Clinical Validation of rPPG-Enabled Contactless Pulse Rate Monitoring Software in Cardiovascular Disease Patients
Jing Wei Chin, Po Him David Chan, Shutao Chen, Chun Hong Cheng, Richard H. Y. So, Elaine Chow, Benny S. P. Fok, Kwan Long Wong

TL;DR
This study shows that contactless camera-based pulse rate monitoring is accurate for patients with cardiovascular disease, offering a promising tool for remote health tracking.
Contribution
The study provides clinical validation of rPPG for pulse rate monitoring in CVD patients, demonstrating its accuracy and robustness.
Findings
rPPG-derived pulse rate showed strong agreement with ECG with a mean absolute error of 1.061 bpm.
Demographic and environmental factors had minimal influence on rPPG accuracy in CVD patients.
PPG-ECG discrepancies were attributed to methodological differences rather than rPPG inaccuracy.
Abstract
Background: Cardiovascular disease (CVD) is the leading cause of mortality worldwide, creating demand for continuous, unobtrusive monitoring solutions. This clinical validation evaluates the accuracy of remote photoplethysmography (rPPG), a contactless method using camera video, for measuring pulse rate (PR) in patients with CVD. Methods: We enrolled 50 adults with confirmed CVD at a clinical trial center. In a 6 min rested session, synchronized facial video (under controlled lighting), electrocardiogram (ECG), and photoplethysmography (PPG) signals were recorded. PR was derived from 25 s video segments using rPPG-enabled software and compared to ECG-derived PR via regression and Bland–Altman analysis. Results: Data from 47 participants (n = 817 samples) were analyzed. rPPG-derived PR showed strong agreement with ECG, with a mean absolute error of 1.061 bpm, root-mean-squared error of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
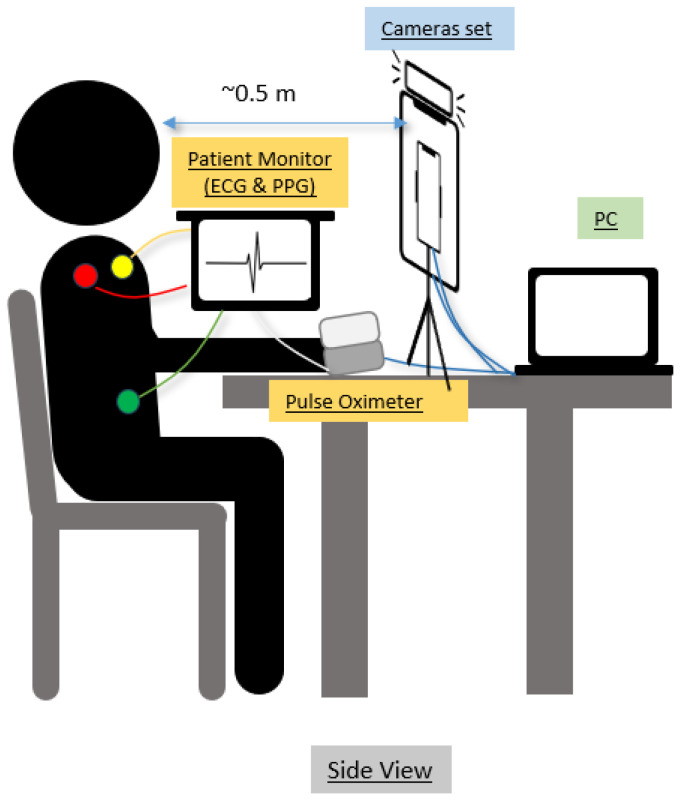 Figure 1
Figure 1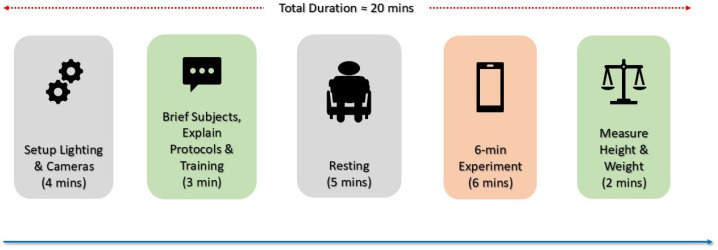 Figure 2
Figure 2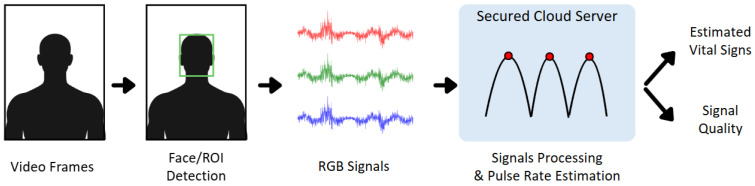 Figure 3
Figure 3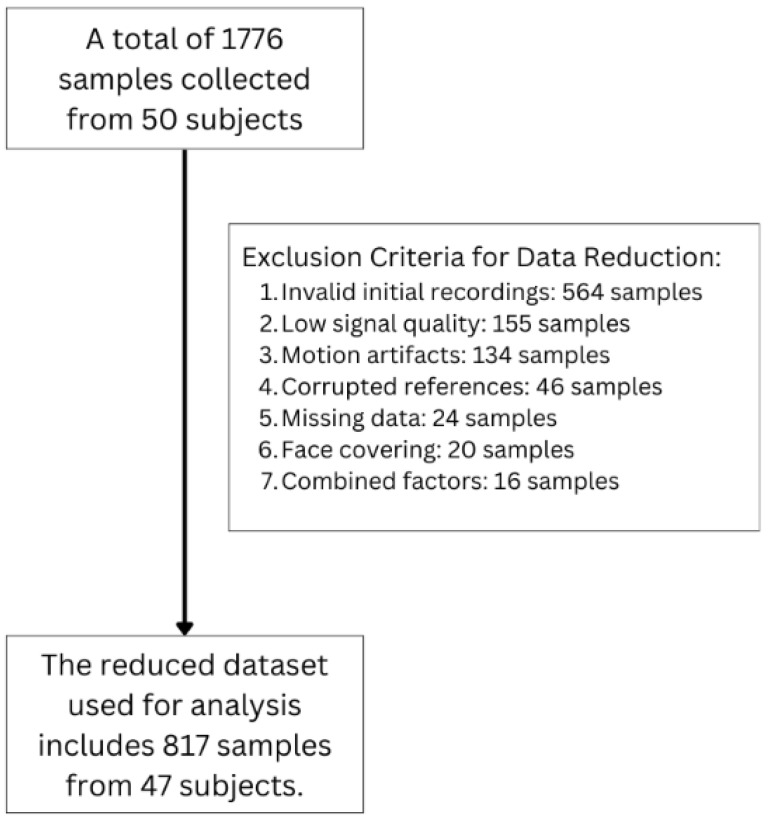 Figure 4
Figure 4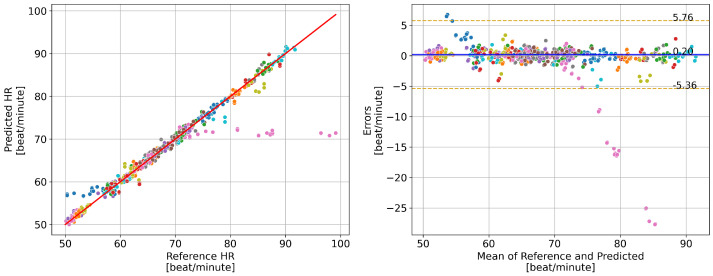 Figure 5
Figure 5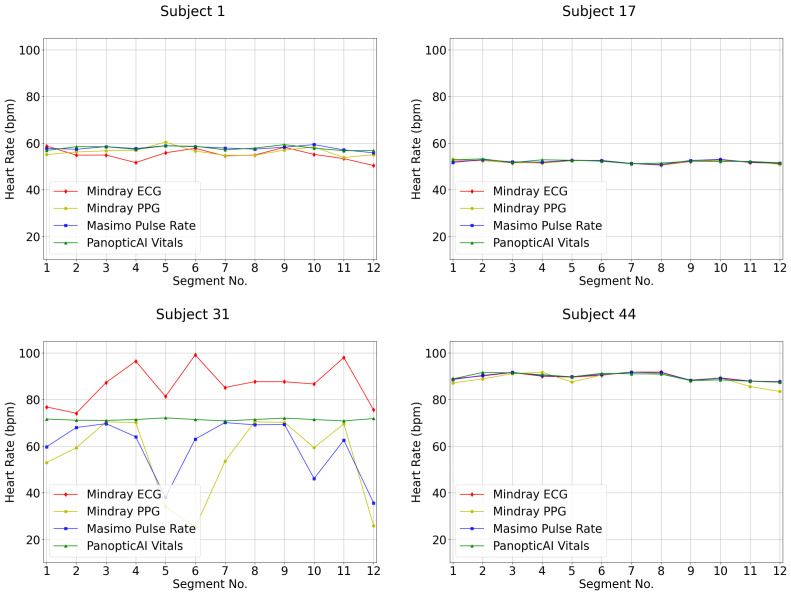 Figure 6
Figure 6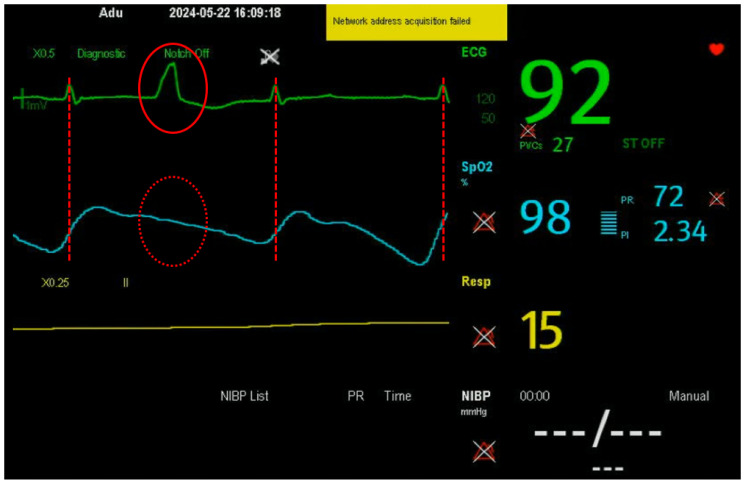 Figure 7
