Hyaluronic Acid and Sodium Hypochlorite as Adjunctive Therapeutic Options for Patients with Periodontal Disease: A Systematic Review
Tomás Infante da Câmara, Francisca Abreu, Miguel Nunes Vasques, Ricardo Faria-Almeida, Honorato Ribeiro-Vidal

TL;DR
This study finds that using hyaluronic acid and sodium hypochlorite alongside standard periodontal treatment improves outcomes like reduced gum pockets and better tissue attachment.
Contribution
The study provides new evidence that combining hyaluronic acid and sodium hypochlorite with standard therapy improves periodontal outcomes.
Findings
Adjunctive therapy with hyaluronic acid and sodium hypochlorite significantly reduced probing pocket depth.
Clinical attachment level improved more with adjunctive treatment compared to standard therapy alone.
Pocket closure rates were higher in deep pockets with the adjunctive treatment.
Abstract
Background: Periodontal disease is a chronic multifactorial inflammatory condition caused by dysbiosis of the dental biofilm, leading to destruction of the connective tissue attachment, alveolar bone resorption, and potentially tooth loss. Non-surgical periodontal therapy (NSPT), involving subgingival instrumentation, aims to restore periodontal health by reducing the probing pocket depth (PPD) and bleeding on probing (BOP) and by improving the clinical attachment level (CAL). The adjunctive use of chemical agents, such as sodium hypochlorite/amino acids (NaOCl) and cross-linked hyaluronic acid (xHyA) gels, has been proposed to enhance the efficacy of NSPT. Objective: This systematic review aimed to evaluate the clinical effectiveness of the subgingival application of NaOCl and xHyA gels as adjunctive therapies to NSPT in patients with periodontal disease. Materials and Methods: A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
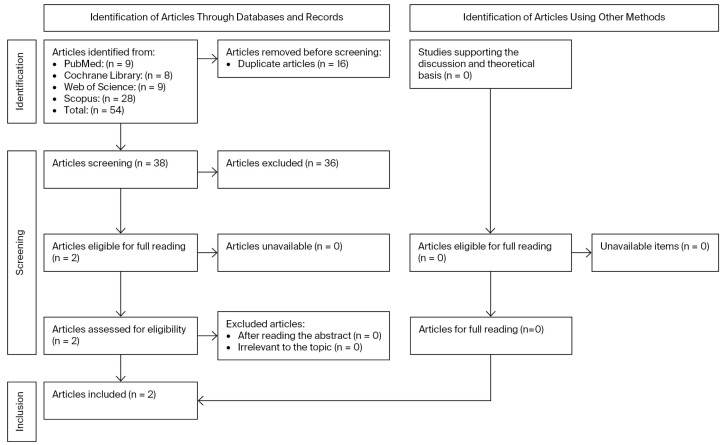 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Endodontics and Root Canal Treatments · Proteoglycans and glycosaminoglycans research
1. Introduction
Periodontal disease is a multifactorial chronic inflammatory disease. It is caused by dysbiosis of the dental biofilm, which leads to the formation of an inflammatory infiltrate that promotes the destruction of the connective tissue attachment supporting the teeth, as well as alveolar bone resorption, potentially culminating in tooth loss [1,2,3,4].
Approximately 90% of the global population may be suffering from extremely common periodontal diseases [5]. At present, one of the most prevalent diseases impacting humankind is periodontitis [5,6], with a concerning 743 million documented cases, ranking sixth in terms of prevalence, according to the Global Burden of Disease Study [7].
According to the National Health and Nutrition Examination Survey (NHANES) conducted between 2009 and 2012, 46% of adults aged 30 or older in the United States suffer from periodontitis, translating to approximately 64.7 million individuals, 8,9% of whom have severe periodontitis. The prevalence tends to increase with age, impacting over 85% of individuals older than 65 [8,9]. Likewise, in Europe, it is reported that roughly 10% of people have suffered from severe periodontal diseases, with the majority of cases occurring in adulthood [10,11,12].
Periodontitis is characterized by the alteration of healthy subgingival plaque with subsequent inflammation and tissue destruction [13,14].
