Structural Features of Nerve Guidance Conduits and Scaffolds in Preventing Axonal Misdirection: A Systematic Review of Retrograde Tracing Studies
Aleksa Mićić, Milan Aksić, Andrija Savić, Joko Poleksić, Jovan Grujić, Milan Lepić, Dubravka Aleksić, Lazar Vujić, Lukas Rasulić

TL;DR
This review examines how nerve guidance conduits and scaffolds affect axonal misdirection in nerve repair using animal studies.
Contribution
The study systematically evaluates the impact of structural features on axonal accuracy using retrograde tracing data.
Findings
Structured NGC/NSC designs showed outcomes closer to autografts compared to unstructured ones.
Current evidence lacks consistency and reliability due to high bias and small sample sizes.
No specific structure was proven superior for preventing axonal misdirection.
Abstract
Background: Axonal misdirection remains a major limitation in peripheral nerve repair. While nerve guidance conduits (NGCs) and nerve scaffolds (NSCs) have advanced structurally, it is unclear whether these designs effectively reduce misdirection compared to autografts (ANGs). This systematic review evaluates the impact of NGC and NSC structural features on axonal dispersion and reinnervation accuracy using retrograde tracing animal models. Methods: A systematic search was performed through Medline (PubMed), Scopus (EBSCOhost), and the Cochrane Library from inception to December 2024. Eligible studies included mammalian in vivo models of peripheral nerve transection repaired by direct coaptation, autografts, or artificial conduits and assessed with retrograde axonal tracing. Data on neurons labeling, innervation accuracy, and histomorphometric parameters were extracted, and misdirection…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
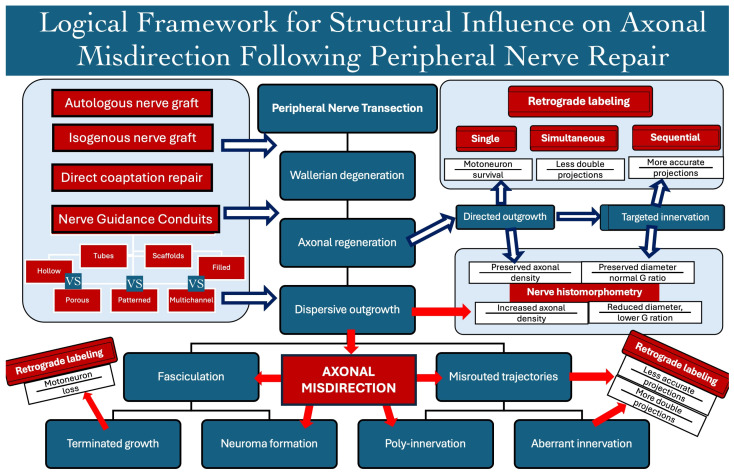 Figure 1
Figure 1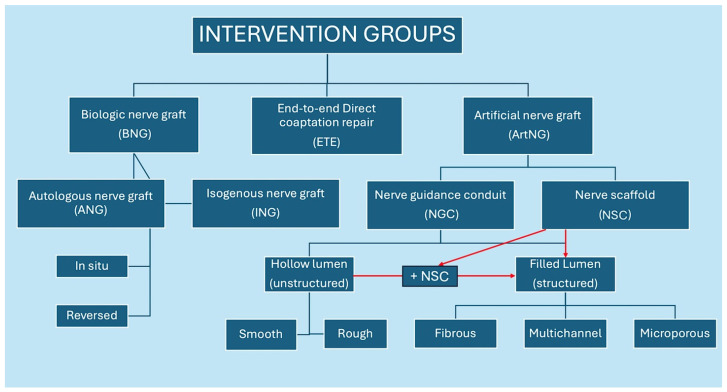 Figure 2
Figure 2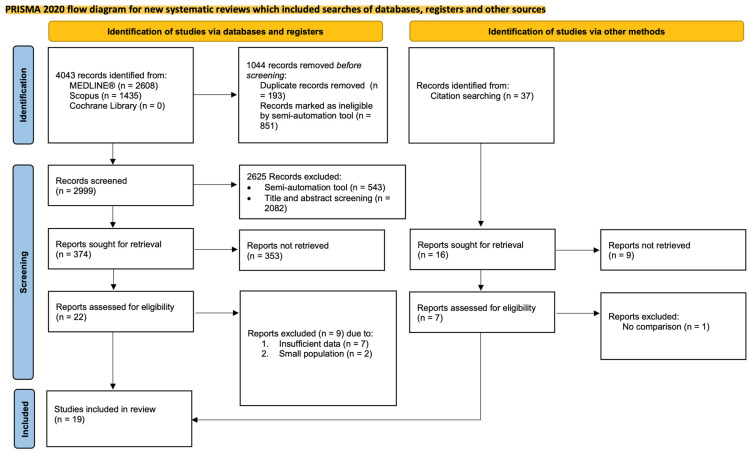 Figure 3
Figure 3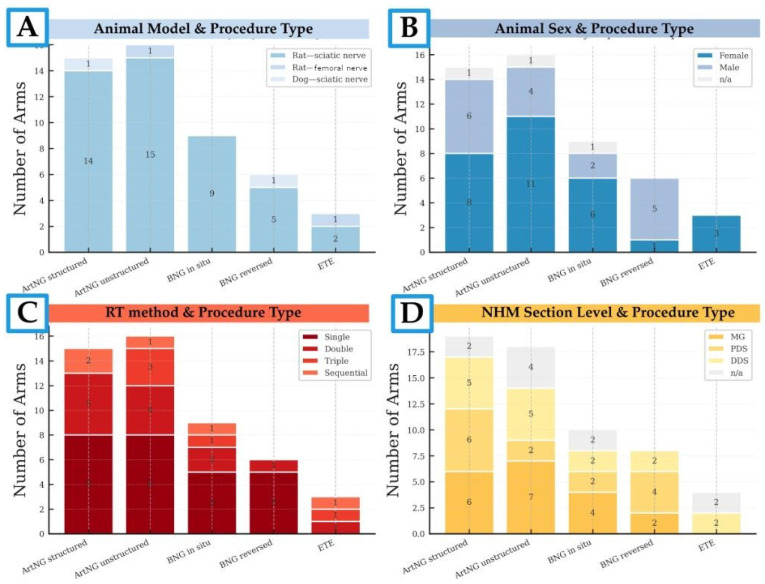 Figure 4
Figure 4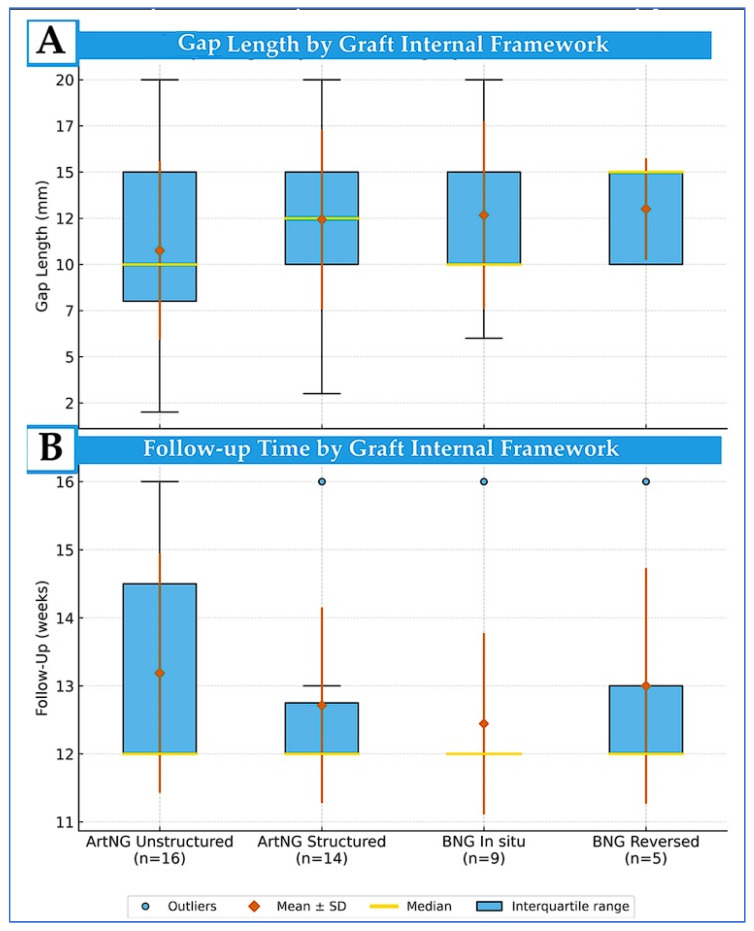 Figure 5
Figure 5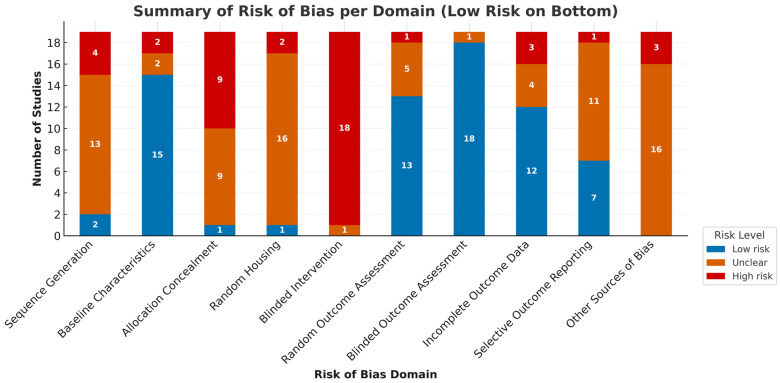 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNerve injury and regeneration · Nerve Injury and Rehabilitation · Neuroscience and Neural Engineering
1. Introduction
Peripheral nerve injuries may lead to serious functional deficits that significantly impact the quality of life of the affected individuals [1,2]. In cases of insufficient spontaneous recovery, a range of multi-disciplinary interventions may be implemented across the three divided action areas, including stimulating neural growth, treating the site of nerve injury, and maintaining the viability of the target organ [3,4]. Any failure to fulfill these criteria can have a significant impact on the final functional recovery.
