Bioengineering Innovations for Personalized Care in Low Back Pain: From Sensors to Smart Therapeutics
Jiri Gallo, Michal Stefancik, Petr Mik, Lenka Lhotska

TL;DR
This paper reviews how bioengineering innovations, like sensors and smart therapeutics, can improve personalized care for low back pain by enabling continuous monitoring and adaptive rehabilitation.
Contribution
The paper introduces a framework for integrating biosensing technologies with clinical rehabilitation workflows to address individual variability in low back pain.
Findings
Multimodal biosensing can track neuromuscular and movement patterns for personalized LBP care.
Continuous monitoring allows early detection of non-response to rehabilitation, enabling timely adjustments.
Integration of biosensing with transparent analytics supports adaptive, patient-centered rehabilitation.
Abstract
Low back pain (LBP) remains one of the most prevalent and disabling musculoskeletal conditions worldwide, shaped by interacting mechanical, neurophysiological, inflammatory, vascular, and behavioral factors. Conventional care often relies on generalized exercise programs and episodic, predominantly subjective assessment, which can underrepresent inter-individual heterogeneity and longitudinal change. Recent bioengineering advances enable continuous, multimodal monitoring of objective correlates of function—neuromuscular activation and coordination (sEMG/polyEMG), movement patterns and activity exposure (IMU), and complementary physiological context (e.g., autonomic and perfusion-related signals). Rather than measuring pain directly, these signals can contextualize symptoms, support treatment stratification within non-surgical care, and enable trajectory monitoring with early…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
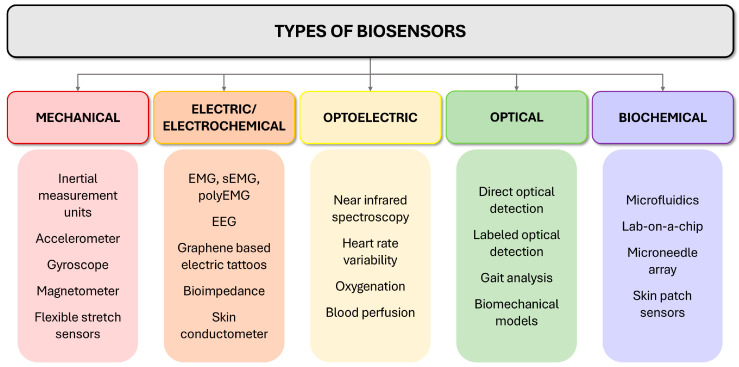 Figure 1
Figure 1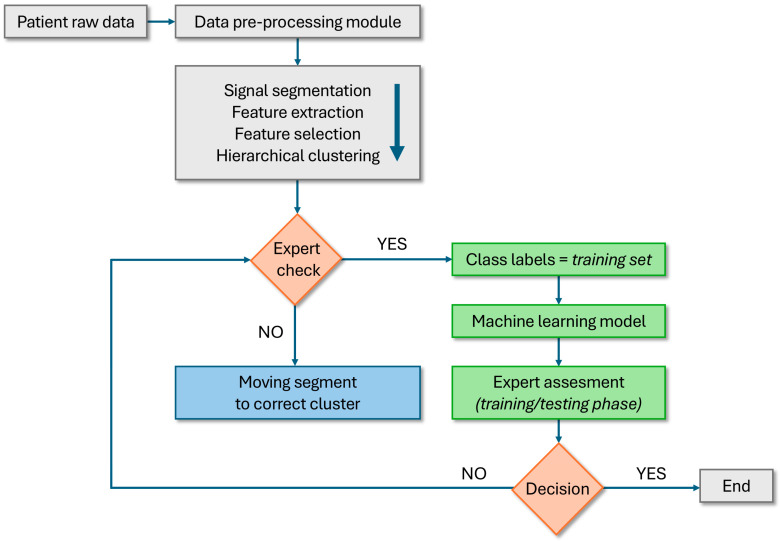 Figure 2
Figure 2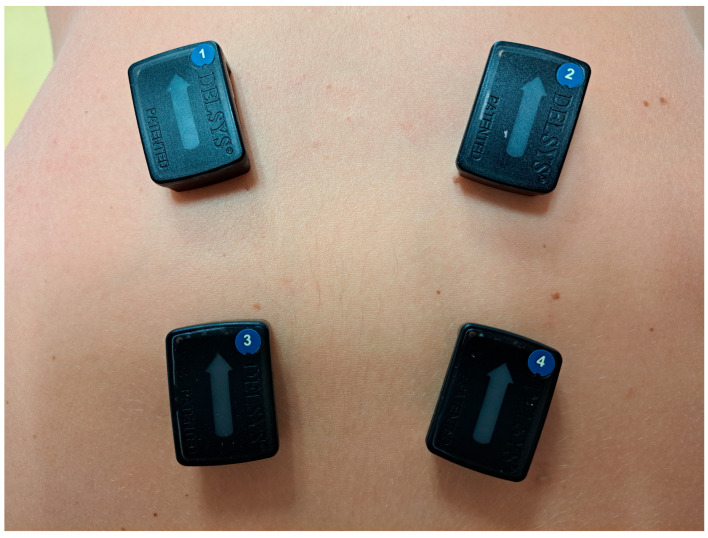 Figure 3
Figure 3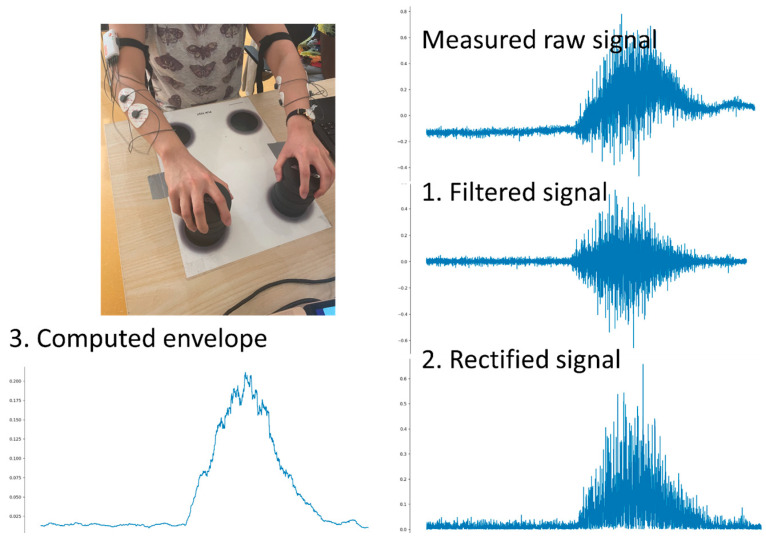 Figure 4
Figure 4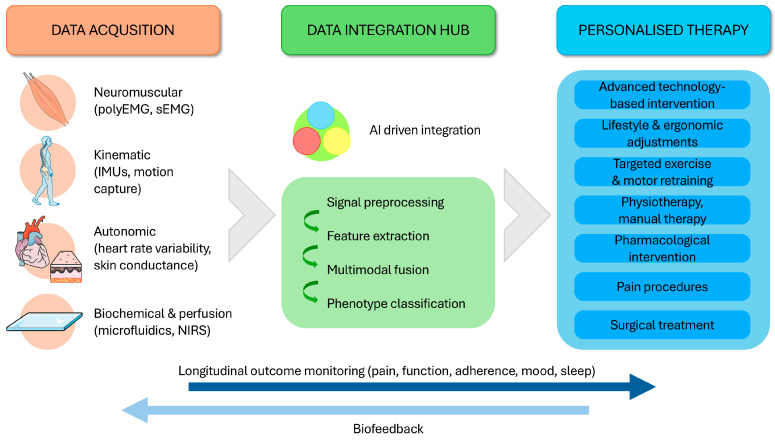 Figure 5
Figure 5- —IGA
- —Ministry of Health, Czech Republic—conceptual development of research organization
- —Center for Artificial Intelligence and Quantum Computing in System Brain Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Muscle activation and electromyography studies · Prosthetics and Rehabilitation Robotics
1. Introduction
Low back pain (LBP) is a multifactorial syndrome characterized by lumbosacral pain with variable stiffness, movement limitation, altered muscle activation, and—in some presentations—neurogenic symptoms [1]. Symptoms often fluctuate with posture and activity exposure, and LBP remains among the leading causes of disability worldwide with substantial societal and healthcare burden [2].