The main contributory factor to periodontitis occurs with the existence of dysbiotic bacterial communities arranged in matrices of extracellular polysaccharides forming subgingival biofilms that adhere to the root surface whilst exposed to the external environment [15,16]. From a contrasting perspective, periodontal health is related to microbial communities in symbiosis with the host [15].
The hundreds of microorganisms that constitute the human oral microbiome colonize a broad variety of surfaces and are mostly organized in complex biofilms [17]. At least 800 bacterial species exist in dental plaque [18,19,20,21,22,23], yet only 54% of these species have been officially identified, 14% have been cultivated, and 32% are uncultivated phylotypes [24].
The main clinical manifestations of periodontitis include the loss of periodontal supporting tissue, translating into clinical attachment loss (CAL) and radiographic bone loss (RBL), with the presence of gingival bleeding and periodontal pockets [4].
Recent guidelines for the treatment of periodontitis stages I-III state that non-surgical periodontal therapy (NSPT) primarily aims to restore periodontal health in the supporting tissues by focusing on reducing and eliminating biofilms and subgingival calculus, decreasing pocket probing depths (PPDs) and bleeding on probing (BOP), and increasing clinical attachment levels through subgingival instrumentation using the mechanical action of curettes combined with ultrasonic devices. The efficacy of subgingival instrumentation can be enhanced by the adjunctive application of chemical agents [25,26,27,28,29,30].
The goal of NSPT is to reduce the pocket-probing depth (PPD) to 4 mm or less and minimize periodontal inflammation with the intention of pocket closure. Thus, for long-term periodontal stability, continuous supportive periodontal therapy (SPT), along with repeated instrumentation as advised by the European Federation of Periodontology (EFP) guidelines, is essential [25,31,32].
1.1. Sodium Hypochlorite
Sodium hypochlorite has been widely used as a surface disinfectant. The World Health Organization (WHO) advises hospitals to utilize disinfectants, such as sodium hypochlorite, as part of proper environmental cleaning and disinfection protocols [33].
In endodontic treatment, sodium hypochlorite (NaOCl) is the most used irrigant. Its antimicrobial and tissue-dissolving abilities make it the gold standard of root canal irrigants [34,35].
In vitro and clinical studies have demonstrated that sodium hypochlorite/amino acid gel acts as an antiseptic and is particularly effective against Gram-negative species associated with periodontitis, showing the ability to alter the biofilm matrix [36,37,38].
Laboratory studies have shown that sodium hypochlorite/amino acid gel has a softening effect on the extracellular matrix of biofilms. Subgingival mechanical instrumentation and the chemical reaction of sodium hypochlorite act synergistically in the disruption of the biofilm and the removal of granulation tissue [37,38].
It is important to emphasize that the use of sodium hypochlorite in conjunction with mechanical debridement does not negatively affect the dentin or root cementum. The high pH of sodium hypochlorite interacts with the calculus, promoting its softening, making subgingival mechanical instrumentation easier to perform [38].
1.2. Hyaluronic Acid
It is noteworthy that hyaluronic acid is the main component of the extracellular matrix of the joints, skin, and eyes, among other tissues and organs [39]. Numerous in vitro studies have demonstrated that hyaluronic acid accelerates blood clot formation, promotes angiogenesis, and stimulates the osteogenesis process [40,41,42,43,44].
Hyaluronic acid plays a fundamental role in every phase of tissue healing by stimulating the proliferation of cells, as well as their differentiation and migration [39].
The application of natural and cross-linked high molecular weight hyaluronic acid gels during subgingival instrumentation has been considered a favorable option in periodontal therapy [36]. Some authors have reported that they promote better sealing of the supporting tissues surrounding the teeth, exert a bacteriostatic effect on bacterial strains associated with periodontitis, and are beneficial in reducing bacterial contamination [39,45].
To improve the outcomes of NSPT, adjunctive periodontal treatment has recently been proposed, combining the use of sodium hypochlorite/amino acids (Perisolv, Regedent; Zürich, Switzerland) and xHyA (high-molecular) gels (Hyadent BG, Regedent) with subgingival instrumentation [32,46,47,48,49,50].
