Influence of Pharmacological Agents on Orthodontic Tooth Movement: A Systematic Review
Lucia Giannini, Federica Macrì, Angelo Michele Inchingolo, Francesco Inchingolo, Gianna Dipalma, Cinzia Maspero

TL;DR
This systematic review explores how medications affect orthodontic tooth movement, pain, and periodontal outcomes, emphasizing the need for clinical trials.
Contribution
The study systematically reviews the clinical and biological effects of pharmacological agents on orthodontic outcomes.
Findings
NSAIDs reduce orthodontic pain but may slow tooth movement in a dose-dependent manner.
Antiresorptive drugs like bisphosphonates are linked to reduced tooth movement.
Topical antimicrobials and probiotics improve periodontal outcomes without affecting tooth movement.
Abstract
Background: Pharmacological agents may interfere with the biological processes underlying orthodontic tooth movement (OTM), potentially affecting treatment duration, pain control, and periodontal outcomes. Methods: A systematic review was conducted according to PRISMA 2020 guidelines and registered in PROSPERO. Human studies were prioritized to assess clinically relevant effects on OTM and pain, while animal and in vitro studies were included to support biological interpretation. Results: Sixty-four studies were included. Human evidence indicates that NSAIDs effectively reduce orthodontic pain but may decrease the rate of tooth movement in a dose-dependent manner. Antiresorptive drugs, particularly bisphosphonates, were consistently associated with reduced OTM. Topical antimicrobials, fluoride agents, and probiotics improved periodontal and enamel outcomes without significantly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
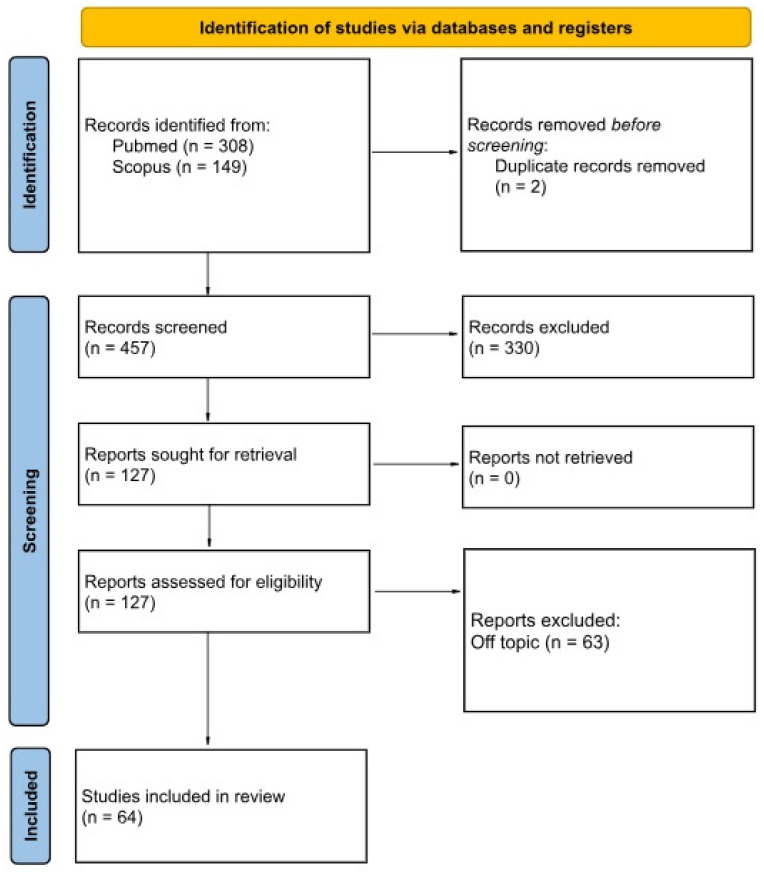 Figure 1
Figure 1- —Italian Ministry of Health—Current research IRCCS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Dental Anxiety and Anesthesia Techniques · Temporomandibular Joint Disorders
1. Introduction
Orthodontic tooth movement (OTM) is a biologically driven process resulting from the application of controlled mechanical forces to teeth, leading to coordinated inflammatory responses and alveolar bone remodeling [1,2,3,4]. These events involve the activation of periodontal ligament cells, the release of cytokines and prostaglandins, and the regulation of osteoclastic and osteoblastic activity. As a result, any factor capable of modulating inflammation or bone metabolism has the potential to influence the rate and pattern of tooth movement [5,6,7,8].