Figure 7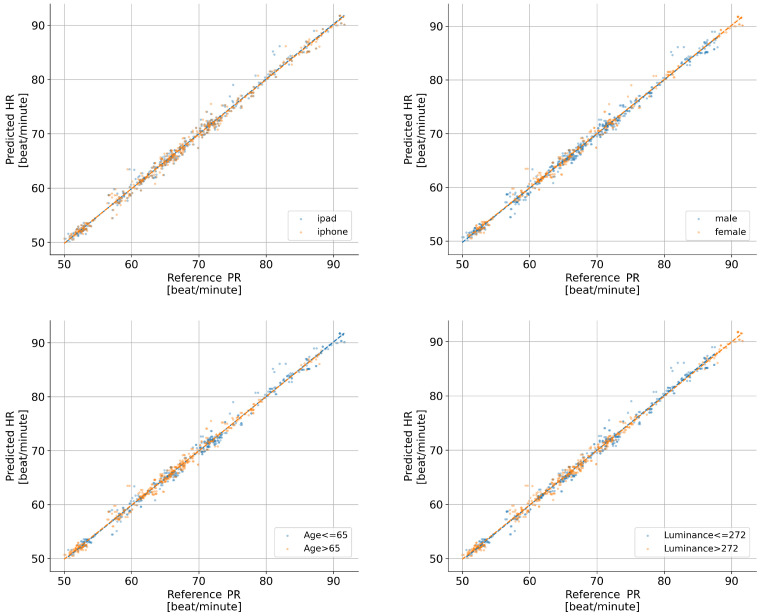 Figure 8
Figure 8- —Innovation Technology Commission of Hong Kong
- —Hong Kong Science and Technology Parks Corporation MedTech Co-create Funding Scheme
- —HKUST’s Sports Development Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNon-Invasive Vital Sign Monitoring · Heart Rate Variability and Autonomic Control · Hemodynamic Monitoring and Therapy
1. Introduction
CVD remains the leading cause of mortality worldwide, responsible for 17.9 million deaths annually, accounting for 32% of all deaths [1]. While advancements in prevention and treatment have reduced mortality in high-income regions, low- and middle-income countries continue to account for more than 75% of CVD-related deaths due to limited healthcare access and delayed interventions [1]. The economic burden is substantial, with projected annual costs expected to exceed 1 trillion USD by 2030 [2]. Notably, ischemic heart disease and stroke alone contribute to of all CVD deaths [3]. Given the persistent impact of CVD, innovative monitoring solutions are crucial for early detection and intervention.
