A study used tissue microarray technology and immunohistochemistry to detect CXCR4 protein expression in 110 lung cancer tissues and 12 corresponding normal lung tissues. The results showed that CXCR4 protein was primarily expressed on the cell membrane and in the cytoplasm, with positive expression rates increasing in corresponding normal lung tissue, lung adenocarcinoma, lung squamous cell carcinoma, and small cell lung cancer, respectively, at 8.3%, 87.1%, 65.2%, and 100%. Additionally, CXCR4 protein expression was closely associated with lung cancer tissue type and the invasive and metastatic capacity of lung cancer tissue [57]. Additionally, studies have reported that the CXCR4/FOXM1/RRM2 axis is regulated by miR-1, thereby inhibiting the growth and metastasis of SCLC [103].
Multiple studies have demonstrated that cancer cells with high CXCR4 expression exhibit increased tumor cell growth, invasion, and metastasis. In summary, increased CXCR4 expression indicates poor prognosis across various cancer types. The CXCR4 receptor, which uses chemokine CXCL12 as its ligand, is overexpressed in SCLC patient samples and serves as the primary chemokine receptor in primary SCLC cells [104].
When chemotherapy is combined with CXCR4 inhibitors, it reduces tumor growth to levels comparable to those achieved with combination chemotherapy alone. Combination therapy with chemotherapy and CXCR4 antagonists can reduce metastasis in SCLC. In summary, combination therapy holds significant potential for clinical application, potentially improving overall survival rates and quality of life for SCLC patients [105].
5. Molecular Targeted Therapy Strategies for CXCR4
As a key regulatory molecule involved in tumor progression, CXCR4 plays a pivotal role in mediating tumor cell migration, invasion, angiogenesis, and immunosuppressive microenvironment formation, which are closely associated with tumor metastasis and poor prognosis (Section 3 has elaborated on its multi-level regulatory mechanisms). The abnormal activation of CXCR4 and its regulatory network provides important targets for tumor targeted therapy, and precise targeting of CXCR4 has become a promising strategy to inhibit tumor metastasis and improve clinical outcomes.
Exploration of CXCR4-Targeted Therapeutic Strategies
Based on a deep understanding of the CXCR4 regulatory network, various targeted therapy strategies have been developed. For example, in terms of small-molecule inhibitor regulation, Daniela Di Paolo’s team noted that co-targeting miR-126-3p and miR-221-3p inhibits PIK3R2 and PTEN, thereby blocking AKT and CXCR4 signaling pathways to reduce lung cancer growth and metastasis [94]. Similarly, miR-9a-5p targets CXCR4 to inhibit MAPK/ERK pathway activation, alleviating lung injury [90,106]. In natural compounds, Matteo Gallazzi’s team found that the A009 extract from Olive Mill Wastewater (OMWW), rich in soluble polyphenols, can reduce lung cancer cell lines migration in vivo through dual inhibition of CXCR4/CXCL12 [107]. Clinically, lidocaine disrupts the CXCL12/Ca^2+^ pathway, significantly slowing NSCLC A549 cell migration [108]. Furthermore, specific CXCR4 antagonists, such as AMD3100, can reduce metastasis by competitively binding to CXCR4 [109].
Combination therapy strategies also show promising results. For example, gefitinib, which upregulates CXCR4 and EMT in PC9 lung adenocarcinoma cells, relies on TGF-β1/Smad2 signaling. Blocking CXCR4 significantly inhibits gefitinib-induced migration, increasing EMT reversal in PC9 lung adenocarcinoma cells in vitro [110]. Notably, CXCR4 antagonists can reverse the pro-metastatic microenvironment induced by cisplatin, reducing metastatic-initiating cells and decreasing inflammatory factor release of CCL2 and CXCL12, respectively [111]. In radiation therapy, the CXCR4/STAT3/Slug pathway confers radiation resistance, whereas siRNA-mediated Slug knockout increases radiation sensitivity. Notably, engineered locked dimerized CXCL12 has been reported to exert radiosensitizing effects by targeting the CXCR4 axis, providing a novel strategy for enhancing radiation therapy efficacy in CXCR4-positive tumors [112], which aligns with the critical role of the CXCL12/CXCR4 axis in maintaining cancer stem cells (CSCs) and inducing tumor dissemination, while also increasing chemotherapy resistance [113]. For example, CXCR4 influences tumor cell resistance through the CXCR4/STAT3 signaling pathway in chemotherapy resistance mediated by bone marrow stromal cells in acute myeloid leukemia [114]. Recent studies have revealed the potential mechanism by which the CXCR4/STAT3/Slug signaling pathway is involved in NSCLC cell radiation resistance. Slug has been identified as the downstream effector molecule of the CXCR4/STAT3 signaling pathway in NSCLC cell radiation resistance, and CXCR4-mediated STAT3 activation is crucial for NSCLC cell radiation resistance. Upregulation of Slug via the CXCR4/STAT3 signaling pathway and siRNA-mediated downregulation can enhance the sensitivity of NSCLC cells to ionizing radiation (IR). This suggests that the CXCR4/STAT3 signaling pathway could serve as a therapeutic target to enhance NSCLC cell sensitivity to IR, offering potential for targeting CXCR4 signaling pathway inhibition and eliminating NSCLC tumor stem cells. Blocking the CXCR4/STAT3 pathway may be an effective method to enhance NSCLC cell sensitivity to IR, thereby providing beneficial assistance for NSCLC radiotherapy [115].