1.3. Objective
The objective of this systematic review was to analyse the scientific literature on the clinical outcomes obtained after the subgingival application of sodium hypochlorite and hyaluronic acid in conjunction with non-surgical periodontal therapy.
2. Materials and Methods
2.1. Research Conduct
This systematic review was conducted between March 2025 and May 2026 by two independent investigators who selected and analyzed articles in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [51] using the MEDLINE (via PubMed), Cochrane Library, Web of Science, and Scopus databases.
The research search strategy used was as follows: ((((((((periodontal disease[MeSH Terms]) OR (gingivitis[MeSH Terms])) OR (periodontitis[MeSH Terms])) OR (peri-implantitis[MeSH Terms])) AND (periodontal therapy[MeSH Terms])) OR (non-surgical therapy[MeSH Terms])) AND (acid hyaluronic[MeSH Terms])) OR (cross-linked hyaluronic acid[MeSH Terms])) AND (sodium hypochlorite[MeSH Terms]). In Scopus, the search was limited to research articles and studies within the fields of medicine and dentistry. The references of eligible articles were also manually searched.
The articles were analyzed by title, abstract, and full text. The studies included in this review met all the predefined criteria according to the PICOS strategy (“Population”, “Intervention”, “Comparison”, “Outcomes”, and “Study Design”).
A detailed search flowchart is presented in the Section 3.
The study protocol for this systematic review was registered on the International Prospective of Systematic Reviews (PROSPERO), under number CRD420251074045.
2.2. Study Selection
The eligibility criteria were organized using the Population, Intervention, Comparison, Outcome, and Study Design (PICOS) method, as follows in Table 1.
2.3. Inclusion Criteria
The inclusion criteria corresponding to the PICO questions were articles written in the English language; articles with no year restriction; human studies; randomized clinical trials (parallel or split-mouth design), with a follow-up period of at least 6 months; studies reporting on the application of sodium hypochlorite/amino acid and xHyA acid gels as adjunctives to non-surgical periodontal therapy; and studies reporting on BOP, PPD, CAL, or RBL as outcomes.
2.4. Exclusion Criteria
The exclusion criteria were articles without an available abstract, literature reviews, systematic reviews, meta-analyses, case series, unavailable articles, expert opinions, letters to editors, conference abstracts, animal studies, and studies examining combinations with biomaterials (e.g., bone substitutes or membranes) or growth factors (Appendix A).
2.5. Screening Method
Screening was performed by two independent examiners (T.I.d.C./F.A.), in accordance with the inclusion and exclusion criteria defined above, and a third reviewer (H.R.-V.) resolved disagreements to ensure intra- and inter-examiner reliability. The Kappa coefficient test applied in this study resulted in almost perfect agreement (0.81–0.99).
The process began with the removal of duplicate articles. Titles and abstracts were initially assessed for relevance, followed by an extensive full-text evaluation to ascertain whether the studies sufficiently addressed the research question. The PRISMA 2020 flow diagram is exhibited in Figure 1.
2.6. Extraction of Sample Data and Outcomes
The primary outcome was the probing pocket depth (PPD), measured in millimeters from the gingival margin to the bottom of the probed pocket.
The secondary outcomes were the values of variables associated with periodontitis, such as CAL, BOP, GR, PI, FMPI, and FMBOP.
The data were extracted by one reviewer (T.I.C) and summarized in a results table. The information was collected taking into consideration the author, study design and objective, eligibility criteria, study population (sample size and average age group), duration of the study and follow-up period in months, outcome measurement, and results.
2.7. Study Quality, Characteristics, and Risk of Bias
To assess the studies’ methodological quality and determine the extent to which they addressed the possibility of bias in their design, conduct, or analysis, two researchers (T.I.C./H.V.) assessed the sample according to the criteria of RoB 2 (randomized clinical trials) tools, which follow the recommendations of the Cochrane Handbook for Systematic Reviews.
3. Results
In total, 54 articles were initially identified. After excluding 16 duplicate articles, 38 studies were screened, culminating in 2 articles fulfilling the selection criteria, which were read in full and included in the qualitative synthesis. The Kappa coefficient test applied in this study resulted in almost perfect agreement (0.81–0.99).