Clinically, LBP is often categorized as “specific” (identifiable structural, inflammatory, or neurological cause) or “non-specific,” yet this dichotomy is increasingly insufficient [3]. Many patients exhibit co-existing structural and functional abnormalities—degenerative findings, altered lumbopelvic coordination, protective co-contraction, reduced movement variability, or fatigue-related deterioration—none of which is universally causal in isolation (Table 1). The practical challenge is therefore not the absence of abnormalities, but objective characterization of how an individual moves, loads, and adapts over time, and how functional patterns relate to symptoms, activity tolerance, and response to rehabilitation [4,5].
This demand for greater precision has accelerated the integration of bioengineering tools that capture objective, continuous, and patient-specific data [7,8]. Wearable and surface biosensors—implemented via inertial measurement units (IMUs), (multi-channel) surface electromyography (sEMG), smart textiles, and flexible sensing platforms—enable high-resolution monitoring of musculoskeletal and physiological signals and can quantify movement and muscle activation while characterizing coordination strategies and compensatory behavior. Key types of sensors and modalities, outputs, and limitations are summarized in Figure 1 and Table 2.
Beyond measurement, biosensors can support adaptive rehabilitation by enabling feedback and longitudinal tracking that inform individualized progression of exercise and lifestyle strategies. This review synthesizes current and emerging biosensor applications for LBP and outlines an implementation-oriented pathway from sensing to clinically actionable, personalized rehabilitation.
2. The Role of Biosensors: From Measurement to Meaning
To meaningfully advance clinical management of LBP, multimodal sensing must move beyond passive data capture toward clinically interpretable, reproducible measures that support individualized rehabilitation. In contrast to single time-point clinical assessments, biosensors can quantify how a patient moves and loads over time—capturing kinematics, muscle activation strategies, and activity exposure in daily-life contexts [20,21,22,23].
Importantly, biosensors do not diagnose pain mechanisms or identify a single anatomical pain generator in isolation [6]. Rather, IMU–EMG (and related) signals provide objective correlates of functional behavior, e.g., altered lumbopelvic coordination, protective co-contraction/guarding, asymmetry, reduced variability, and fatigue-related deterioration that can support clinical phenotyping and guide mechanism-informed decision-making when integrated with history, examination, imaging where indicated, and patient-reported outcomes [20,24,25,26,27]. In this sense, sensing helps operationalize “movement quality” and “stability-related behavior” in a way that is trackable and comparable across time.
Multimodal systems integrating IMUs and sEMG (Table 2), optionally complemented by pressure or physiological sensing, enable (i) task-specific quantification of spinal and lumbopelvic motion, (ii) characterization of muscle recruitment, site asymmetries and coordination strategies, and (iii) longitudinal monitoring of change during rehabilitation [28,29]. This longitudinal perspective is clinically relevant because dysfunctional patterns often emerge from intersegmental dependencies across the pelvis–spine–lower-limb chain rather than from an isolated impairment.
Beyond measurement, wearable sensing can support self-management through feedback and adherence monitoring. Real-time cues (e.g., posture reminders, movement-quality targets, muscle engagement feedback) and app-based coaching can reinforce motor retraining and facilitate sustained behavior change [30,31,32,33]. When coupled with robust preprocessing, transparent reporting, and clinician oversight—particularly for atypical or previously unseen patterns—biosensing can enable adaptive progression of exercise and lifestyle strategies within a continuous, data-informed care pathway (Figure 2). Section 3.1, Section 3.2, Section 3.3, Section 3.4 and Section 3.5 summarize the main sensing layers, while their necessity and reasons for clinical use are listed in Table 3.