In immunotherapy, CXCR4 exhibits a cell-type-dependent dual role Table 1. Specifically, CXCR4 antagonists target CXCR4 expressed on immunosuppressive cells rather than tumor cells, and their combination with PD-1 inhibitors shows positive synergistic effects: this combination increases CD8+ T cell infiltration and reduces Treg proportions in the tumor microenvironment, thereby extending survival in the MC38 model. In contrast, when the proportion of CXCR4+ Tregs in peripheral blood exceeds 25%, the objective response rate of immunotherapy decreases by 42%, and progression-free survival is shortened by 5.3 months—consistent with the role of CXCR4 in mediating Treg recruitment to the tumor microenvironment and suppressing anti-tumor immunity. In terms of microenvironment remodeling, CXCR4-targeted therapy promotes the formation of tertiary lymphoid structures, increasing tertiary lymphoid structures (TLS) numbers by 3.5 per field of view and significantly enhancing antigen presentation efficiency. Additionally, in a human melanoma PES43 xenograft model expressing PD-1, the combination of the human-specific CXCR4 antagonist Pep R54 with nivolumab also demonstrated tumor growth inhibition effects [116]. Further studies indicate that the combination of CXCR4 antagonists and PD-1 blockade holds significant potential in hepatocellular carcinoma (HCC) models. Concurrent blockade of CXCR4 and PD-1 can reprogram conventional type 1 dendritic cells (cDC1s) within tumors, thereby enhancing antitumor immune responses [117]. In breast cancer, the combination of the CXCR4 antagonist balixafortide with anti-PD-1 therapy has demonstrated significant therapeutic potential. The combination therapy not only reduced tumor growth and prolonged overall survival but also increased the formation of TLS in the tumor microenvironment, as shown by histological analysis. Further single-cell RNA sequencing analysis indicated that this combination therapy reduced the expression of immune checkpoint genes and exhaustion markers in T cells, suggesting a overall reduction in myeloid-mediated immune suppression [118].
In immunotherapy prediction, particularly in NSCLC studies, CXCR4 and its interactions with the immune microenvironment have emerged as critical factors influencing the efficacy of immunotherapy. In patients with stage IA to IIB NSCLC who underwent surgery, studies have shown that CXCL12 is expressed in most NSCLC tissue sections, and its expression levels are closely associated with the degree of tumor inflammation. Specifically, the co-existence of CXCL12 and activated TILs CD4^+^CXCR4^+^CD69^+^ cells may influence tumor progression by shaping the immune cell population infiltrating lung adenocarcinoma [59]. In this context, CXCR4 blockade has been found to potentially increase the number of tumor-infiltrating T lymphocytes and exhibit synergistic effects with immune checkpoint inhibitors. However, high CXCR4 expression in peripheral T lymphocytes may be associated with poorer immunotherapy efficacy, suggesting that CXCR4 plays a complex role in immunotherapy. These findings highlight the dual role of CXCR4 in immunotherapy across different tumor types: it may enhance immunotherapy efficacy in some cases while potentially weakening it in others, depending on its specific function and expression pattern within the tumor microenvironment (Figure 3).