In contemporary orthodontic practice, an increasing number of patients—both adolescents and adults—are exposed to systemic or local pharmacological agents for acute or chronic conditions. Analgesics, anti-inflammatory drugs, bone metabolism–modifying agents, hormones, and immunomodulatory therapies are frequently prescribed and may interfere with the biological mechanisms underlying OTM. From a clinical perspective, such interactions may affect treatment duration, anchorage control, pain management, and the risk of adverse effects such as root resorption or periodontal alterations [9,10,11,12].
Experimental and clinical studies have reported heterogeneous and sometimes conflicting effects of pharmacological agents on OTM. Non-steroidal anti-inflammatory drugs (NSAIDs) have been shown to reduce orthodontic pain but may slow tooth movement by inhibiting prostaglandin-mediated bone resorption. Conversely, agents influencing bone turnover, such as parathyroid hormone or vitamin D, have been associated with accelerated movement in preclinical models. However, much of the available evidence derives from animal or in vitro studies, and the translational relevance to human orthodontic treatment remains uncertain [13,14,15,16,17,18].
Previous reviews have addressed selected drug classes or specific outcomes, but a focused synthesis integrating clinically relevant outcomes with underlying biological mechanisms is still lacking. Importantly, the wide variability in study design, experimental models, and outcome measures has contributed to fragmented knowledge and limited clinical applicability.
Therefore, the aim of this systematic review is to address the following focused question: how do pharmacological agents influence orthodontic tooth movement and its underlying biological mechanisms?
Human studies were prioritized to assess clinical outcomes such as tooth movement rate, pain, and treatment-related effects, while animal and in vitro studies were included to elucidate mechanistic pathways supporting or explaining clinical observations. By adopting a translational framework, this review seeks to provide a critical and clinically oriented synthesis of the evidence, while clearly acknowledging its methodological limitations.
2. Materials and Methods
2.1. Protocol
This systematic review was conducted in accordance with the PRISMA 2020 and PRISMA-P guidelines for transparent reporting of systematic reviews.
The protocol of this systematic review was prospectively registered in PROSPERO [CRD420251242400].
2.2. Review Objectives and Hypotheses
The primary objective of this review was to critically evaluate the effects of pharmacological agents on orthodontic treatment. Specifically, the review investigated how different drugs influence.
The analysis focused on how different drugs influence:
- -Orthodontic tooth movement;
- -Bone remodeling and inflammatory markers;
- -Periodontal and pulpal responses;
- -Pain modulation during orthodontic treatment;
- -Enamel demineralization;
- -Clinical implications for orthodontic mechanics and treatment planning in growing patients and adults.
Underlying hypotheses were that:
- -NSAIDs and other anti-inflammatory drugs reduce OTM by suppressing prostaglandin-mediated bone resorption.
- -Bone metabolism-modifying agents can impact the rate and pattern of tooth movement.
- -Hormonal agents and immunomodulatory drugs alter periodontal tissue responses.
- -Topical agents influence enamel stability during fixed appliance therapy.
2.3. PICO
-
Population (P): Patients undergoing orthodontic treatment; animal and in vitro models were included to support biological interpretation.
-
Intervention (I): Systemic or local pharmacological agents administered during orthodontic treatment.
-
Comparison (C): No pharmacological exposure, placebo, or alternative drug when applicable.
-
Outcomes (O):
-
Primary outcome: Rate or extent of orthodontic tooth movement.
-
Secondary outcomes: Pain perception during orthodontic treatment and periodontal or enamel responses directly related to appliance therapy.