In cases with a loss of nerve continuity, surgical repair of the injury site presents the primary treatment option [5]. Direct end-to-end (ETE) nerve coaptation without tension has historically been regarded as the gold standard due to its high success rates. However, in cases when tension-free coaptation is not feasible, biologic nerve grafts (BNGs), such as autologous nerve grafts (ANGs) remain the primary surgical alternative. Successfully repairing nerve defects by grafting and ensuring complete functional recovery remains a great challenge, particularly in extensive or proximal nerve injuries considered irreparable [6,7]. Although ANGs still stand as the gold standard for nerve defect repair [8], their limitations cannot be overlooked [9]. Therefore, substantial resources are devoted to advancing the development of artificial nerve grafts (ArtNGs), primarily in the form of tubular nerve guidance conduits (NGCs) or nontubular three-dimensional nerve scaffolds (NSCs) [10,11].
The main strategies in ArtNG development include the selection of the material, the fabrication method, the structural design, and functional enhancement [12,13]. Due to the failure of early ArtNG designs to ensure aligned axonal guidance over nerve gap sizes comparable to ANGs, most studies shifted their focus toward bridging over gap sizes similar to ANGs. Given the cellular and biochemical structure of ANGs which has been shown to promote axonal guidance toward distal nerve stumps most studies have concentrated on enhancing ArtNGs by integrating a variety of molecular, cellular, and physical factors and advancing biomaterial characteristics [14,15,16,17,18,19].
Although many studies have demonstrated that ArtNGs can support nerve fiber growth and facilitate regeneration towards the distal stump, simply reaching the distal end does not guarantee precise target reinnervation or the restoration of voluntary function. Most of the literature selectively reports morphological and electrophysiological outcomes, frequently presenting ArtNG repair as numerically comparable to ANG repair and emphasizing its beneficial impact on peripheral nerve regeneration. Meanwhile, it rarely assesses axonal misdirection in terms of axonal dispersion and aberrant reinnervation. Such interpretations lack deeper insight, and outcomes remain largely incomparable due to unstandardized reporting methods. Even when direct comparisons are possible, the correlations between reported outcomes generally remain weak [20,21,22,23,24,25].