6. Outlook
In terms of disease diagnosis and treatment, the expression levels of CXCR4 may vary across different types of tumors, potentially serving as a biomarker for disease prognosis and a potential drug target [9]. In NSCLC, CXCR4 expression levels could serve as a novel tumor marker for predicting patient outcomes. Higher CXCR4 expression in NSCLC has been linked to shorter overall survival (OS) [19]. In a study of 2932 lung cancer patients, high CXCR4 expression was associated with shorter OS and disease-free survival compared to low expression. In NSCLC, poor overall survival was significantly associated with CXCR4 expression in the cell membrane and cytoplasm. The study also showed that CXCR4 expression is associated with male gender, advanced tumor stage, advanced nodular stage, distant metastasis, advanced TNM staging, and epidermal growth factor receptor expression. However, it is not associated with age, smoking history, histopathology, lymphatic invasion, or local recurrence [23]. However, the current detection of CXCR4 expression lacks a standardized system, with inconsistent immunohistochemistry interpretation criteria and mRNA quantification methods employed across different studies. Therefore, the clinical applicability of CXCR4 as a prognostic biomarker still requires validation through multicenter large-scale studies.
Given the important role of CXCR4 in NSCLC, its genetic and structural characteristics have also attracted widespread attention. Research indicates that CXCR4 is translated into five different splice variants of varying lengths, each with distinct amino acids at the N-terminal end. Since the N-terminal end is the first recognition site for chemokines, CXCR4 variants may exhibit different responses to CXCL12. Hee-Kyung Park’s team [82] explored CXCR4 variants expression in cell lines and found that most cell lines express more than one variant. The N-terminal sequence of each CXCR4 variant determines receptor expression and influences ligand recognition. Functional analyses suggest that CXCR4 variants may also interact or influence each other during CXCL12-stimulated cellular responses. These findings suggest that CXCR4 variants could have unique functional roles warranting further investigation and may pave the way for new drug interventions, particularly for lung cancer. The impact of N-terminal sequence variations among CXCR4 splice variants on ligand recognition affinity, downstream signal transduction specificity, and tumor subtype adaptability remains a critical scientific question to be urgently elucidated in this field.
Additionally, Nanako Kawaguchi’s team revealed through studies using gene-knockout mice that CXCR4 is involved in cardiac development and brain development. Mice with homozygous CXCR4 knockout died before birth. Thus, CXCR4 is a key molecule for normal development. Interestingly, CXCL12-expressing cells are present in the outflow tract, while CXCR4^+^ cells are found in the neural cREST. Thus, CXCR4 may be involved in the migration of neural cREST cells during normal development [119]. The core regulatory role of CXCR4 in normal physiological processes provides an important reference for reverse inference of its aberrant activation mechanisms in tumors, yet the molecular regulatory network connections between the two remain to be further elucidated.
In terms of therapeutic development, several small molecules antagonizing CXCR4 have been created [120]. The FDA-approved first CXCR4 antagonist, plerixafor (AMD3100), is currently used to mobilize hematopoietic stem cells for the treatment of non-Hodgkin lymphoma [10,119] and has been shown not to exhibit cross-resistance with T134 (another small-molecule CXCR4 inhibitor that binds to CXCR4) [121]. Similarly, MSX-122 for vascular diseases and AMD11070 for HIV treatment have completed clinical trials [10]. A C-terminally modified small cyclopeptide, LY2510924 [116], will also serve as a universal scaffold for developing CXCR4-targeted probes or therapeutic agents for tumor imaging or treatment [122]. Additionally, an anti-CXCR4 antibody, LY2624587 has been developed for targeting tumors and cancers [105,118]. Additional CXCR4 antagonists are listed in Table 2.
Current clinical application of CXCR4-targeted therapeutics remains challenged by side effects such as hematopoietic suppression and infection risk, necessitating formulation optimization (e.g., tumor microenvironment-responsive preparations) and adjustment of combination regimens to reduce systemic toxicity and enhance tumor targeting specificity. Meanwhile, the development and clinical translation of CXCR4-specific molecular imaging probes (such as 68Ga-pentixafor PET) hold promise for integrating precise patient selection with dynamic monitoring of therapeutic efficacy. Moreover, the crosstalk mechanisms between CXCR4 and signaling pathways including PI3K/AKT, MAPK/ERK, and Wnt/β-catenin provide novel insights for developing multi-target combination therapeutic strategies, which will require validation of their efficacy and safety through additional preclinical and early-phase clinical studies in the future.