3. Bioengineering Sensors in LBP Management
3.1. Wearable Sensors, Smart Textiles, and Graphene-Based Devices
Wearable technologies are increasingly used for functional assessment and longitudinal monitoring in LBP [24,30,34,35]. For clinical translation, wearables must be skin-compatible and robust over extended use, provide stable signal quality under real-world conditions, and remain scalable in cost and manufacturing. These constraints often determine translational success as much as the sensing principle itself.
Inertial sensors (accelerometers, gyroscopes, magnetometers; IMUs) can be integrated into garments or adhered to the skin to track posture, lumbar and lumbopelvic kinematics, gait proxies, and activity exposure in daily life (Table 2). Rather than “diagnosing” a source of pain, these measures help quantify functional patterns relevant to rehabilitation, e.g., altered coordination, asymmetry, reduced movement variability, or fatigue-related deterioration, especially when interpreted alongside clinical assessment and patient-reported outcomes. Signal quality metrics and placement checks are essential to avoid false “phenotypes” driven by artefacts.
Smart textiles extend this approach by embedding conductive fibers and flexible sensor arrays into clothing, supporting comfortable, low-burden monitoring suitable for home use [35,36,37,38]. Multimodal fusion (e.g., IMU with sEMG and, where relevant, pressure/force sensing) can enrich interpretation by linking how the body moves with how it is controlled, enabling a more complete description of movement strategy and compensation during daily tasks [39]. However, signal quality, placement stability, and data synchronization remain key practical limitations that must be reported transparently.
Graphene-based electronic tattoos and other ultrathin epidermal electronics represent an emerging direction for unobtrusive, high-fidelity sensing [40,41]. Their main promise lies in conformal skin contact and improved comfort during prolonged monitoring, potentially enabling higher-quality electrophysiological and physiological recordings in mobile settings. For LBP, these platforms remain largely pre-translational; their near-term value is best framed as enabling technology requiring further validation and workflow integration.
3.2. Devices for Analyzing the Muscular Component of Low Back Pain
Spinal posture and stability reflect interactions between passive structures and active muscular control. Imaging (ultrasound, MRI, CT) can reveal structural muscle changes (atrophy, fatty infiltration, asymmetry) associated with chronic LBP, but it does not capture real-time function during movement or task exposure [42].
Surface EMG offers dynamic insight into neuromuscular behavior, and multi-site/multi-channel approaches (polyEMG) (Figure 3 and Figure 4) extend conventional recordings by sampling multiple regions or muscle groups simultaneously [43,44,45]. In LBP research, such recordings have been used to characterize activation strategies, timing relationships, asymmetry, fatigue signatures, and guarding/co-contraction patterns during static postures and functional tasks [46,47]. Importantly, these signals reflect motor behavior under pain and load and should be interpreted as functional correlates rather than direct indicators of a single pathology.
When synchronized with kinematic sensing (e.g., IMU), multi-channel EMG can help link electrical activation to movement execution and reveal task-specific coordination strategies across the lumbopelvic chain. This supports individualized rehabilitation planning (e.g., targeting excessive co-contraction, improving timing/control, addressing endurance deficits) and allows objective tracking of change over time [22,48,49]. At the same time, the clinical evidence base for polyEMG in routine LBP care remains limited; studies are often small and methodologically heterogeneous, with variable protocols and outcomes. Standardized acquisition, reporting, and interpretation frameworks—together with outcome-linked validation—are therefore essential before broad clinical adoption.
Building on prior EMG and LBP rehabilitation work [50,51], long-duration surface EMG monitoring has emerged as a promising—yet methodologically demanding—approach for capturing real-world neuromuscular behavior beyond short laboratory tasks. In this line of work, the focus is on processing continuous, hours-long EMG recordings with synchronized auxiliary signals, and on incorporating an expert-in-the-loop step to improve training-set curation and model refinement when novel patterns arise (Figure 2) [52]. Such frameworks can support individualized rehabilitation by integrating patient-specific baselines with longitudinal change during therapy, under clinician oversight.