Axonal misdirection (misrouting) represents its failure to reach the corresponding target organs, leading to their terminated growth or mismatched target organ reinnervation (Figure 1). It occurs due to the dispersive axonal outgrowth, its tendency for selective reinnervation, and its variable intraneural branching topography. Terminated axonal growth may involve adhesion to surrounding tissues, fasciculation, and neuroma formation. Mismatched reinnervation may involve motor axons spreading into antagonistic muscle groups, sensitive pathways, or both, as well as sensory axons spreading into muscle pathways or inappropriate sensory organs. For a long time, axonal misdirection was recognized as a significant factor contributing to poor outcomes following nerve repair, particularly in extensive injuries with large structural defects. With the advance of axonal tracing techniques, there is emerging evidence linking axonal misdirection with poor outcomes following nerve repair [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48].
Despite the significance of manipulating molecular, cellular and genetic factors to provide proper axonal guidance and innervation accuracy, only a suitable ArtNG structural configuration may have a significant impact on axonal misdirection, especially in larger nerve gaps [54,55]. The research aimed at improving conduit performance by emphasizing functional properties usually involves few enhanced structural designs and compares their impact with ANGs, while lacking an assessment of the isolated impact of the structural design and comparing how different structures with the same functional enhancement impact axonal guidance. Consequently, the scientific community lacks sufficient comparative data on structural features and their role in preventing axonal regeneration and guidance [56,57,58,59].
Most of the recently published review articles focus on functionally enhanced ArtNGs while reviews conducted on designs and fabrication strategies usually briefly cover the topic, referring to other review articles or few research studies [13,60,61]. To the best of our knowledge, no systematic review has comprehensively examined the role of ArtNG structural design in influencing axonal misdirection. Without systematically assessing and comparing axonal misdirection across various ArtNG structures, it remains challenging to identify optimal designs capable of truly matching or surpassing the functional efficacy of ANGs.
This paper aims to fill this gap by systematically reviewing various NGC and NSC design strategies with a specific focus on their potential to influence axonal misdirection. By evaluating the effectiveness of different structural features, this review will highlight key challenges and future perspectives in ArtNG optimization for the improvement of nerve regeneration and recovery.
2. Materials and Methods
A systematic review was conducted and last searched on 1 January 2025 in accordance with the PRISMA 2020 statement. The full PRISMA checklist is provided as a Supplementary Materials [62]. The review protocol was written a priori but was not registered; interested readers may obtain a copy from the corresponding author.
2.1. Eligibility Criteria
The eligibility criteria were defined using the PICO framework and are summarized in Table 1. The review includes original, peer-reviewed studies involving mammalian in vivo models with full-text availability, published in English up to the end of 2024. Only studies involving experimental groups of peripheral nerve transection injury and immediate repair using functionally non-enhanced ArtNGs in comparison with direct ETE coaptation, BNGs, or structurally different ArtNGs were considered.
To ensure the assessment of axonal misdirection, only studies that implemented retrograde axonal tracing were included. This technique was considered essential, as it is emphasized by numerous authors as the most reliable method for assessing both axonal dispersion and reinnervation accuracy following peripheral nerve repair [30,47,63,64]. A more detailed explanation of the selected outcomes is provided in the Data Items (Outcome) section (Section 2.5).
To ensure homogeneity, internal validity, and relevance to the objective of assessing the structural features of NGCs and NSCs on axonal misdirection, specific exclusion criteria were applied at the population, intervention, comparator, and outcome levels.
2.1.1. Population Exclusions
Studies involving juvenile, elderly, or genetically altered animals were excluded due to their altered regenerative capacity, which could confound comparisons between conduit designs. Models with bilateral or multiple nerve injuries or involving proximal neural structures (central motoneurons, cranial nerves, spinal cord, spinal root or nerve), were excluded because they introduce systemic or anatomical complexities unrelated to peripheral nerve conduit performance. Non-transection injury models (crush, compression, freeze, radiation, or metabolic) were excluded because they differ fundamentally in pathophysiology and regeneration dynamics from clean transection injuries. Studies that included fewer than three animals per experimental group or had a short-term follow-up period were excluded, as such designs are unlikely to provide sufficient data for valid synthesis or reliable evaluation of reinnervation outcomes.
2.1.2. Intervention Exclusions
This review focused on early repair using linear, structurally distinct ArtNGs. Studies using delayed repair, indirect techniques (nerve transfers, end-to-side (ETS) or interfascicular coaptation), or intentional misalignment at the suture site were excluded due to their divergent regenerative mechanisms. Combined interventions and two-stage procedures were excluded to avoid confounding effects from multimodal treatments. To isolate structural effects, individualized or custom-made conduits, non-linear designs (di-branched, multi-branched), and functionally enhanced ArtNGs (filled with cells, adhesive molecules, responsive hydrogels, growth factors, or made of conductive materials) were also excluded. Biological grafts such as cellular soft tissues (muscle, vein, omentum) or acellular grafts (auto-, allo-, or xenografts) were excluded, as they confound the assessment of structural design alone.
2.1.3. Comparator Exclusions
Eligible studies were required to include at least two distinct interventions (ETE/BNG vs. ArtNG) to allow a direct comparison. Studies comparing ArtNGs with identical structures made of different materials without isolating structural variables were excluded, as they did not address the primary aim of this review.
2.1.4. Outcome Exclusions
Studies were excluded if they did not provide sufficient outcome details to assess axonal misdirection. This included qualitative-only presentations such as textual interpretations of statistical significance without raw data, microscopy images with size bars but without quantitative analysis, and graphical charts lacking standard deviations or error bars. Studies using only single axonal tracing without nerve histomorphometry, or vice versa, were excluded. Short-term follow up was excluded due to insufficient time for reinnervation of the muscles and assessment using axonal tracing.
2.2. Information Sources and Search Strategy
PubMed (MEDLINE^®^), Scopus (via EBSCOhost), and the Cochrane Library were searched from inception to 31 December 2024.