7. Conclusions
CXCR4 has emerged as a promising diagnostic and therapeutic target in lung cancer due to its abnormal high expression in both NSCLC and SCLC, with significant histological subtype heterogeneity, and strong association with tumor progression. Research indicates that CXCR4 expression correlates with the invasiveness and metastatic potential of lung cancer and directly impacts patient prognosis—especially in adenosquamous carcinoma (ASC), high CXCR4 expression is closely associated with lymph node metastasis and advanced TNM staging, serving as an independent poor prognostic factor. As a crucial regulator of tumor cell migration and invasion, CXCR4 may also modulate tumor immune responses by influencing immune cell function within the tumor microenvironment, such as recruiting myeloid-derived suppressor cells and activating regulatory T cells. CXCR4 expression is regulated at transcriptional (transcription factor binding, DNA methylation), post-transcriptional (miRNA/lncRNA ceRNA network), and post-translational (phosphorylation, ubiquitination, glycosylation)multiple levels, and its expression levels can serve as a prognostic biomarker for lung cancer and represent a potential drug target. Recent research advances indicate that CXCR4-targeted therapy—including small-molecule antagonists, anti-CXCR4 antibodies, and combination strategies with chemotherapy, immunotherapy, or targeted therapy—shows promising potential in enhancing treatment efficacy and reducing tumor recurrence, offering new directions for future treatment strategies. However, the exact mechanisms of CXCR4 in lung cancer and its role as an optimal therapeutic target require further clarification.
8. Discussion
As summarized earlier, CXCR4 acts as a core regulatory hub in lung cancer, integrating multiple oncogenic processes including tumor cell proliferation, invasion, distant metastasis, tumor microenvironment (TME) remodeling, and chemoresistance, which collectively supports its potential as a translational therapeutic target. Despite this well-established theoretical basis, current research progress and clinical translation of CXCR4-targeted strategies still face multiple unresolved bottlenecks. At the basic research level, the functional specificity of CXCR4 splice variants remains undefined—the impact of N-terminal amino acid sequence variations on ligand binding affinity and downstream signal transduction lacks systematic validation, precluding explanation of differential responses to targeted therapy among patients. Simultaneously, bidirectional regulatory mechanisms between CXCR4 and stromal/immune cells in the tumor microenvironment remain poorly understood, particularly the regulatory threshold for tumor progression concerning the synergistic/competitive relationship between the CXCL12/CXCR4 axis and CXCR7. At the clinical translation level, the primary issue is the lack of a standardized system for CXCR4 expression detection, with inconsistent immunohistochemistry interpretation criteria and mRNA quantification methods across studies, limiting its clinical applicability as a prognostic biomarker. Second, current CXCR4 antagonists exhibit side effects including hematopoietic suppression and infection risk, with insufficient tumor tissue targeting, and mature solutions for toxicity reduction through formulation optimization or combination regimens have yet to be established. Furthermore, predictive models for CXCR4-targeted therapy response in lung cancer patients with different pathological subtypes and genetic backgrounds (e.g., EGFR mutations, ALK fusions) remain undeveloped, and precise identification of beneficiary populations remains a critical issue requiring urgent breakthrough. Finally, research on mechanisms of CXCR4-mediated chemoresistance in SCLC lags behind that in NSCLC, with clinical exploration of related targeted strategies still in early stages. Future studies should advance the precision application of CXCR4-targeted strategies. At the basic research level, it is necessary to thoroughly investigate the functional heterogeneity of CXCR4 splice variants and clarify their expression profiles and regulatory networks across different lung cancer subtypes. Simultaneously, through technologies such as single-cell sequencing and spatial transcriptomics, elucidate the cell-specific functions of CXCR4 in the tumor microenvironment and reveal its synergistic regulatory mechanisms with immune checkpoint molecules. In the field of technology development, clinical translation of CXCR4-specific molecular probes should be promoted. Meanwhile, optimize targeted drug design and develop tumor microenvironment-responsive novel antagonists or antibody-drug conjugates (ADCs) to enhance targeting specificity and reduce systemic toxicity. At the clinical translation level, multicenter, large-scale clinical studies are needed to validate the synergistic prognostic value of CXCR4 expression with existing clinical indicators (such as TNM staging, genetic test results) and establish standardized detection protocols. Design individualized combination therapy regimens for different lung cancer subtypes, such as combining CXCR4 antagonists with PD-1/PD-L1 inhibitors in NSCLC and with chemotherapy agents in SCLC. Future research should focus on the following key questions: First, how can the CXCR4 pathway be precisely targeted to improve patient treatment responses? Second, can CXCR4 expression serve as a reliable biomarker for predicting patient responses to specific treatments? Additionally, can the combination of CXCR4-targeted therapy with other treatment methods (such as immunotherapy) yield more significant therapeutic effects? The answers to these questions will have a significant impact on the application of CXCR4 in lung cancer treatment and may provide patients with more effective treatment options. By thoroughly exploring the mechanism of action of CXCR4 and its integration with other treatment strategies, future research holds promise for bringing new hope to lung cancer patients (Figure 4).