Mechanistic outcomes derived from animal or in vitro studies (e.g., inflammatory mediators and bone remodeling markers) were considered supportive and hypothesis-generating.
2.4. Search Strategy and Study Selection
A systematic search was conducted in PubMed-MEDLINE and Scopus databases. A manual search of reference lists of included articles and relevant reviews was performed. Grey literature was searched through OpenGrey and Google Scholar and reference lists of included studies and relevant reviews were manually searched.
The search included studies published between January 2000 and December 2025, in English.
A structured search strategy using MeSH terms and free-text keywords was applied.
** PubMed search: **
[[“orthodontic tooth movement”[tiab] OR “orthodontic movement”[tiab] OR “tooth movement”[tiab] OR orthodontic[tiab]] AND [“Pharmaceutical Preparations”[MeSH] OR “Drug Therapy”[MeSH] OR drug*[tiab] OR medication*[tiab] OR pharmacolog*[tiab] OR medicine*[tiab] OR analgesic*[tiab] OR “anti-inflammatory”[tiab] OR corticosteroid*[tiab] OR bisphosphonate*[tiab] OR hormone*[tiab] OR prostaglandin*[tiab] OR “Anti-Inflammatory Agents, Non-Steroidal”[MeSH] OR “Bone Remodeling”[MeSH]] AND [“bone remodeling”[tiab] OR “bone resorption”[tiab] OR “orthodontic force”[tiab] OR “tooth movement”[tiab]] AND Humans[MeSH Terms] AND English[lang] NOT [review[Publication Type] OR case reports[Publication Type]] AND [“1 January 2000“[Date-Publication]: “31 December 2025”[Date-Publication]]*
** Scopus search: **
TITLE-ABS-KEY [“orthodontic tooth movement” OR “orthodontic treatment” OR “tooth movement” OR “orthodontic therapy”] AND [“drug therapy” OR drug OR medication OR NSAID OR bisphosphonate OR corticosteroid OR antibiotic OR statin OR metformin OR hormone OR analgesic OR chlorhexidine] AND [“effect” OR “influence” OR “impact” OR “interaction” OR “response” OR “tooth movement rate” OR “anchorage loss” OR “bone remodeling” OR “bone resorption”] AND [child OR children OR pediatric OR paediatric OR adolescent OR “growing patient”] AND NOT [“implant” OR “cleft” OR “craniofacial” OR “surgery”] AND PUBYEAR > 1999 AND PUBYEAR < 2026 AND [LIMIT-TO [DOCTYPE, “ar”] AND [LIMIT-TO [LANGUAGE, “English”]
The last search was performed on 20 October 2025.
2.5. Study Selection
The study selection process was conducted independently by two reviewers. Any discrepancies in the screening or eligibility assessment were resolved through discussion and consensus.
All retrieved citations from PubMed-MEDLINE, Scopus, and grey literature were imported into Microsoft Excel, and duplicate records were removed prior to screening.
The screening process was conducted in two sequential phases: initial screening of titles and abstracts, followed by full-text assessment for eligibility.
A PRISMA flow diagram illustrates the selection process.
2.6. Inclusion and Exclusion Criteria
Inclusion criteria:
- -Randomized controlled trials [RCTs], controlled clinical trials, observational studies, in vitro studies, and preclinical animal studies;
- -Studies evaluating the effects of drugs on tooth movement, bone remodelling, periodontal response, or pain modulation during orthodontic treatment;
- -Published between 2000 and 2025;
- -Full text available in English.
Exclusion criteria:
- -Studies not relevant to the review objective;
- -Studies on dental topics unrelated to orthodontics;
- -Case reports, letters, or abstracts;
- -Non-English articles without full text
Studies focused exclusively on surgical orthodontics or craniofacial anomalies
2.7. Data Extraction and Organization
Data extraction was conducted independently by two reviewers using a standardized and piloted extraction sheet.
For each included study, the following data were collected:
- -Authors and year of publication;
- -Study design;
- -Population or experimental model;
- -Drug studied;
- -Orthodontic intervention or biological outcome;
- -Main results;
- -Clinical relevance of drug effects.