PR is a key physiological marker of cardiovascular health, with elevated resting PR associated with increased myocardial oxygen demand and adverse cardiac outcomes [4]. Traditional PR monitoring relies on ECG or clinical assessments that require specialized equipment and are often inaccessible in resource-limited settings. Moreover, prolonged use of wearable sensors may be inconvenient for certain patients and can be unsuitable in cases where the skin is sensitive or medically compromised, such as during recovery from dermatological conditions or surgical procedures [5,6].
rPPG has emerged as a promising and non-invasive alternative to conventional contact-based methods for continuous vital sign monitoring using an RGB camera [7,8,9,10,11,12]. The rPPG technique leverages recordings from an RGB camera to capture the subject’s face and applies algorithms to detect subtle skin color fluctuations resulting from blood volume changes, eliminating the need for physical sensors, enhancing accessibility, comfort, and adherence [13,14,15,16]. Unlike contact-based methods, rPPG can be deployed on widely available hardware, including specialized cameras and consumer smartphones or tablets, reducing barriers to vital sign monitoring. This accessibility supports longitudinal cardiovascular assessment and early CVD risk detection [17,18]. Recent employment of deep learning technology further improves the robustness and accuracy of rPPG-derived measurements [19,20,21,22,23]. However, the primary challenge of rPPG lies in its reliability. Its performance in individuals with CVD, who may exhibit irregular cardiac rhythms or compromised circulation, has only recently begun to be systematically evaluated [24], and further clinical validation is required to determine its feasibility for reliable cardiovascular monitoring across a wide range of clinical scenarios.
The primary objective of this study was to evaluate the accuracy of contactless PR estimation in patients with CVD in Hong Kong using a proprietary rPPG algorithm. To achieve reliable PR measurements, we adopted a medical-grade rPPG-derived vital sign monitoring software developed by Wong et al. [25]. The software is commercialized by PanopticAI Technologies Limited, a Hong Kong-based company, and has received FDA Class II clearance (K240890) [26]. While the software has demonstrated strong performance in the general population, its applicability to CVD patients has not been previously validated. To address this gap, we conducted a clinical evaluation of the rPPG-enabled software for PR monitoring in individuals diagnosed with CVD. Data collection was carried out in collaboration with the Prince of Wales Hospital (PWH) at the Phase 1 Clinical Trial Centre (P1CTC), under ethics approval No. 2023.408. The results indicate that the rPPG-enabled software provides reliable and consistent PR measurements in CVD patients, demonstrating robustness across different devices and demographic subgroups.
2. Materials and Methods
2.1. Experimental Setup
Before data collection, all participants underwent a standardized medical screening administered by qualified healthcare professionals. Exclusion criteria included the presence of pacemakers or implantable cardioverter-defibrillators (ICDs); use of topical facial products (including makeup) on the day of assessment; clinically significant diseases that could affect study outcomes, as determined by the investigators; and any other factors deemed by the investigators to make the participant unsuitable for the study. Following informed consent, the baseline characteristics of the participants, including gender, height, weight, and medical history, were recorded. They were instructed to remove personal accessories (including face covers and electronic devices) and sit quietly in a controlled environment for 5 min to stabilize before the experiment began.