In summary, relying on its core regulatory role in lung cancer progression, CXCR4 remains a highly translational therapeutic target. The success of its clinical application depends on in-depth analysis of core mechanisms, effective breakthrough of technical bottlenecks, and precise optimization of clinical protocols. In the future, through interdisciplinary collaboration, it is expected to provide new treatment options for lung cancer patients and ultimately improve patient prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smolarz B. Łukasiewicz H. Samulak D. Piekarska E. Kołaciński R. Romanowicz H. Lung Cancer—Epidemiology, Pathogenesis, Treatment and Molecular Aspect (Review of Literature)Int. J. Mol. Sci.202526204910.3390/ijms 2605204940076671 PMC 11900952 · doi ↗ · pubmed ↗
- 2Abdelaziz H.M. Gaber M. Abd-Elwakil M.M. Mabrouk M.T. Elgohary M.M. Kamel N.M. Kabary D.M. Freag M.S. Samaha M.W. Mortada S.M. Inhalable particulate drug delivery systems for lung cancer therapy: Nanoparticles, microparticles, nanocomposites and nanoaggregates J. Control. Release 201826937439210.1016/j.jconrel.2017.11.03629180168 · doi ↗ · pubmed ↗
- 3Zhao D. Deshpande R. Wu K. Tyagi A. Sharma S. Wu S.-Y. Xing F. O’N Eill S. Ruiz J. Lyu F. Identification of TUBB 3 as an immunotherapy target in lung cancer by genome wide in vivo CRISPR screening Neoplasia 20256010110010.1016/j.neo.2024.10110039671912 PMC 11699798 · doi ↗ · pubmed ↗
- 4Jin M. Huang Y. Li B. Wang Y. Li Y. Chen Z. Tang Z. Liu C. Zhang L. Yuan X. Genetic Regulation of Alternative Polyadenylation Provides Novel Insights into Molecular Mechanisms Underlying Non-small Cell Lung Cancer Adv. Sci.202512 e 250200810.1002/advs.202502008 PMC 1224500640285671 · doi ↗ · pubmed ↗
- 5Cao Z. Meng Z. Li J. Tian Y. Lu L. Wang A. Huang J. Wang J. Sun J. Chen L. Interferon-γ-stimulated antigen-presenting cancer-associated fibroblasts hinder neoadjuvant chemoimmunotherapy efficacy in lung cancer Cell Rep. Med.2025610201710.1016/j.xcrm.2025.10201740056907 PMC 11970394 · doi ↗ · pubmed ↗
- 6Li Y. Yan B. He S. Advances and challenges in the treatment of lung cancer Biomed. Pharmacother.202316911589110.1016/j.biopha.2023.11589137979378 · doi ↗ · pubmed ↗
- 7Katoh M. Katoh M. Integrative genomic analyses of CXCR 4: Transcriptional regulation of CXCR 4 based on TGFβ, Nodal, Activin signaling and POU 5F 1, FOXA 2, FOXC 2, FOXH 1, SOX 17, and GFI 1 transcription factors Int. J. Oncol.20103641542010.3892/ijo_0000051420043076 · doi ↗ · pubmed ↗
- 8Mezzapelle R. Leo M. Caprioglio F. Colley L.S. Lamarca A. Sabatino L. Colantuoni V. Crippa M.P. Bianchi M.E. CXCR 4/CXCL 12 Activities in the Tumor Microenvironment and Implications for Tumor Immunotherapy Cancers 202214231410.3390/cancers 1409231435565443 PMC 9105267 · doi ↗ · pubmed ↗