To facilitate interpretation, studies were organized by drug categories:
- 1NSAIDs and analgesics;
- 2Drugs affecting bone metabolism [bisphosphonates, RANK/RANKL modulators, vitamin D, etc.];
- 3Hormones and endocrine agents;
- 4Antiseptics and antimicrobials;
- 5Special systemic or immunomodulatory drugs;
- 6Other drugs with potential orthodontic impact.
Given the overlap in clinical purpose and outcomes, antiseptics, antimicrobials, probiotics, and preventive topical agents were analyzed within a single category focusing on periodontal and enamel protection during orthodontic treatment.
This classification allows for a clearer understanding of the specific interaction of each drug with orthodontic treatments.
2.8. Risk of Bias Assessment and GRADE
Risk of bias was independently assessed by two reviewers using validated tools according to study design:
RoB2 for randomized controlled trials;
ROBINS-I for non-randomized clinical studies;
SYRCLE’s RoB tool for animal studies;
OHAT risk-of-bias tool for in vitro studies;
Disagreements were resolved through discussion.
The certainty of evidence for each outcome category was evaluated using the GRADE approach, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias.
For each included study, the overall risk-of-bias judgement was supported by explicit methodological reasons, which are reported in the risk-of-bias tables and Supplementary Material.
2.9. Data Analysis
Due to clinical and methodological heterogeneity in drugs, experimental models, and measured outcomes, a meta-analysis was not performed. A qualitative synthesis of the studies was conducted using a tabular comparison. Where available, quantitative results such as tooth movement rates, inflammatory biomarker levels, or tissue effects were reported and compared. Descriptive statistics were used to summarize the distribution of studies by drug type and outcome.
3. Results
The electronic and manual searches identified a total of 457 records. After removal of duplicates and two-stage screening (title/abstract and full-text assessment), 64 studies met the inclusion criteria and were included in the qualitative synthesis. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
3.1. Characteristics of Included Studies
The included studies comprised a heterogeneous body of evidence, including randomized controlled trials, non-randomized clinical studies, observational studies, animal models, and in vitro experiments. Pharmacological agents investigated encompassed NSAIDs and analgesics, drugs affecting bone metabolism, hormonal and endocrine agents, antimicrobials, probiotics, and selected immunomodulatory drugs.
Given this heterogeneity, results were synthesized qualitatively and organized according to drug class and clinical relevance. Detailed characteristics of individual studies are reported in the Supplementary Materials.
PRISMA 2020 flow diagram illustrating the study identification, screening, eligibility assessment and inclusion process.
3.2. Human Clinical Evidence on Orthodontic Tooth Movement and Pain
3.2.1. NSAIDs and Analgesics
Human clinical studies consistently demonstrated that NSAIDs effectively reduce orthodontic pain, particularly during the early phases of treatment. Ibuprofen showed superior analgesic efficacy compared with acetaminophen in several randomized trials, both when administered pre-emptively and post-activation. Acetaminophen also reduced pain intensity but generally to a lesser extent [18,19,20].
Evidence from animal models suggested that NSAIDs, including ibuprofen and meloxicam, may reduce the rate of orthodontic tooth movement (OTM) through inhibition of prostaglandin-mediated osteoclastic activity. However, this inhibitory effect was primarily supported by preclinical data, while direct clinical evidence on OTM reduction in humans remains limited [21,22]. (Tables S1–S3).
Collectively, these findings indicate that NSAIDs provide effective pain control but may influence bone remodeling mechanisms involved in OTM, particularly with prolonged or high-dose administration. Summary of clinically relevant findings is reported in Table 1.
3.2.2. Drugs Affecting Bone Metabolism
Drugs modulating bone remodeling showed consistent effects on OTM, with direction dependent on their mechanism of action [23,24,25].
Antiresorptive agents, particularly bisphosphonates, were associated with reduced tooth movement in both human observational studies and animal models. Patients undergoing chronic bisphosphonate therapy demonstrated slower orthodontic movement and increased difficulty in achieving planned tooth displacement.