A patient room in P1CTC was designated as the experiment room, and its illumination levels, temperature, and humidity were recorded using specialized sensors. All devices were tested for adequate storage capacity and functionality.
2.2. Device Configuration
Two cameras—an iPhone 13 Pro and an iPad Air (5th generation) manufactured by Apple Inc., San Jose, CA, United States—were mounted on a tripod at eye level to capture consistent facial footage of the participant. A reference timer ensured synchronization across devices.
This study utilized multiple reference devices for monitoring participants’ physiological parameters. As illustrated in Figure 1, we attached three ECG electrodes on the shoulders and left abdomen, along with a blood pressure cuff (USCOM BP+, USCOM Ltd., Sydney, Australia) on the left arm. To monitor photoplethysmography, we utilized two photoplethysmography sensors: the Mindray iMEC8 patient monitor sensor (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) on the right index finger and the Masimo MightySat Pulse Oximeter (Masimo Corporation, Irvine, CA, USA) on the right middle finger. The Masimo MightySat Pulse Oximeter streamed data to a mobile app for real-time monitoring. We integrated all devices, including both the Mindray monitor and Masimo MightySat Pulse Oximeter, with a central PC to maintain data synchronization. The specifications and settings of each device are shown in Table 1.
2.3. Data Collection Protocol
The data collection timeline is illustrated in Figure 2. The experimental protocol required approximately 20 min per participant, with the core assessment period lasting 6 min. Prior to data collection, investigators systematically calibrated and validated all lighting conditions and camera configurations. Nurses provided participants with standardized instructions on the experimental protocol to ensure adherence to study procedures. Subjects rested for 5 min prior to measurement to allow physiological stabilization. The 6 min assessment phase required participants to remain seated while following visual instructions presented on the monitoring device. Throughout this period, video recording across both the iPhone and iPad together with continuous physiological measurements (ECG and PPG) were obtained. Post assessment, anthropometric measurements (height and weight) were documented, followed by secure data transfer and archival for subsequent processing and analysis.
2.4. Data Processing
During data processing, the first minute of each 6 min resting video was excluded to account for sensor warm-up artifacts. The remaining 5 min segment was divided into twelve 25 s clips for analysis. As shown in Figure 3, each clip underwent a fixed processing pipeline adapted from established rPPG-derived vital sign monitoring software [25]. A face detector performed frame-by-frame face localization with tracking and facial landmark detection to define and stabilize cheek regions of interest (ROIs). Pre-processing, including skin masking and spatial filtering, was applied to reduce non-skin contamination, motion-related noise, and illumination-related variability before ROI signal extraction. Temporal, anonymized RGB signals were extracted from the ROIs and transmitted to a secured cloud server, where fixed signal-processing algorithms were applied to derive the rPPG waveform. Pulse rate was then estimated in the frequency domain by bandpass filtering the rPPG signal to the physiological heart-rate range and identifying the dominant spectral peak. A proprietary signal quality metric was computed per clip and used to exclude low-quality samples. Finally, pulse rates meeting the quality threshold were validated against synchronized reference measurements from an FDA-cleared Mindray iMEC8 patient monitor.
Figure 4 illustrates the data cleaning protocol implemented in this study. Low signal quality was automatically flagged on the cloud server using a proprietary signal-quality metric (Figure 3), and samples below the predefined threshold were excluded. Although the processing pipeline includes face detection and tracking to maintain ROI alignment under subtle facial motion, clips with pronounced motion (e.g., head turning, large translational movement) or facial obstructions (e.g., occlusion, turning away) were excluded based on manual video review by trained reviewers. For invalid initial recordings, defined as those compromised by protocol non-compliance, improper camera setup, or subject drowsiness during acquisition, additional recordings were acquired whenever feasible to ensure protocol adherence. Additional exclusions included corrupted reference signals, missing data, and combined factors. After this multi-tier screening, the final dataset comprised 817 valid samples from 47 participants for subsequent analysis. For future clinical deployment, automated or standardized procedures to detect and handle large-motion and obstruction cases, together with supervision by trained medical personnel to ensure adequate use (i.e., remaining still and breathing naturally), should be considered to reduce the risk of inaccurate estimates.