3.3. Toward Biosensing of Pain
Pain is inherently subjective and remains best captured through patient self-report using validated instruments [6]. In LBP, symptom intensity and interference can vary substantially across individuals with similar imaging findings, and pain mechanisms may be mixed and dynamic over time. These features limit any single “objective” pain measure and complicate outcome evaluation.
Current biosensors do not measure pain directly. Their value is in capturing correlates of pain-related physiology and behavior, which can complement self-report and clinical assessment [20,53,54,55,56]. Relevant domains include (i) neuromuscular patterns (e.g., guarding/co-contraction, altered timing, fatigue-related changes), (ii) autonomic arousal and recovery proxies (e.g., heart rate variability (HRV), electrodermal activity, temperature), (iii) brain-related signals in research contexts (e.g., electroencephalography (EEG) or other neuro-sensing modalities), and (iv) movement behavior and activity exposure captured via kinematics. These signals can help contextualize fluctuations in symptoms, identify task sensitivity, and track rehabilitation-relevant functional change without implying that a sensor can “verify” pain or replace the patient’s report [5,57].
A pragmatic translational direction is triangulation: combining repeated self-report (intensity, interference, function) with objective sensing during standardized tasks and in daily life, to model within-person change and treatment response [1,2,49]. This approach prioritizes longitudinal patterns, reproducibility, and clinically interpretable endpoints rather than attempting to infer a single pain generator or definitive pain “type” from biosignals alone.
3.4. Monitoring of Inflammatory and Perfusion Biomarkers
LBP is not solely biomechanical; inflammatory signaling, metabolic stress, and microcirculatory factors may contribute to symptom persistence in subgroups of patients [58,59]. Accordingly, physiological biosensing may complement neuromuscular and kinematic monitoring by providing context on systemic or local stress responses and recovery.
Low-grade inflammation has been associated with chronic pain states and may influence nociceptor sensitivity and tissue repair [4,60,61]. Emerging wearable biochemical sensors (e.g., sweat or interstitial-fluid sampling platforms) aim to detect metabolites, stress-related hormones, or inflammatory mediators, but most approaches remain early in validation and require careful interpretation due to biological variability and uncertain reference ranges [62,63]. Near-term clinical utility is therefore more plausible as trend monitoring or flare detection in defined contexts rather than as a stand-alone diagnostic.
Perfusion and oxygenation monitoring provides another complementary layer [18,63,64]. Near-infrared spectroscopy (NIRS) can non-invasively track tissue oxygenation dynamics during rest and activity and may help interpret endurance limitations or recovery delays when synchronized with EMG and kinematics. While promising, these measures also require standardized protocols and outcome-linked validation to clarify what constitutes clinically meaningful change (e.g., Oswestry Disability Index, pain interference, work ability, activity tolerance).
3.5. Integrating Biosensor Data and AI-Driven Interpretation
Here, we focus on transparent, implementation-oriented machine learning (ML) workflows (data quality control, feature engineering, and expert-in-the-loop labeling) rather than proposing a novel algorithm or reporting benchmarked performance metrics. Our emphasis is on long-duration, real-world recordings and on safe model refinement when atypical patterns occur, which are common translational failure points in wearable sensing [65,66]. Multimodal sensing generates heterogeneous, noisy, and context-dependent data. The main opportunity for ML is not “automation for its own sake,” but improving interpretability: identifying robust patterns linked to function, rehabilitation response, and clinically meaningful endpoints when models are trained and evaluated rigorously [67,68,69,70].
In LBP, ML methods have been explored for tasks such as activity recognition, detection of movement strategies (e.g., guarding/co-contraction proxies), within-person monitoring of change, and prediction of response trajectories—typically by combining IMU, EMG, and (where available) physiological features [27,55,71,72]. However, generalizability is often constrained by small datasets, inconsistent protocols, and limited external validation. For clinical translation, models should be explainable, trained on well-defined outcomes, and embedded within workflows that support clinician oversight rather than replacing judgment.