Conversely, intermittent parathyroid hormone (PTH) administration and prostaglandin E1 (PGE1) were associated with accelerated OTM, particularly in experimental settings or in conjunction with surgical interventions. However, human clinical evidence supporting routine clinical use of these agents remains limited [26,27,28,29,30,31,32,33].
Other agents, such as simvastatin, showed a modulatory effect by preserving anchorage without significantly altering OTM. Tables S4–S6.
A clinically oriented synthesis of these effects is provided in Table 2, while detailed mechanistic and preclinical data are reported in the Supplementary Materials.
3.2.3. Hormonal and Endocrine Agents
Hormonal status and endocrine agents were associated with variable modulation of OTM. Clinical studies suggested that sex hormones may influence inter-individual variability in tooth movement, with testosterone associated with faster OTM and estrogen exerting a modulatory effect. Tables S7–S9.
Vitamin D and vitamin E supplementation showed potential to support bone remodeling and antioxidant balance, with limited evidence suggesting a possible acceleration of OTM. In contrast, glucocorticoid therapy and nicotine exposure were associated with impaired bone metabolism and potentially slower tooth movement.
Given the predominance of observational and preclinical data, these findings should be interpreted cautiously. Detailed results are reported in the Supplementary Materials [34,35,36,37,38,39,40,41].
3.2.4. Periodontal and Enamel Outcomes in Orthodontic Patients
Topical antimicrobials and preventive agents demonstrated consistent benefits for periodontal and enamel health without significantly affecting OTM.
Chlorhexidine mouthwashes and varnishes effectively reduced plaque accumulation and bacterial load, particularly Streptococcus mutans, although prolonged use was associated with side effects such as tooth staining and taste alteration. Probiotics, fluoride formulations, MI Paste Plus, and natural dentifrices improved gingival indices and reduced enamel demineralization around orthodontic appliances. Tables S10–S12.
A summary of clinically relevant periodontal and enamel outcomes is provided in Table 3. Detailed comparisons of formulations and protocols are reported in the Supplementary Materials [42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65].
3.2.5. Special Systemic Drugs and Immunomodulators
Limited evidence suggested that certain systemic drugs, including cyclosporine, methylphenidate, and long-term corticosteroids, may adversely affect periodontal tissues, bone remodeling, or craniofacial growth, potentially complicating orthodontic treatment. Tables S13–S17.
Conversely, thymosin α1 showed beneficial effects on periodontal healing in specific clinical contexts, such as tooth reimplantation. Due to the limited number of studies and high risk of bias, these findings should be considered hypothesis-generating [66,67,68,69,70,71,72,73,74].
3.3. Risk of Bias and Certainty of Evidence
Overall, most included studies demonstrated moderate to high risk of bias, primarily due to inadequate randomization, lack of blinding, and small sample sizes. Using the GRADE approach, the certainty of evidence was rated as low to very low across most outcomes. A condensed GRADE summary is presented in Table 4 and Table 5, while detailed assessments are provided in the Supplementary Materials.
4. Discussion
This systematic review evaluated the effects of systemic and local pharmacological agents on orthodontic tooth movement and related biological and clinical outcomes. The available evidence suggests that several commonly prescribed drugs can influence orthodontic treatment primarily through modulation of inflammatory responses and bone remodeling processes [1,2,3,4,5]. However, the direction and clinical relevance of these effects vary considerably depending on drug class, dosage, duration of administration, and patient-related factors (Table 6).
One of the most consistent findings concerns the use of non-steroidal anti-inflammatory drugs (NSAIDs) during orthodontic treatment. Human clinical studies confirmed that NSAIDs are effective in reducing orthodontic pain, particularly during the early phases following appliance activation [1,2,17,18,19,20]. Ibuprofen was generally more effective than acetaminophen in pain control, especially in the first 24–48 h [2,17,18,20]. At the same time, experimental evidence indicates that NSAIDs may reduce the rate of orthodontic tooth movement by inhibiting prostaglandin-mediated osteoclastic activity [5,21,22]. Although this inhibitory effect on tooth movement has been demonstrated mainly in animal models, it raises relevant clinical considerations, particularly in patients requiring prolonged or frequent analgesic use. From a clinical perspective, careful selection of analgesics remains important to balance effective pain management with preservation of orthodontic efficiency [6,7,8].