A comprehensive list of keywords and MeSH terms was developed to reflect the terminology used in peripheral nerve repair and tissue engineering (Table A1). Filters applied across all platforms included the peer-reviewed publication type, full-text availability, the exclusion of reviews, systematic reviews, and meta-analyses, as well as articles mentioning “spinal cord”, “brain,” or “stroke” in the title field (Table A2).
The PubMed search strategy was constructed step-by-step (Table S1) and adapted for Scopus via the EBSCOhost interface using prompt-based assistance from ChatGPT (GPT-4, OpenAI, San Francisco, CA, USA) (Table S2). The SmartText search option was used in EBSCOhost, with peer-reviewed and full-text filters enabled. The Cochrane Library was also searched using the same strategy; no eligible studies were retrieved.
Additionally, a supplementary search in PubMed (MEDLINE^®^) was performed using the same search query but filtered for review articles, systematic reviews, and meta-analyses, to support contextualization in the Introduction and Discussion. During full-text screening, the reference lists of all included studies were manually reviewed to identify additional eligible reports.
2.3. Selection Process
All search results were imported into EndNote X20, where duplicate records were automatically identified and removed. Title and abstract screening was performed independently by two reviewers, using the predefined eligibility criteria. Semiautomated title screening was conducted using EndNote X20. Articles were grouped and excluded based on title keywords deemed irrelevant to the review objectives. This process was carried out by applying custom grouping and search rules within EndNote’s reference management system. Although automation was used to reduce the initial screening burden, manual verification was performed by same reviewers to ensure that potentially eligible studies were not inadvertently excluded. No external machine learning classifier was applied. Full-text articles were retrieved for all potentially eligible studies and evaluated in duplicate by the same reviewers. Discrepancies between reviewers at any stage were resolved through discussion. When disagreements persisted, a third independent reviewer adjudicated the decision.
If additional clarification of study details was needed, no attempts were made to contact the corresponding authors, and the studies were excluded but cited in the Excluded Studies section (Section 3.2). No automation tools, machine learning classifiers, or crowdsourcing methods were used in the study selection process. All records were screened manually. No translations were required during screening, as all included studies were published in English.
2.4. Data Collection
Data extraction was performed independently by two reviewers using a predefined piloted extraction form, with discrepancies resolved through discussion and confirmed by a third reviewer. When outcomes were presented only in graphical form, numerical data were extracted using WebPlotDigitizer v5, with interpretive and calculating assistance from ChatGPT (GPT-4, OpenAI, San Francisco, CA, USA). No other automation or translation tools were used in the data collection process.
2.5. Data Items (Outcomes)
In line with the primary objective of this study, which was to assess the structural impact of NGCs and NSCs on preventing axonal misdirection, the outcomes were selected to capture both axonal dispersion and reinnervation accuracy, recognized as the two principal indicators of misdirected regeneration. The frequently observed lack of correlation between commonly reported outcomes in experimental peripheral nerve repair research is largely attributed to the misdirected reinnervation of target organs. Therefore, retrograde axonal tracing has been emphasized as the most reliable method for assessing this phenomenon. Even though not without limitations [50,53], and with an awareness of the functional methods evolving to assess reinnervation accuracy, as well as the possibility of using immunostaining to evaluate axonal dispersion, retrograde axonal tracing currently appears to be the only viable technique capable of simultaneously assessing both axonal dispersion and reinnervation accuracy [63].
Therefore, the primary outcome sought for this study was the total number of retrogradely labeled motoneurons (LMNs). However, the sole use of LMN counts was considered insufficient for assessing axonal misdirection. Lower LMN values may result from motoneuron death rather than dispersion, while equal or even higher LMN counts compared to uninjured controls may reflect the significant misdirection of motor axons toward inappropriate targets. Such misrouting can yield misleadingly high LMN totals without translating into accurate reinnervation or functional recovery. Accordingly, the total LMN counts were always interpreted in relation to other metrics, which were selected secondary outcomes:
- LMN/LSN ratio—LMN counts relative to the number of retrogradely labeled sensory neurons (LSNs). The LMN/LSN ratio is defined as the proportion of labeled motoneurons to labeled sensory neurons, with lower ratios indicating higher misdirection of motor axons.
- TLN/TF ratio—total number of labeled motoneurons (TLN) relative to the total number of myelinated fibers (TF). To ensure comparability across studies, TF was standardized as a regenerated nerve (RN) measure, defined as values obtained at the mid-graft or distal graft; when both were reported, the mean value was used.
- Incorrect projections—The number of double or multiple labeled motoneurons following simultaneous retrograde tracing studies, expressed as a percentage of incorrectly projected neurons, indicating axonal dispersion, in the form of distal arborization and consequential polyinnervation and/or missinervation.
- Accurate projections—The number of double labeled motorneurons following sequential retrograde tracing studies, expressed as a percentage of correctly projecting neurons.
- AD/FD ratio—the relationship between axon diameter (AD) and fiber density (FD), where lower values reflect dense networks of fine sprouts indicative of axonal dispersion, and higher values reflect sparser networks of more mature fibers. Both AD and FD were standardized as RN measures, taken at the mid- or distal graft, or averaged when both sites were reported.
- TF ratios between nerve segments (e.g., MG.TF/PDS.TF, DDS.TF/MG.TF, DDS.TF/PDS.TF) indicating the extent of axonal continuity, dispersion, or loss.
All reported results that were compatible with outcome domains were sought. When studies presented multiple time points, the one closest to mid-term follow-up was prioritized, as this interval represents a standard endpoint in retrograde axonal tracing studies where axonal regeneration and target reinnervation are typically complete. Mid-term follow-up was defined as about 12 weeks in rodents, 20 weeks in rabbits, 28 weeks in cats and dogs, 32 weeks in sheep, goats, and pigs, and 38 weeks in non-human primates.