3.1. Studies Characteristics
The two articles included were randomized clinical trials (RCTs), for which their characteristics are displayed in Table 2. Both studies, published between 2023 [48] and 2024 [50], compared the clinical outcomes of subgingival instrumentation alone and subgingival instrumentation adjunctively used sodium hypochlorite/amino acid and xHyA gels combined together. The follow-up time ranged between 6 [48] and 9 months [50].
The sample sizes were comparable across studies, comprising a total of 98 patients, ranging from 48 [48] to 50 patients [50]; the minimum mean age was 29, and the maximum age was 82.
This systematic review included the assessment of 5344 sites—1448 sites evaluated in the 2024 study by Benyei et al. and 3896 sites evaluated in the 2023 study by Ramanauskaite et al., which required further periodontal treatment [48,50].
3.2. Adjuvant Characteristics
This review included two articles [48,50] describing the adjunctive use of a sodium hypochlorite/amino acid gel (Perisolv^®^, Regedent AG, Zürich, Switzerland) administered into the pockets before subgingival instrumentation and repeatedly applied during the procedure.
Subsequently, a mixture of natural and xHyA (high molecular) gel (Hyadent^®^ BG, Regedent AG, Zürich, Switzerland) was delivered inside the pockets up to the gingival margin.
3.3. Output Measurement Methods and Results (Table 3)
3.3.1. Pocket Probing Depth (PPD)
Pocket probing depth (PPD) was reported in both studies [48,50]. In the 2024 study by Benyei et al., the PPD means did not significantly differ between the control and test groups at baseline (T1: 4.69 mm, SD = 1.01 mm vs. 4.74 mm, SD = 0.99 mm) [50]. Furthermore, in the 2023 study by Ramanauskaite et al., no significant differences were observed at baseline between the control and test groups in terms of the mean moderate pockets (4–6 mm; T0: 4.8 mm, SD = 0.2 mm and 4.7 mm, SD = 0.2 mm, respectively; p = 0.417) and in mean deep pockets (≥7 mm; T0: 8.0 mm, SD = 0.7 mm and 8.2 mm, SD = 0.9 mm, respectively; p = 0.443) [48].
As the study progressed, Benyei et al. observed a notable and significant reduction in PPD in both groups (T2: 3.35 mm, SD = 1.08 mm in control group and 3,50 mm, SD = 1.03 mm in test group; T3: 3.14 mm, SD = 1.08 mm and 2.94 mm, SD = 0.82 mm, respectively). Furthermore, the test group showed a considerably greater reduction than the control group at both the 3- and 9-month follow-ups, with that at the latter being statistically significant [50]. Ramanauskaite et al. reported statistically significant improvements in mean moderate pockets and mean deep pockets in both groups at 3 and 6 months compared to baseline (p < 0.001); however, statistically significantly higher reductions in PPD were observed at both follow-ups, favoring the test group (p < 0.001). The change in PPD between 3 and 6 months significantly differed between the groups, favoring the test group (p = 0.002) in mean moderate pockets; however, it did not differ between the groups (p = 0.096) in mean deep pockets [48].
3.3.2. Clinical Attachment Level (CAL)
Benyei et al. assessed clinical attachment levels (CALs) and reported no significant differences in the mean values between the groups at baseline (T1: 6.07 mm, SD = 1.59 mm for the control group and 5.85 mm, SD = 1.42 mm for the test group, p = 0.105) [50]. However, Ramanauskaite et al. reported that the CAL values at baseline were marginally higher in the control group (4.8 mm, SD = 0.3 mm) than in the test group (4.6 mm, SD = 0.2 mm; p = 0.026) in mean moderate pockets but were not statistically significantly different (7.9 mm, SD = 0.6 mm in the control group and 8.1 mm, SD = 0.7 mm in the test group; p = 0.412) in mean deep pockets [48].