An important practical role for human oversight is handling atypical signals and unexpected patterns during real-world deployment [73]. Semi-automatic expert-in-the-loop approaches can support training-set curation, robust labeling, and safer model updates when new patterns emerge (Figure 2). Ultimately, successful integration will depend on: (i) transparent preprocessing and reporting, (ii) reference datasets linking biosensor metrics to validated clinical outcomes, (iii) interoperability standards, and (iv) interfaces that deliver actionable summaries rather than raw signals. Taken together, these elements define an implementation blueprint for clinically usable biosensing analytics rather than a claim of algorithmic novelty.
4. Implementation, Regulation, and Market Barriers
For biosensor-based technologies to move from prototypes to everyday LBP care, they must fit clinical reality. Devices should be quick to apply, robust to placement variability, and require minimal calibration, with outputs that are interpretable without specialist technical expertise [74]. Adoption also depends on workflow integration—interoperability with electronic health records, telemedicine platforms, and rehabilitation software, automated data quality control, and clinician-friendly dashboards that provide actionable summaries rather than raw streams [75,76,77]. To support clinical governance and safe use, platforms should provide a complete audit trail and model/version control (including parameter changes), ensuring traceability of outputs over time and across care settings. Scalability across settings (tertiary centers, outpatient clinics, and home-based rehabilitation) and low patient burden are equally critical for sustained use.
A major barrier is the evidence burden itself. Beyond technical performance, biosensors must demonstrate measurement validity (that they capture the intended construct), clinical reliability and accuracy under real-world conditions (motion artefacts, missing data, placement variability), and—most importantly—clinical utility (that outputs improve decisions, trajectories, or outcomes) [28]. This requires evaluation that extends from bench and laboratory studies to pragmatic clinical validation and implementation evidence (feasibility, adherence, workflow fit, and adoption), because real-world uptake often becomes the decisive test of translational value.
Implementation is also constrained by regulation, ethics, and economics. In the EU, wearable devices and software used for clinical decision support may fall under medical device regulation, and software components must align with applicable requirements under the EU MDR; AI-enabled systems additionally need to comply with emerging EU AI governance frameworks where relevant [78,79,80]. Data privacy, cybersecurity, and transparent model updating are essential, particularly for cloud-connected and remote-monitoring solutions. Finally, reimbursement and procurement models must recognize the added clinical work and infrastructure, and cost-effectiveness evidence will be needed to justify investment.
Global market momentum is driven by the high prevalence of LBP, capacity constraints in rehabilitation services, and the rapid expansion of tele-rehabilitation and home-based care [1,2,81,82,83]. However, adoption at scale will depend on demonstrating real-world effectiveness and value, and on meeting regulatory and interoperability requirements across health systems.
Despite rapid advances in biosensor hardware and analytics, clinical uptake remains limited and uneven (Table 4). Most solutions still fall short of routine requirements—validated endpoints, robust performance in real-world use, and workflow integration—so patient benefit is currently constrained to selected settings. Closing this implementation gap, rather than further incremental sensing capability, is likely the main determinant of near-term impact.
5. Future Developments
The integration of biosensing into LBP care is moving from isolated measurements toward longitudinal, clinically interpretable monitoring that can support more consistent and value-based management (Figure 5). Rather than replacing clinical judgment, the primary goal is to quantify objective correlates of function and recovery—how patients move, load, and adapt in real-world contexts—and to translate these signals into mechanism-informed decisions supported by objective correlates and validated outcomes [56,84,85,86,87].
In the coming years, biosensor-based systems are most likely to add value through treatment stratification within non-surgical care. Multimodal sensing can help characterize rehabilitation-relevant profiles (e.g., guarding/co-contraction-dominant behavior, coordination deficits, fatigue-limited endurance, activity sensitivity) and monitor how these patterns change with therapy [88,89,90]. Combined with patient-reported outcomes, such profiles can support selection and timing of interventions (exercise therapy, education/behavioral strategies, traction where appropriate, and image-guided procedures in selected cases), reducing unwarranted variation and enabling better matching between patient needs and therapeutic options [91,92].