If outcome data were not uniformly reported, selection was guided by the methodological completeness and alignment with the defined concepts of axonal dispersion and reinnervation accuracy. Where numeric data were missing but derivable, values were calculated using ChatGPT (o4-Mini-High, OpenAI) and established formulas with standard deviation (SD) incorporated into every estimate and reported as approximate. SD was estimated from error bars by dividing the error bar value by the square root of the sample size (n). TF number was obtained by multiplying fiber density by the nerve cross-sectional area, with area expressed in mm^2^ or µm^2^ to match density units. FD was calculated as the fiber count divided by the analyzed area and is typically reported as fiber per mm^2^. AD was derived from available parameters using one of three approaches: subtracting twice the myelin thickness from the myelinated fiber diameter; multiplying the fiber diameter by the G-ratio (where G-ratio = axon diameter / fiber diameter); or, in cases where only G-ratio and myelin thickness were reported, calculating AD as the G-ratio multiplied by two times the myelin thickness divided by one minus the G-ratio. This approach ensured consistent interpretation across studies and allowed the integration of structurally relevant indices even when not explicitly reported.
2.6. Data Items (Other Variables)
In addition to outcomes, the following variables were extracted to describe the characteristics of the included studies and to support subgroup and sensitivity analyses:
- Study identifiers: Including the first author, year of publication, journal name, and funding.
- Population characteristics: Genus (strain), sex, weight, number of animals per group, injured nerve, length of nerve gap (mm).
- Intervention characteristics: Autologous/isogenous nerve graft orientation, artifitial nerve graft material and fabrication method, porosity, degradability, permeability, internal structure.
- Retrograde tracing methodology: The tracer compounds used, labeled nerves, and whether single, double, triple simultaneous or sequential labeling is performed.
2.7. Study Risk of Bias Assessment
The risk of bias was assessed using the SYRCLE Risk of Bias (RoB) tool, developed specifically for animal intervention studies [65]. The tool evaluates ten domains: sequence generation, baseline characteristics, allocation concealment, random housing, caregiver blinding, outcome assessment randomization, assessor blinding, incomplete outcome data, selective reporting, and other sources of bias. Two reviewers independently evaluated each included study, and discrepancies were resolved by discussion. A third reviewer verified final judgments. To support standardized and unbiased data handling, the tabulation and visual presentation of RoB results were performed using OpenAI’s GPT-5, a large language model trained on biomedical data and capable of automated evidence synthesis.
2.8. Effect Measures
Effect measures for all continuous outcomes—including total labeled motoneurons (LMN), labeled sensory neurons (LSN), total fibers (TF), fiber density (FD), and axon diameter (AD)—are reported as mean ± standard deviation (SD), where applicable. In studies using simultaneous retrograde tracing, the proportion of double- or triple-projecting neurons is expressed as a percentage (mean ± SD), where applicable. Sequential labeling studies contributed percentages of correctly directed motoneurons (mean ± SD), where applicable. Ratios derived from retrograde tracing and histomorphometric data are reported as relative numbers. As no standardized minimal clinically important difference thresholds exist for these animal models, all effect measures were calculated and reported using the original outcome-specific units to ensure consistency and comparability across included studies.
2.9. Synthesis Methods
Data synthesis was conducted in accordance with the PRISMA 2020 statement and the Synthesis Without Meta-analysis reporting framework [66] to ensure the clarity and reproducibility of our narrative approach. Studies were grouped into two primary intervention categories to evaluate the impact of different ArtNG structural designs on axonal misdirection by comparing them with direct ETE or BNG repair:
- Unstructured ArtNGs (hollow NGCs without internal framework, further categorized by architecture to smooth and rough).
- Structured ArtNGs (NSCs or filled NGCs, with internal framework, stratified by architecture to fibrous, multichannel, microporous).
ArtNGs are further divided into NGCs and NSCs, while BNGs are divided into ANGs and INGs. A schematic presentation of the classification is provided in Figure 2 and detailed rationale in the following text.
The literature does not clearly distinguish between the terms “nerve guidance conduit (NGC)” and “nerve scaffold (NSC)”. While NSCs are often used as fillers within conduits, they are also commonly used independently as bridging materials. The main difference between these two is that NCSs do not provide a lumen for a nerve stump to be placed in during the repair, which is, according to the literature, a cornerstone characteristic of NGCs.
Furthermore, while the literature traditionally categorizes NGCs into hollow, porous, micropatterned, filled, and multichannel types, we found that most conduits incorporate characteristics spanning multiple categories. For example, electrospun nanofibrous conduits are often simultaneously porous and micropatterned, and may even be filled. This overlap complicated the subgroup classification, as the lack of standardized definitions made it difficult to clearly allocate interventions into discrete categories. When key information was missing, assumptions were not made conservatively and transparently. A challenging factor was that the authors of original studies often do not define their NGCs according to these commonly used structural classifications. In many cases, classification must be inferred indirectly, through a detailed assessment of the fabrication method, materials used, or, when available, an analysis of structural images and 3D scans. Without consistent reporting, structural categorization becomes subjective, introducing potential for bias or misinterpretation during synthesis.
Due to substantial heterogeneity across studies including differences in animal models, nerve types, gap lengths, follow-up durations, conduit architectures, and outcome measures a formal meta-analysis was not feasible. Instead, a directional effect assessment with vote counting was used to determine whether individual studies favored structured or unstructured ArtNGs for applicable outcome domain. Studies were further stratified into three comparison groups based on intervention characteristics and outcome assesment methods.
Direct ETE repair versus ArtNG repair.ANG versus ArtNG repair assessed by single-dye tracing methods.ANG versus ArtNG repair assessed by multiple-dye tracing methods.
Directional effect was assessed for each outcome domain by comparing ArtNGs with ANG or ETE. An upward arrow (↑) indicated a favorable outcome for ArtNGs, while a downward arrow (↓) indicated a favorable outcome for ANGs. Equality signs (=) denoted no clear difference, based on overlapping SDs, a mean difference of less than 10%, or non-significant p-values. The exception was for incorrect projecting LMNs, where lower values indicate better outcomes and ↑ was assigned when ArtNGs showed fewer misdirected motoneurons than ANGs.
When authors reported statistical tests or variance (SD/CI), classification followed the reported significance (α = 0.05). When variance was unavailable, a ±10% threshold versus the comparator was applied. Classifications based on thresholds are interpreted as directional trends, not statistical effects. Vote counting was then applied across these groups, providing the number of study arms that favored ArtNGs (↑), favored ANGs (↓), or showed no effect (=). This approach enabled identification of overall trends without requiring statistical pooling.