To quantify the agreement between the estimated and reference pulse rates, we computed the mean absolute error (MAE), root-mean-squared error (RMSE), and Pearson correlation (R) according to the following equations:
where denotes the estimated pulse rate, denotes the reference pulse rate, and K represents the total number of samples.
3. Results
3.1. Demographic Statistics
Table 2 presents the demographic characteristics and environmental conditions of the study cohort. The final dataset included 817 measurements collected from 47 participants, with an age distribution spanning 44 to 80 years (male: n = 17; female: n = 30). The mean ambient temperature recorded by environmental monitoring was 22.47 °C with an averaged relative humidity of 67.76%. Illuminance levels ranged from 126 to 547 lux across experimental sessions. The distribution of participants across different medical conditions is presented in Table 3.
3.2. PR Measurements
The results of PR measurements are presented in Figure 5. The estimation achieved high accuracy, with an MAE of 1.061 bpm, an RMSE of 2.845 bpm, and R of 0.962. The Bland–Altman plot reveals that most prediction errors fall within the range of −5.36 to 5.76 bpm. Two subjects exhibited anomalies: Subject ID 1 (marked with blue points) and Subject ID 31 (marked with pink points). For Subject ID 1, the rPPG-derived PR was around 58 bpm while the reference ECG-derived PR varied between 50 and 60 bpm. For Subject ID 31, the rPPG-derived PR remained around 72 bpm, while the reference ECG-derived PR ranged between 72 bpm and 100 bpm. These discrepancies are consistent with known modality differences between ECG-derived and peripheral pulse-based (PPG/rPPG) measurements and highlight potential limitations of rPPG in real-world clinical settings. Overall, the rPPG-enabled software achieved accurate PR estimation in CVD subjects (see Section 4.1). However, the two anomalous cases may reflect transient rhythm irregularities (e.g., ectopic beats), which may not be reliably captured by PPG/rPPG, highlighting a potential limitation under arrhythmic conditions.
4. Discussion
4.1. Disparity Between PPG and ECG
Given that subjects remained seated and relaxed, the rPPG-derived pulse rate was expected to align closely with the ECG reference. However, a notable short-term discrepancy was observed (Figure 6). This stems from a fundamental measurement difference: ECG captures direct cardiac electrical activity, making it highly sensitive to transient rhythm changes [27,28], while rPPG and PPG measure peripheral blood volume changes to determine pulse rate from pulse wave peaks [29,30,31]. As shown in Figure 7, an extra ECG peak absent in the PPG signal indicates a ventricular ectopic beat that did not produce a sufficient peripheral pulse. This explains the closer rPPG-PPG agreement and the ECG discrepancy: the optical methods correctly followed the dampened hemodynamic signal.
This inherent limitation of hemodynamic-based monitoring is well-documented. PPG signals are subject to mechanical smoothing during vascular propagation, making them less sensitive to brief, non-perfusing ectopic events compared to ECG, which precisely tracks R–R intervals [27,28]. Therefore, the observed discrepancy highlights the complementary nature of these modalities: ECG excels at detecting fine-grained electrical activity and arrhythmias, while optical methods like rPPG provide stable, convenient monitoring of perfused pulse trends. The clinical records of the affected subjects, who had hypertension, a condition linked to increased ectopic activity [32,33], suggest that such discrepancies may be more prevalent in certain patient groups. Importantly, because rPPG estimates PR from peripheral pulse dynamics rather than cardiac electrical activity, ectopic or non-perfusing beats may be missed, and rPPG may therefore underestimate transient arrhythmic events compared with ECG. This highlights a key limitation for contactless monitoring, and further studies are needed to evaluate rPPG performance in arrhythmic patient populations across a range of arrhythmia types. Nevertheless, a great consistency between ECG and optical-based PR measurements has been observed in most cases [34,35].