Drugs affecting bone metabolism showed more pronounced and predictable effects on orthodontic tooth movement. Antiresorptive agents, such as bisphosphonates, were consistently associated with reduced tooth movement in both clinical and experimental studies [27,28]. In patients undergoing long-term bisphosphonate therapy, orthodontic treatment may be characterized by a potentially slower response, increased resistance to movement, and a higher risk of suboptimal outcomes [27]. Conversely, agents that stimulate bone remodeling, including intermittent parathyroid hormone and prostaglandin E1, demonstrated a potential to accelerate orthodontic tooth movement, particularly in experimental settings or in conjunction with surgical interventions [9,25,26,31,32]. Nevertheless, the limited availability of controlled clinical trials and concerns regarding adverse effects, such as root resorption, currently restrict their routine clinical application [31,32].
Hormonal and endocrine agents appeared to contribute to inter-individual variability in orthodontic response rather than exerting uniform effects. Clinical and experimental data suggest that sex hormones may modulate bone turnover and periodontal ligament response, potentially influencing the rate of tooth movement [11,40]. Similarly, vitamin D and vitamin E supplementation were associated with favorable effects on bone metabolism and oxidative stress balance, with limited evidence suggesting a possible supportive role during orthodontic treatment [34,35,36,37]. In contrast, chronic glucocorticoid therapy and nicotine exposure were generally associated with impaired bone quality and altered tissue responses, potentially complicating orthodontic mechanics and treatment duration [33,38,39]. These findings highlight the importance of considering endocrine status and lifestyle factors during treatment planning.
In contrast to systemic drugs affecting bone remodeling, topical agents and microbiome-modulating therapies primarily influenced periodontal and enamel outcomes rather than orthodontic tooth movement. Chlorhexidine-based products consistently reduced plaque accumulation and bacterial load around orthodontic appliances [42,43,44,45,46,47,48], although their prolonged use was associated with well-known side effects, including tooth staining and taste alteration [42,47]. Probiotics, fluoride-based products, remineralizing agents, and natural dentifrices demonstrated beneficial effects on gingival health and enamel demineralization without significantly affecting tooth movement [13,49,52,53,54,55,56,57,58,59,60,61,62,63,64,65]. These interventions appear to represent valuable adjuncts for maintaining oral health during fixed appliance therapy, particularly in patients at increased risk of caries or periodontal inflammation.
Special systemic drugs and immunomodulatory agents were supported by limited and heterogeneous evidence. Immunosuppressive therapies, including cyclosporine and long-term corticosteroids, were associated with increased risk of gingival overgrowth, periodontal complications, and altered craniofacial growth patterns [12,67,70]. Conversely, thymosin α1 showed beneficial effects on periodontal healing in specific clinical scenarios, such as tooth reimplantation [66]. Due to the limited number of studies and the predominance of observational or experimental designs, these findings should be interpreted cautiously and primarily serve to raise clinical awareness rather than guide definitive treatment decisions [68].
Unlike previous reviews focusing on single drug classes, this review integrates systemic, topical and microbiome-modulating agents within a translational orthodontic framework.
A relevant aspect of this review is the inclusion of animal and in vitro studies to support biological interpretation of clinical findings. While preclinical models provide valuable insights into the mechanisms underlying orthodontic tooth movement, their direct translation to clinical practice is limited by differences in force application, tissue response, and systemic conditions [72,73,74]. For this reason, preclinical evidence in the present review was considered supportive rather than determinant for clinical recommendations.
Several limitations must be acknowledged. The overall quality of the available evidence was low to very low, with many studies affected by high risk of bias, small sample sizes, and methodological heterogeneity [14,15]. The frequent reliance on animal models and surrogate biochemical markers further limits the direct applicability of findings to human orthodontic treatment. In addition, differences in drug dosage, administration protocols, and outcome measures prevented quantitative synthesis and meta-analysis.