Nevertheless, as the intervention continued, the study by Benyei et al. found that Group A (the test group) exhibited a superior improvement in CAL compared to Group B (the control group) at both the 3- and 9-month follow-ups (T2: 3.35 mm, SD = 1.08 mm in control group and 3.50 mm, SD = 1.03 mm in the test group; T3: 3.14 mm, SD = 1.01 mm and 2.94 mm, SD = 0.82 mm, respectively), with statistically significant differences (p = 0.001) [50]. In addition, Ramanauskaite et al. found statistically significant improvements in both groups at both follow-ups compared to baseline (p < 0.001); however, statistically significantly higher values were observed in the test group (p < 0.001), even though the mean CAL change between the 3- and 6-month follow-ups did not significantly differ between the groups (p = 0.077) [48].
3.3.3. Bleeding on Probing (BOP)
Benyei et al. found that bleeding on probing (BOP) did not significantly differ between the groups at any follow-up (T1—baseline; T2—3 months; T3—9 months), with p-values of 0.796, 0.175, and 0.339, respectively [50].
Ramanauskaite et al. evaluated the BOP values of treated sites (PPD ≥ 4 mm), revealing no statistically significant difference in baseline values between the control and test groups (p = 0.687). However, both groups demonstrated statistically significant improvements at the 3- and 6-month follow-ups in comparison to baseline (p < 0.001). Additionally, the BOP reduction was significantly greater in the test group than in the control group at both the 3- and 6-month follow-ups (p = 0.0018 and p < 0.001, respectively) [48].
3.3.4. Approximal Plaque Index (API)/Plaque Index (PI)
Benyei et al. presented a graphic illustrating that the development of the approximal plaque index (API) reduced throughout the follow-up periods (T1—baseline; T2—3 months; T3—9 months) [50].
Moreover, Ramanauskaite et al. found that, at baseline, the plaque index (PI) values of treated pockets (PPD > 4 mm) were higher in the test group than in the control group (T0: 60.6%, SD = 10.9% and 38.8%, SD = 26%, respectively, p = 0.002). In addition, both study groups showed statistically significant improvements at 3 months (T2: 18.8%, SD = 11.4% in the test group and 20.3%, SD = 16.7% in the control group, p = 0.714) and at 6 months (T3: 12.7%, SD = 8.9% in the test group and 26.5%, SD = 20.5% in the control group, p = 0.018) compared to baseline (p < 0.001). No statistically significant difference was observed between the groups at the 3-month follow-up (p = 0.714); however, at the 6-month follow-up, the PI reduction was significantly greater in the test group (p = 0.018) [48].
3.3.5. Gingival Recession (GR)/Recession (REC)
Benyei et al. found that the gingival recession (GR) values significantly differed between the groups at baseline (1.38 mm, SD = 1.14 mm in the control group and 1.12 mm, SD = 0.95 mm in the test group, p < 0.001). Furthermore, GR showed greater recovery in the test group, which exhibited slight positive changes (T2: 0.95 mm, SD = 0.88 mm; T3: 0.81 mm, SD = 0.82 mm), than in the control group, which showed little progression from baseline to the 3- and 9-month follow-ups (T2: 1.51 mm, SD = 1.15 mm; T3: 1.48 mm, SD = 1.15 mm) [50].
Ramanauskaite et al. took the distance (in millimeters) from the gingival margin to the cemento-enamel junction or to the margin of a cervical restoration as a measurement of recession (REC); however, they only presented clinical attachment level (CAL) values, which were calculated by adding the probing depth (PPD) and recession (REC) at each site [48].
3.3.6. Full Mouth Plaque Index (FMPI)
Ramanauskaite et al. found that the FMPI values were higher in the test group (52.9%, SD = 11.4%) than in the control group (35.7%, SD = 23.7%). Both groups showed significant improvements at the 3- and 6-month follow-ups compared to baseline (p < 0.001); however, there was a statistically significant difference between the groups, in favor of the test group at 6 months (p = 0.006) [48].
3.3.7. Full Mouth Bleeding on Probing (FMBOP)
Ramanauskaite et al. found that, at baseline, the FMBOP values were similar between the test group (76.5%, SD = 18.2%) and the control group (68.9%, SD = 20.3%): p = 0.184. Both study groups exhibited significant improvements at both 3 months (33.3%, SD = 13.7% in the control group and 25.9%, SD = 12.3% in the test group, p = 0.06) and 6 months (40.8%, SD = 13.8% in the control group and 15.6%, SD = 9.9% in the test group, p < 0.001). The difference between the groups at 3 months was not statistically significant; however, there was a statistically significant difference at the 6-month follow-up, in favor of the test group (p < 0.001) [48].