4.2. Statistical Analysis
4.2.1. Effect of Configurations
To evaluate the accuracy of rPPG-derived PR measurements against ECG reference, we employed mixed-effects linear models accounting for repeated measurements within subjects. To enhance model robustness, we removed the most extreme 2% of observations from each tail, yielding an analytic sample of 782 measurements (96% of original data). Two models were then estimated using restricted maximum likelihood (REML). Model 1 assessed the unadjusted relationship between rPPG-estimated and ECG-reference PR, while Model 2 included covariates (age, luminance, device, and gender groups). Age and luminance were dichotomized at 65 years and 272 lux, respectively, for subgroup analysis.
Visual inspection of regression plots (Figure 8) reveals the relationship between estimated and reference pulse rates across different devices, while Table 4 provides descriptive performance metrics, R, MAE, and RMSE, stratified by age, gender, luminance, and device.
For inferential analysis, mixed-effects linear models revealed excellent agreement between rPPG-estimated and reference pulse rates (Table 5). In the unadjusted model (Model 1), the regression coefficient for estimated pulse rate was 0.996 (95% CI: 0.978–1.015, SE = 0.009, ), indicating near-perfect 1:1 correspondence with ECG measurements. The adjusted model (Model 2) yielded a similar coefficient of 0.991 (95% CI: 0.966–1.016, SE = 0.013, ) after incorporating covariates. Notably, none of the covariates reached statistical significance: age group ( , SE = 0.153, ), luminance group ( , SE = 0.157, ), device group ( , SE = 0.061, ), or gender group ( , SE = 0.154, ).
Variance components indicated moderate between-subject variability (Model 1: 0.146, SE = 0.093; Model 2: 0.199, SE = 0.137) with residual variances of 0.714 and 0.705, respectively. The simpler unadjusted model demonstrated better fit with a less negative REML log-likelihood (−1016.30 vs. −1019.88), supporting its statistical parsimony. Collectively, these results indicate robust performance of the rPPG pulse rate estimation method across varying demographic and experimental conditions, with no significant subgroup differences observed in our sample.
4.2.2. Effect of CVD
In our CVD cohort (n = 47 patients, 782 observations after outlier removal), we assessed whether common cardiovascular conditions affect rPPG pulse rate accuracy. Given the distribution of medical conditions in our sample (Table 3), we focused our subgroup analysis on hyperlipidemia (53% prevalence) and type 2 diabetes (36% prevalence), which had sufficient representation in both diseased and non-diseased groups. Hypertension (85% prevalence) and other less prevalent conditions (all <7% prevalence) were excluded from subgroup analysis due to insufficient reference group sizes, which would compromise statistical validity. Mixed-effects models in Table 6 revealed no significant main effects of hyperlipidemia ( , ) or type 2 diabetes ( , ) on accuracy (Model 3). Interaction models (Model 4) similarly showed no evidence that these conditions modify the rPPG-ECG relationship (hyperlipidemia interaction: , ; diabetes interaction: , ). The core rPPG-ECG association remained strong across both models ( , ), suggesting maintained accuracy despite varying cardiovascular profiles. These findings indicate that rPPG pulse rate estimation is robust across common cardiovascular conditions. However, several limitations warrant acknowledgment: the high prevalence of hypertension (85%) precluded assessment of its independent effect, and the low prevalence of specific cardiac conditions (e.g., atrial fibrillation, 4.3%; ischemic heart disease, 6.4%) limited condition-specific evaluation. Future studies with larger, more balanced cohorts are needed to comprehensively evaluate rPPG performance across the full spectrum of cardiovascular conditions, particularly arrhythmias and acute cardiac events.
4.2.3. Effect of Skin Tone
Skin tone may affect rPPG accuracy. Since recruitment was conducted in Hong Kong, the cohort consisted entirely of Asian participants and all subjects were Fitzpatrick skin types III–IV, resulting in limited skin tone variability and precluding subgroup comparisons. Future work should validate performance in more diverse populations.
4.2.4. Effect of Lightning
Lighting conditions can influence rPPG signal quality and estimation accuracy. In this study, ambient lighting in the clinical trial center was recorded using a light meter in the experiment room, and the illuminance measured at the subject’s face was maintained at approximately 100–500 lux. Since real-world lighting may vary across environments and may fall outside this range, rPPG accuracy may deviate under suboptimal illumination (e.g., dim lighting or strong directional lighting). Accordingly, the results of this study should be interpreted as performance under the recorded lighting conditions (100–500 lux).