A second near-term contribution is trajectory monitoring with early non-response flags [55,74,84,93]. Repeated sensing across daily life and standardized tasks can identify slow progress, deteriorating movement quality, poor adherence, or adverse physiological responses, prompting timely review and therapy adjustment. Importantly, these systems should function as decision support with explicit uncertainty and clear escalation rules, ensuring clinician oversight and preserving patient autonomy.
Looking ahead, the long-term vision is an incremental closed-loop model of rehabilitation. Initial implementations will remain clinician-supervised and will use simple, transparent rules and feedback to guide exercise progression and self-management [85,94,95,96,97]. As larger, outcome-linked datasets become available and governance matures, more advanced analytics may help personalize progression and predict response trajectories—provided models are interpretable, externally validated, and integrated into clinician-friendly workflows [28,98,99].
Finally, sustainable adoption will depend on implementation realities: usability, interoperability with clinical records, reimbursement alignment, and ethical governance (privacy, transparency, fairness, and safe model updates). Progress will therefore require close clinician-engineer collaboration to ensure that sensing systems deliver actionable summaries—not raw signals—and demonstrate added value in pragmatic trials and real-world implementation studies
6. Conclusions
Biosensing for LBP is advancing rapidly, but clinical uptake remains limited and uneven. Most patients cannot yet benefit in routine care because key translational requirements—outcome-linked validation, robust real-world performance, standardized reporting, and workflow/reimbursement integration—lag behind technical capability.
In the near term, the most credible impact lies in clinician-supervised decision support: treatment stratification within non-surgical care, trajectory monitoring, and early non-response flags, integrated with validated self-report and clinical assessment. Overall, closing the implementation gap—rather than incremental sensing novelty—will determine whether biosensing and intelligent analytics deliver scalable, patient-relevant benefit.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Knezevic N.N. Candido K.D. Vlaeyen J.W.S. Van Zundert J. Cohen S.P. Low back pain Lancet 2021398789210.1016/S 0140-6736(21)00733-934115979 · doi ↗ · pubmed ↗
- 2Chiarotto A. Koes B.W. Nonspecific Low Back Pain N. Engl. J. Med.20223861732174010.1056/NEJ Mcp 203239635507483 · doi ↗ · pubmed ↗
- 3Kabeer A.S. Osmani H.T. Patel J. Robinson P. Ahmed N. The adult with low back pain: Causes, diagnosis, imaging features and management Br. J. Hosp. Med.2023841910.12968/hmed.2023.0063 · doi ↗
- 4Teodorczyk-Injeyan J.A. Triano J.J. Injeyan H.S. Nonspecific Low Back Pain: Inflammatory Profiles of Patients with Acute and Chronic Pain Clin. J. Pain 20193581882510.1097/AJP.000000000000074531283548 PMC 6735949 · doi ↗ · pubmed ↗
- 5Maher C. Underwood M. Buchbinder R. Non-specific low back pain Lancet 201738973674710.1016/S 0140-6736(16)30970-927745712 · doi ↗ · pubmed ↗
- 6Nijs J. Kosek E. Chiarotto A. Cook C. Danneels L.A. Fernández-De-Las-Peñas C. Hodges P.W. Koes B. Louw A. Ostelo R. Nociceptive, neuropathic, or nociplastic low back pain? The low back pain phenotyping (BACPAP) consortium’s international and multidisciplinary consensus recommendations Lancet Rheumatol.20246 e 178e 18810.1016/S 2665-9913(23)00324-738310923 · doi ↗ · pubmed ↗
- 7Wu J. Liu H. Chen W. Ma B. Ju H. Device integration of electrochemical biosensors Nat. Rev. Bioeng.2023134636010.1038/s 44222-023-00032-w 37168735 PMC 9951169 · doi ↗ · pubmed ↗
- 8Rahman S. Sarker S. Haque A.K.M.N. Uttsha M.M. Islam F. Deb S. AI-Driven Stroke Rehabilitation Systems and Assessment: A Systematic Review IEEE Trans. Neural Syst. Rehabil. Eng.20233119220710.1109/TNSRE.2022.321908536327176 · doi ↗ · pubmed ↗