3.4. Risk of Bias Assessment
The risk of bias (Table 4) was assessed using the ROB2 tool for two RCTs, which were concealed as “Low risk” [48,50]. After re-evaluating the studies, we found that the results remained clear and did not raise any significant issues. Nonetheless, only one domain (D4) related to outcome measurement was rated as “Some concerns” due to the fact that outcome assessors were likely to be aware of the status of the intervention and were not blinded; however, the outcomes were not influenced by knowledge of the intervention received [50].
Therefore, both studies classified as “Low risk” overall reinforced the investigation value.
4. Discussion
The aim of this systematic review was to investigate the scientific literature and the current evidence regarding the clinical outcomes obtained with the subgingival application of sodium hypochlorite and hyaluronic acid in conjunction with non-surgical periodontal therapy. The fact that only two RCTs could be included in our review indicates that that there is scarce clinical evidence available in the scientific literature. Based on our findings, it is determined that adjunctive subgingival application of sodium hypochlorite/amino acids and xHyA can enhance the clinical outcomes of non-surgical periodontal therapy, as demonstrated by improvements in PPD, CAL, and BOP values [48,50].
Periodontitis is a chronic multifactorial inflammatory disease of microbial etiology that results from a dysbiotic shift in the subgingival biofilm and a subsequent destructive host immune–inflammatory response. This interplay between pathogenic microbial communities and the host’s immune mechanisms leads to the progressive loss of the tooth-supporting apparatus, clinically characterized by the formation of periodontal pockets, attachment loss, and radiographic alveolar bone resorption. The disease is modulated by genetic, systemic, and environmental factors—such as smoking, diabetes, and immune dysregulation—that influence both microbial composition and host susceptibility. Several Gram-negative anaerobic bacterial strains have been identified in the biofilms associated with periodontitis. Their roles in the dysbiosis associated with periodontitis have been extensively studied. Some of the most studied bacterial strains are A. actinomycetemcomitans, P. intermedia, P. gingivalis, T. forsythia, T. denticola, and F. nucleatum [52,53,54,55].
For instance, preclinical studies have shown that sodium hypochlorite/amino acid gel effectively disrupts the biofilm matrix and exhibits potent antiseptic activity, particularly against Gram-negative bacterial species associated with periodontitis [36,37,48,50]. Moreover, clinical studies have indicated that the adjunctive use of sodium hypochlorite/amino acid gel provides significant therapeutic benefits in the management of deep periodontal pockets in untreated periodontitis, as well as in residual periodontal pockets, peri-implant mucositis, and peri-implantitis [38,46,47,56,57,58].
Furthermore, hyaluronic acid has been shown to be efficient in reducing the proliferation of bacteria on surgical wounds and to exhibit antibacterial effects on bacterial strains linked to periodontitis [45,49]. In addition to being considered biocompatible with periodontal tissues, preclinical studies on xHyA have indicated that this formulation improves the migration, proliferative, and wound-healing capabilities of the cells essential for soft tissue wound healing [47,59]. Moreover, xHyA can sustain the stemness of osteoprogenitors while strongly promoting their growth, which could potentially stabilize the ratio between differentiation and self-renewal during bone regeneration [47,60].
As demonstrated in the studies by Ramanauskaite et al. and Benyei et al., both mechanical debridement alone and subgingival debridement in combination with xHyA and sodium hypochlorite/amino acids significantly altered microbial activity; however, distinct differences were observed between the test and control groups [47,50]. Both groups displayed statistically significant reductions in T. forsythia, T. denticola, P. gingivalis, and P. intermedia at 3 months compared to baseline (p < 0.05); nonetheless, the adjunctive group displayed a statistically significant decrease in P. intermedia and P. gingivalis (p < 0.05). However, it is important to emphasize that a statistically significant reduction in A. actinomycetemcomitans was only observed in the test group (p = 0.001) at 3 months. At 6 months, the detection frequency of T. forsythia and P. gingivalis statistically significantly decreased in the control group (p < 0.01) compared to baseline. However, in the test group, statistically significant reductions were observed for all examined periopathogenic species compared with baseline (p < 0.05) [47].