The heterogeneity was assessed by comparing distributions across subgroups using SPSS v.29 and visually through box plots. The certainty was qualitatively assessed using the GRADE domains (http://www.gradeworkinggroup.org/publications/JCE_series.htm, accessed on 30 April 2025):
- Risk of bias: based on SYRCLE tool
- Heterogeneity: noted when SD of the study means was large (>50% of mean)
- Indirectness: variation in species (rat vs. dog) or gap length
- Imprecision: small n of study arms per group (<5)
- No publication bias assessment was possible.
By adhering to both PRISMA and SWiM guidelines, this approach ensures the transparent, reproducible, and comprehensive synthesis of ArtNG structural features and their impact on axonal misdirection. Results were presented in structured summary tables, with bar graphs, and box plots used to visualize distributions across studies.
2.10. Automatization Tools and Language Based Models
ChatGPT (OpenAI, GPT-4) was used as a secondary tool to support data handling and manuscript preparation. Its use was limited to non-analytical, supportive functions, including (1) formatting tables and figures, (2) refining the clarity and consistency of written text, and (3) approximating numerical values from graphical data when not explicitly reported in the text. The tool was used to double-check manually extracted or formatted data, and all outputs were subsequently reviewed by human investigators to resolve any discrepancies and ensure accuracy. The inclusion of this additional verification layer enhanced the quality and consistency of the review but also extended the production timeline relative to a standard workflow. ChatGPT did not perform study selection, data extraction, or risk of bias assessment, all of which were conducted manually by independent reviewers.
3. Results
3.1. Study Selection
The search strategy identified a total of 4043 articles (Figure 3). Before screening, 1044 records were removed (193 duplicates and 851 records marked as ineligible by a semi-automation tool) leaving 2999 records for title/abstract screening. During the title and abstract review, 2625 were excluded (543 by the semi-automation tool and human confirmation and 2082 after complete human screening) leaving 374 reports for retrieval. Upon retrieval, 22 records were selected for full-text review, out of which 7 were excluded due to insufficient data and two due to small population, leaving 13 studies for inclusion.
From 37 additional records identified from citation searching, 7 records were assessed for eligibility out of which 6 were included and one was excluded due to lack of comparison group.
3.2. Excluded Studies
Several promising studies were excluded due to insufficient motoneuron labeling data, small sample sizes, or incomplete reporting [68,69,70,71,72,73,74,75,76].
3.3. Study Characteristics
Of the 19 included studies comprising 49 experimental groups (Table 2), the rat sciatic nerve (SN) model was most frequently employed, represented in 17 studies encompassing 45 groups (Figure 4A). Sprague–Dawley rats were the predominant strain (n = 29 groups), followed by Lewis (n = 13) and Wistar (n = 5). Female animals were used in the majority of groups (n = 29), with the remainder including male (n = 17) or unspecified sexes (Figure 4B). The rat femoral nerve and dog sciatic nerve models were used in singular studies, involving 2 groups each.
Retrograde axonal labeling methods were variable across included studies (Figure 4C). Single-labeling was most common (26 groups), with 21 using Fluorogold (FG) and 3 using DiI on the SN, while two using FG on the tibial nerve. Double-labeling accounted for 13 groups—eleven employed Diamidino Yellow (DY) on the peroneal nerve and Fast Blue (FB) on the tibial nerve, while two used True Blue (TB) and DiI on femoral motor and sensory branches. All five triple-labeling studies utilized the DiI/FB/FG combination (DiI to the tibialis anterior branch, FB to the gastrocnemius branch, and FG to the peroneal motor branch). Out of five groups that used sequential labeling: three applied TB followed by FG on the tibial nerve, and two applied TB followed by DiI on femoral nerve branches.
Nerve histomorphometry was reported in 39 groups, including all single-labeled and all double-labeled groups (Figure 4D). Multiple anatomical levels were assessed in 26% of these groups, out of which 7 in single-labeling and 3 in double-labeling studies.
The distribution of gap lengths and follow-up durations across graft categories for 45 experimental groups is shown in Figure 5. The groups treated with ArtNGs exhibited the greatest variability due to inclusion of three studies with ArtNG application in short-gap models (2–5 mm) to compare with direct ETE repair. Follow-up duration showed less variability, with all graft categories displaying a median of 12 weeks and mean values between 12.5 and 13.0 weeks (IQRs: 12–13 to 12–14 weeks).
3.4. Risk of Bias in Studies
The results of the risk of bias assessment are summarized in both tabular format and a color-coded heatmap (Table A3, Figure 6), presenting each domain’s risk judgment (low, unclear, or high) across all studies. The studies demonstrated a generally low methodological quality, with multiple domains at high or unclear risk.
Blinding of intervention was the most consistently problematic area, with 18 studies rated as high risk, suggesting that performance bias is a major concern across the evidence base. Random housing was also poorly addressed, with only three studies providing low-risk methods, while allocation concealment and sequence generation were frequently either inadequately described or at high risk, limiting confidence in the randomization process. In contrast, outcome-related domains such as blinded outcome assessment and random outcome assessment were more robust, with the majority of studies rated as low risk. However, incomplete outcome data and selective reporting varied, and many studies did not provide sufficient information to judge the presence of reporting bias or other potential sources of bias.
3.5. Results of Individual Studies
Individual study results are provided in Table S3. Key outcomes are presented below by domain and stratified by comparator group with directional effect and vote counting used to summarize study findings.
3.5.1. LMN Counts
Total LMN counts were provided for all 19 studies. Results are summarized below according to comparator groups.
ArtNG vs. Direct ETE Repair
In all 3 studies comparing unstructured ArtNGs and direct ETE repair there were no significant differences in total LMN counts between the intervention and comparator group (Table 3). However, in 2/3 cases there was a Δ ≥ 10% mean difference, compared to ETE. There were no records comparing structured ArtNGs with direct ETE repair.