5. Conclusions
This study clinically evaluated a contactless pulse rate monitoring software for PR estimation in individuals with CVD. Across 47 participants and 817 valid 25 s samples, rPPG-derived PR demonstrated strong agreement with ECG-derived PR (MAE: 1.061 bpm; RMSE: 2.845 bpm; Pearson ), with most errors lying within the Bland–Altman limits of agreement (−5.36 to bpm). Two subjects exhibited anomalies consistent with known modality differences between electrical (ECG) and peripheral pulse-based measurements.
Mixed-effects regression analyses indicated that PR estimation accuracy was robust to device type (iPhone/iPad), ambient luminance, age group, and gender. Disease-stratified analysis revealed no significant effect of hyperlipidemia or type 2 diabetes on rPPG accuracy, suggesting robustness across these common metabolic conditions. However, the high prevalence of hypertension (85%) precluded assessment of its independent effect, and limited representation of specific cardiac conditions (e.g., atrial fibrillation, ischemic heart disease) restricted condition-specific evaluation. These limitations highlight the need for future validation studies with larger, more balanced cohorts to systematically examine rPPG performance across the full spectrum of cardiovascular pathology.
Overall, these results support the feasibility of accurate, contactless PR monitoring in CVD patients and its potential utility for remote patient monitoring. Future work will evaluate rPPG performance in patients with irregular rhythms (e.g., ectopic beats) and extend validation to additional vital signs and diverse cohorts to enhance clinical robustness for broader cardiometabolic risk assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Cardiovascular Diseases (CV Ds)2021 Available online: https://www.who.int/health-topics/cardiovascular-diseases(accessed on 16 February 2026)
- 2Bloom D.E. Cafiero E. Jané-Llopis E. Abrahams-Gessel S. Bloom L.R. Fathima S. Feigl A.B. Gaziano T. Hamandi A. Mowafi M. The Global Economic Burden of Non-Communicable Diseases 2011 Available online: https://ideas.repec.org/p/gdm/wpaper/8712.html?utm_medium=email&utm_source=transaction(accessed on 16 February 2026)
- 3Roth G.A. Johnson C. Abajobir A. Abd-Allah F. Abera S.F. Abyu G. Ahmed M. Aksut B. Alam T. Alam K. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015 J. Am. Coll. Cardiol.20207012510.1016/j.jacc.2017.04.052PMC 549140628527533 · doi ↗ · pubmed ↗
- 4Fox K. Borer J.S. Camm A.J. Danchin N. Ferrari R. Sendon J.L. Steg P.G. Tardif J.C. Tavazzi L. Tendera M. Resting heart rate in cardiovascular disease J. Am. Coll. Cardiol.20075082383010.1016/j.jacc.2007.04.07917719466 · doi ↗ · pubmed ↗
- 5Piwek L. Ellis D.A. Andrews S. Joinson A. The rise of consumer health wearables: Promises and barriers P Lo S Med.201613 e 100195310.1371/journal.pmed.100195326836780 PMC 4737495 · doi ↗ · pubmed ↗
- 6Shabaan M. Arshid K. Yaqub M. Jinchao F. Zia M.S. Bojja G.R. Iftikhar M. Ghani U. Ambati L.S. Munir R. Survey: Smartphone-based assessment of cardiovascular diseases using photoplethysmography BMC Med. Inform. Decis. Mak.20202017710.1186/s 12911-020-01199-732727453 PMC 7392662 · doi ↗ · pubmed ↗
- 7Mc Duff D. Camera measurement of physiological vital signs ACM Comput. Surv.20235514010.1145/3558518 · doi ↗
- 8Xiao H. Liu T. Sun Y. Li Y. Zhao S. Avolio A. Remote photoplethysmography for heart rate measurement: A review Biomed. Signal Process. Control 20248810560810.1016/j.bspc.2023.105608 · doi ↗