Beyond that, a series of investigations have pointed out that statistically significant decreases in P. gingivalis, T. forsythia, and T. denticola may be a hallmark of effective periodontal therapy [61].
Recent research investigations have demonstrated that sodium hypochlorite/amino acids and xHyA gels can be used adjunctively to treat deep persistent pockets non-surgically while improving clinical parameters efficiently. This allows for the delay or even circumvention of invasive surgical intervention [32,48,49,50,62].
Sodium hypochlorite/amino acid (A2H) gel makes it easier to distinguish between healthy and granulated tissues, decreases the bacterial population by dissolving the biofilm matrix, restricts tissue recession by improving clinical attachment levels (CALs) and decreasing pocket probing depth (PPDs), helps to decontaminate the periodontal sites, and successfully treats the biofilm, as well as being harmless to the tissues and tooth surface when used at a 0.5% concentration [32,47,48,49,50,57,63,64].
Cross-linked hyaluronic acid (high-molecular) gel promotes soft tissue and bone regeneration, accelerates pocket closure by maintaining blood clots, presents bacteriostatic characteristics that promote healing and maintain wound decontamination, and fosters periodontium cell adherence and regeneration, thereby reducing pocket probing depths (PPDs) and improving clinical attachment levels (CALs) [32,46,47,48,49,59,60,61,62,63,64,65,66,67,68,69].
According to the results obtained, adjunctive non-surgical periodontal treatment with sodium hypochlorite/amino acids and xHyA (high molecular) gels has advantages over SRP alone. Ramanauskaite et al. conducted a 6-month study and investigated PPD as the primary outcome. They found that both adjunctive treatment and SRP alone provided statistically significant improvements in every clinical parameter evaluated; however, the combination of sodium hypochlorite/amino acids and xHyA gels with subgingival mechanical debridement yielded statistically significantly better improvements than SRP alone, thereby providing a useful strategy to enhance the clinical outcomes of non-surgical periodontal therapy, such as PPD, CAL, and BOP [48]. Benyei et al. conducted a 9-month study and investigated CAL as the primary outcome. They found that the adjunctive combination of sodium hypochlorite/amino acids and xHyA gels with subgingival mechanical debridement sufficiently improved clinical outcomes, namely, PPD, CAL, and BOP. Furthermore, at the 9-month follow-up, they also found that adjunctive treatment might indicate a propensity for a regenerative response to treatment [50].
Interestingly, both studies reported high efficacy of the adjunctive treatment related to deep pockets. Ramanauskaite et al. found that the number of deep pockets reduced from 277 to 35 in the control group; however, much better results were found in the test group, where the number reduced from 298 to 4 (p = 0.003) [48]. These findings are also consistent with those of the study conducted by Benyei et al., who reported a deep pocket closure rate of 94% in the test group, highly contrasting with the rate of 42% in the control group [50].
Another study conducted by Ramanauskaite et al., which included twenty-one systemically healthy patients diagnosed with stage II-III grade A/B periodontitis, also reported that the use of sodium hypochlorite/amino acids and xHyA gels adjunctive to subgingival mechanical debridement may constitute an advantageous method for enhancing the clinical outcomes of NSPT. At 3- and 6-month follow-ups, statistically significant mean reductions in PPD were observed compared to baseline (p < 0.001), and the difference between the 3- and 6-month follow-ups was also statistically significant (p = 0.004). Furthermore, the mean CAL enhancement was statistically significant at both the 3- and 6-month follow-ups compared to baseline (p < 0.001), and a statistically significant difference in CAL gain was also found between the 3- and 6-month follow-ups (p = 0.016). A notable and significant difference was found in this study, with a reduction in the number of deep pockets from 319 to 3 [49], which is consistent with the results of Ramanauskaite et al. and Benyei et al. [48,50].