ArtNG vs. ANG Repair
Out of 28 ArtNG arms, 26 had study level ANG comparator, out of which 10 provided similar and 16 provided lower LMN counts compared to ANGs (Table 3). Of these 16, eight were significant at p < 0.01, four at p < 0.05, and four were reported as ≥10% decreases without p-values (Table 4 and Table 5.)
Unstructured ArtNG arms, provided similar LMN counts in 2/11 and lower in 9/11 cases compared to ANGs.Structured ArtNG arms provided similar LMN counts in 8/15 and lower in 7/15 cases compared to ANGs. In 5/5 cases, longitudinal multichannel NSCs led to similar LMN counts, while randomized multichannel NSCs (2/2) and multichannel NGCs (3/3) led to lower LMN counts in all scenarios. Fibrous designs led to similar LMN counts in 3/5, and lower in 2/5 cases compared to ANGs.
3.5.2. TLN Counts and Associated Ratios
Out of 13 ArtNG arms with TLN counts reported, 11 had study level ANG comparator. Out of 11, five were structured and 6 were unstructured.
Structured ArtNG arms matched ANGs in TLN counts in 4/5, LSN counts in 3/5, and LMN/LSN ratio in 4/5 cases. LSN counts exceeded ANGs in one case. Regarding TLM/TF ratio, structured ArtNGs were similar to ANGs in one and superior in other case, out of two.Unstructured ArtNG arms matched ANGs in TLN counts in 1/6, LSN counts in 1/6 and LMN/LSN ratio in 3/5 cases. Regarding TLM/TF ration, unstructured ArtNGs were superior to ANGs in 4/5 and inferior in 1/5 cases.
3.5.3. Motoneuron Projection Accuracy
Projection accuracy metrics were provided in 8 studies out of which 3 compared ArtNGs with direct ETE repair and 5 compared ArtNGs with ANGs (Table 5).
ArtNG vs. Direct ETE Repair
Across three short-gap neurorrhaphy comparisons, LMN survival was similar between ETE and conduits, but projection specificity diverged by design. In rats with hollow silicone NGCs, Bodine-Fowler et al. 1997 [77] found no difference in accurate projecting LMNs versus ETE (14 ± 5 vs. 19 ± 9). Valero Cabre et al. 2004 [79] also saw comparable LMN counts but a higher proportion of incorrect projections with silicone NGC than ETE (6.3% vs. 2.2%, p < 0.05), indicating worse specificity. In contrast, Yu et al. 2015 [85] (femoral nerve, 2-mm gap) reported better targeting with chitosan tubulation: incorrect projections were lower than ETE (74 ± 11 vs. 112 ± 13, p < 0.05) and accurate projections were higher (68.18 ± 2.04% vs. 55.89 ± 1.63%, p < 0.05).
ArtNG vs. ANG Repair
Structured ArtNGs had lower percentage of incorrect projecting LMNs compared to ANGs in 4/7, similar in 2/7, and higher in 1/7 cases. Accurate projecting LMNs were reported only for the two arms and were similar to ANG in both cases.Unstructured ArtNGs provided similar percentage of incorrect projecting LMNs as ANGs in 3/5 and lower percentage in 2/5 cases. There were no data about accurate projecting LMNs across unstructured ArtNG arms.
3.5.4. Other Outcomes
RN.AD/RN.FD ratios were reported in four studies (n = 13 arms). In short-gap models, structured conduits (0.06–0.13) aligned closely with autograft controls (0.05–0.13), whereas unstructured conduits produced higher ratios (0.15–0.44). In one long-gap study [87], both structured (9.85) and unstructured (20.79) exceeded in situ autograft values (9.76). No variance data were available, so these results are presented descriptively.
Structured ArtNGs had similar AD/FD ratios in 2/5, lower in 2/5 and higher in 1/5 arms, when compared to ANGs.Unstructured ArtNGs had higher AD/FD ratios in 2/2 arms when compared to ANGs.
TF ratios between nerve segments were rarely reported, preventing any meaningful interpretation or directional analysis.
3.6. Synthesis of Results
Overall, structured ArtNGs demonstrated outcomes more closely aligned with ANG repair, while unstructured ArtNGs generally underperformed. Certainty of evidence across all domains was rated as very low, reflecting high risk of bias in included studies, small sample sizes, incomplete reporting of variance data, and indirectness inherent to animal models (Table 6).
LMN counts: In 26 arms with ANG comparators, structured ArtNGs preserved LMN numbers in approximately half of cases (8/15), with longitudinal microchannel NSCs consistently matching ANGs (5/5). In contrast, unstructured ArtNGs provided similar LMN counts in only 2/11 arms, with 9/11 showing reductions.TLN counts: Structured ArtNGs preserved TLN in 4/5 arms, whereas unstructured guides showed preservation in just 1/6, with the remainder reporting decreases.LSN counts: Structured conduits preserved LSN in 3/5 arms and exceeded autografts in one arm, while unstructured conduits preserved LSN in only 1/6, with reductions in the others.LMN/LSN ratio: Structured conduits preserved motor–sensory balance in 4/5 arms, whereas unstructured guides were preserved in 3/5 but decreased in 2/5 arms.Projection accuracy: For incorrect projecting LMNs, structured conduits outperformed autografts in 4/7 arms, were similar in 2/7, and worse in 1/7; accurate projections were reported in only two structured arms, both comparable to ANG. Unstructured conduits reduced misdirected projections in 2/5 arms, matched in 3/5, and did not report accurate projection data.
3.7. Risk of Bias Due to Missing Values
Since only one outcome was consistently reported across all study groups, while the remaining outcomes did not exceed values of 50%, a pooled quantitative analysis could not be performed. The included studies were highly heterogeneous in terms of design, interventions, and reported endpoints. Furthermore, we judged the studies to carry a high risk of selective outcome reporting, as key functional and histological parameters were frequently missing or incompletely presented.
3.8. Certainty of Evidence
The overall certainty of evidence in this review is low to very low due to methodological limitations, small sample sizes, risk of bias, inconsistency, and imprecision across studies. While autografts consistently show benefits for motoneuron survival and regeneration, and structured NGCs may reduce axonal misdirection, the evidence is limited and uncertain, emphasizing trends rather than definitive conclusions.