Despite these limitations, the present review highlights the clinical relevance of pharmacological factors in orthodontic treatment. A thorough medication history should be considered an essential component of orthodontic diagnosis and treatment planning. Awareness of potential drug–orthodontic interactions may help clinicians anticipate variations in tooth movement, adjust biomechanics, and optimize patient management [16]. Future well-designed clinical studies are required to clarify drug-specific effects and to support evidence-based, personalized orthodontic care [75,76,77,78,79,80,81,82,83,84].
5. Conclusions
This systematic review highlights that pharmacological agents may influence orthodontic tooth movement primarily through modulation of inflammation and bone remodeling. Clinical evidence from human studies supports effective pain reduction with NSAIDs, although potential effects on tooth movement rate should be considered. Antiresorptive drugs are consistently associated with slower orthodontic movement, while topical preventive agents improve periodontal and enamel health without altering OTM [85,86,87,88,89].
Most mechanistic insights derive from animal and in vitro studies and should be interpreted cautiously when applied to clinical practice. Given the overall low certainty of available evidence, clinicians should individualize orthodontic treatment based on comprehensive medication history and risk assessment. Further high-quality human studies are required to clarify drug-specific effects and guide evidence-based orthodontic decision-making [90,91,92,93,94,95,96,97,98,99,100,101,102].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta M. Kandula S. Laxmikanth S.M. Vyavahare S.S. Reddy S.B.H. Ramachandra C.S. Controlling pain during orthodontic fixed appliance therapy with non-steroidal anti-inflammatory drugs (NSAID): A randomized, double-blinded, placebo-controlled study J. Orofac. Orthop.20147547147610.1007/s 00056-014-0243-725355194 · doi ↗ · pubmed ↗
- 2Shetty N. Patil A.K. Ganeshkar S.V. Hegde S. Comparison of the effects of ibuprofen and acetaminophen on PGE 2 levels in the GCF during orthodontic tooth movement: A human study Prog. Orthod.201314610.1186/2196-1042-14-624325834 PMC 3847847 · doi ↗ · pubmed ↗
- 3Maspero C. Galbiati G. Giannini L. Guenza G. Farronato M. Class II division 1 malocclusions: Comparisons between one- and two-step treatment Eur. J. Paediatr. Dent.2018429529910.23804/ejpd.2018.19.04.830567446 · doi ↗ · pubmed ↗
- 4Farronato G. Rosso G. Giannini L. Galbiati G. Maspero C. Correlation between skeletal Class II and temporomandibular joint disorders: A literature review Minerva Stomatol.20166523924726938175 · pubmed ↗
- 5Kirschneck C. Meier M. Bauer K. Proff P. Fanghänel J. Meloxicam medication reduces orthodontically induced dental root resorption and tooth movement velocity: A combined in vivo and in vitro study of dental-periodontal cells and tissue Cell Tissue Res.2017368617810.1007/s 00441-016-2553-028044198 · doi ↗ · pubmed ↗
- 6Maspero C. Galbiati G. Giannini L. Farronato G. Sagittal and vertical effects of transverse sagittal maxillary expander (TSME) in three different malocclusion groups Prog. Orthod.201516610.1186/s 40510-015-0075-z 25907431 PMC 4409608 · doi ↗ · pubmed ↗
- 7Farronato G. Giannini L. Galbiati G. Stabilini S.A. Maspero C. Orthodontic-surgical treatment: Neuromuscular evaluation in open and deep skeletal bite patients Prog. Orthod.2013144110.1186/2196-1042-14-4124325989 PMC 4394416 · doi ↗ · pubmed ↗
- 8Cenzato N. Crispino R. Galbiati G. Giannini L. Bolognesi L. Lanteri V. Maspero C. Premature loss of primary molars in children: Space recovery through molar distalisation. A literature review Eur. J. Paediatr. Dent.202425727610.23804/ejpd.2024.211038353522 · doi ↗ · pubmed ↗