In line with our study, in 2022, Diehl et al. performed a 6-month study in 29 patients with 111 sites receiving treatment. Bleeding on probing decreased by more than 60%, and an overall PPD reduction exceeding 2 mm was achieved, alongside a comparable CAL gain of 2.02 mm. Pocket closure was observed in nearly 25% of sites. Furthermore, they also reported that sodium hypochlorite cleaning–gel application may provide additional benefits to NSPT by enhancing mechanical biofilm removal, thereby amplifying the impact of xHyA. This study concluded that the adjunctive application of sodium hypochlorite and hyaluronic acid gels in NSPT is extremely advantageous [32], a conclusion identical to that of the previously mentioned studies [47,48,49,50].
Another clinical investigation conducted in 2024 by Shirakata et al. [70] compared the histological aspects of NSPT both with and without the adjunctive use of sodium hypochlorite/amino acids and xHyA gels in dogs. The clinical outcomes of this animal study are consistent with those of clinical investigations that concluded that the use of SRP with sodium hypochlorite/amino acids and xHyA gels produced statistically significant enhancements in clinical outcomes, reflected in a decline in BOP values, improvements in CALs, and reductions in PPDs, when compared to baseline or SRP alone [70], which is also in accordance with our study [32,47,48,49,50]. Consistent with the clinical findings, the histological evaluation provided noteworthy evidence supporting these outcomes. The test group showed statistically significantly greater amounts of new connective attachment, new cementum formation, and new bone formation than the control group [70].
To date, only positive results have been obtained regarding the adjunctive use of sodium hypochlorite/amino acids and xHyA (high molecular) gels in non-surgical periodontal therapy (NSPT).
5. Conclusions
The adjunctive use of sodium hypochlorite/amino acids and xHyA (high-molecular) gels in non-surgical periodontal therapy (NSPT) significantly enhances clinical outcomes compared to the use of subgingival instrumentation alone. Adjunctive periodontal therapy appears to contribute to a regenerative healing response. Despite these promising results, the limited number of studies highlights the need for further multicenter, long-term randomized controlled trials with longer follow-up periods and larger sample sizes in order to corroborate these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Belibasakis G.N. Belstrøm D. Eick S. Gursoy U.K. Johansson A. Könönen E. Periodontal microbiology and microbial etiology of periodontal diseases: Historical concepts and contemporary perspectives Periodontol. 2000202311710.1111/prd.1247336661184 · doi ↗ · pubmed ↗
- 2Borisy G.G. Valm A.M. Spatial scale in analysis of the dental plaque microbiome Periodontol. 20002021869711210.1111/prd.1236433690940 PMC 8972407 · doi ↗ · pubmed ↗
- 3Sedghi L. Di Massa V. Harrington A. Lynch S.V. Kapila Y.L. The oral microbiome: Role of key organisms and complex networks in oral health and disease Periodontol. 200020218710713110.1111/prd.1239334463991 PMC 8457218 · doi ↗ · pubmed ↗
- 4Papapanou P.N. Sanz M. Buduneli N. Dietrich T. Feres M. Fine D.H. Flemmig T.F. Garcia R. Giannobile W.V. Graziani F. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions J. Periodontol.201889 S 173S 18210.1002/JPER.17-072129926951 · doi ↗ · pubmed ↗
- 5Pihlstrom B.L. Michalowicz B.S. Johnson N.W. Periodontal diseases Lancet 20053661809182010.1016/S 0140-6736(05)67728-816298220 · doi ↗ · pubmed ↗
- 6Papapanou P.N. The Prevalence of Periodontitis in the USJ. Dent. Res.20129190790810.1177/002203451245869222935674 · doi ↗ · pubmed ↗
- 7Kassebaum N.J. Smith A.G.C. BernabéE. Fleming T.D. Reynolds A.E. Vos T. Murray C.J.L. Marcenes W. GBD 2015 Oral Health Collaborators Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors J Dent. Res.20179638038710.1177/002203451769356628792274 PMC 5912207 · doi ↗ · pubmed ↗
- 8Chung S.Y. Song K.B. Lee S.G. Choi Y.H. The strength of age effect on tooth loss and periodontal condition in Korean elderly Arch. Gerontol. Geriatr.201153 e 243e 24810.1016/j.archger.2011.04.02121641050 · doi ↗ · pubmed ↗