4. Discussion
This systematic review provides the first comprehensive analysis of the structural impact of ArtNGs on axonal misdirection following peripheral nerve repair, focusing on studies implementing retrograde axonal tracing. Because of the lack of consensus on structural classification and the limited subset of features tested using, we adopted a pragmatic dichotomy: (1) structured (scaffolds and tubular conduits with internal framework and (2) unstructured (tubular conduits without internal framework). Despite this simplification, the evidence consistently indicates that structured ArtNGs more often performed similarly to or better than unstructured conduits, while ANGs remained superior across all domains. Because no single outcome providing assessment of axonal misdirection was reported in more than half of the experimental arms and overall certainty was very low, these observations should be interpreted as suggestive trends, not definitive conclusions.
The NGCs have been considered as significant factor that reduce axonal dispersion at the proximal stump [26] and provide initial directional alignment toward the distal stump [75,76], positioning this as a fundamental mechanism of nerve regeneration and recovery. However, no studies were identified that quantitatively assessed the impact of NGC structural design on proximal stump dispersion. In this review, only three included studies directly compared epineurial ETE with unstructured NGCs reporting similar, occasionally slightly higher LMN counts with NGCs. This may be due to the larger internal space of hollow conduits allowing more extensive axonal dispersion, whereas epineurial sutures may cause direct or indirect fiber trauma, with the interstump space further influenced by fibrin glue or fibrotic tissue formation.
Despite consistently reported equal LMN counts, the precision of reinnervation is generally reduced and, in some cases, increased. Reduced precision could be due to selective reinnervation driven by stronger distal cues, which in tubulation repair have more space and more fibers available to attract towards incorrect targets. While most of such studies used impermeable silicone hollow NGCs, in only case where ArtNGs achieved better reinnervation than direct ETE repair, the conduit was biodegradable and permeable. Such results should be reassessed as a potential consequence of a reduced selective reinnervation or diminished inhibition from sensory fibers toward motor fibers due to wall permeability and dilution of distal molecular factors. The dilution of distal molecular factors could be considered as contributing factor, regarding the satisfactory results in two studies when comparing non-soluble tube with epineurial ETE repair for distal coaptation site of autologous nerve graft [94,95].
This interpretation may be further supported by the findings of Liu et al. [89] the only included study to demonstrate superiority over ANG in reducing numbers of misdirected motoneurons. Notably, Liu et al. used structured fiber filled NGCs, which may have contributed to this outcome by reducing the influence of distal molecular cues through immediate physical guidance from its internal fibrous framework. This design provides a direct trajectory for axonal regrowth and limits the gap where distal misdirection could occur, particularly at a stage when distal molecular factors are already diluted.
The results of our studies aligns with the findings from earlier key experimental studies such as those by De Ruiter et al. [80] and Yao et al. [55], which showed that although structured conduits can mimic fascicular architecture, they still result in greater rates of double projections and lower reinnervation precision compared to ANGs. Studies using multichannel ArtNGs (Zhang et al., 2011 [83]; Bozkurt et al. 2016 [86]; Daly et al., 2012 [31]) showed an intermediate performance—better than hollow designs but not matching the fidelity of ANGs. Contrastingly, prior reviews often emphasized only histomorphometric or functional outcomes, without specifically assessing the reinnervation accuracy. This led to overly optimistic comparisons between NGCs and ANGs. Our review corrects this by integrating motoneuron labeling data and dispersion indices, revealing frequent misdirection in even structurally advanced NGCs.
The observed limitations of NGCs despite structural innovations reflect the complexity of axonal pathfinding, influenced not only by the luminal architecture but also by fascicular topography and intrinsic neuronal properties. Therefore, the current results underscore a growing consensus in the literature that physical guidance alone is insufficient for achieving target-specific reinnervation.
4.1. Limitations of the Evidence
The evidence included in this review is subject to several limitations that affect the overall certainty and generalizability of the findings. Most studies were preclinical and relied on small animal models (predominantly rat SN), limiting their translational relevance to human nerve repair. Sample sizes were frequently small, and many studies lacked key methodological safeguards such as randomization, blinding, or prospective protocol registration, increasing the risk of bias. Furthermore, significant heterogeneity was observed in conduit materials, fabrication methods, defect lengths, follow-up durations, and outcome metrics, complicating direct comparisons across studies. Reporting was often incomplete or selective—particularly regarding misdirection outcomes—leading to potential reporting bias. Finally, while retrograde tracing is the gold standard for assessing reinnervation accuracy, it remains a technically complex method with variable reproducibility, contributing to uncertainty in interpreting misdirection rates.
4.2. Limitations in the Review Process
Several limitations in the review processes may have influenced the findings of this systematic review. First, although a review protocol was written a priori, it was not registered in a public database, which may reduce transparency and increase the risk of post hoc changes to the eligibility criteria or analysis plans. Second, while data extraction and risk of bias assessment were performed in duplicate, with conflict resolution by a third reviewer, no attempts were made to contact the authors of studies for missing or unclear data, potentially leading to the exclusion of relevant information. Third, due to the methodological heterogeneity of the included studies, no meta-analysis was performed, limiting the ability to generate pooled effect estimates. Instead, a narrative synthesis following SWiM guidelines was used, which, although structured, remains inherently more subjective. Lastly, while automated tools were used to extract numerical data from figures, manual verification was not always possible, which may introduce minor inaccuracies. Together, these limitations may have introduced bias, reduced reproducibility, and affected the strength of conclusions.
4.3. Implications for Practice and Policy
The findings of this review suggest that while structured ArtNG designs, such as multichannel and fibrous tend to improve axonal guidance compared to unstructured hollow conduits, they do not yet match the reinnervation accuracy achieved with ANGs. Therefore, ArtNG should not currently be considered as replacements for autografts in clinical scenarios where precise functional recovery is critical, especially in large nerve gaps. However, structured designs may be considered as alternatives in select cases where autograft harvest is not feasible, particularly in small- to mid-sized nerve defects.
From a policy standpoint, the results highlight the need for stricter preclinical validation standards before novel ArtNG are translated into human use. Regulatory frameworks may benefit from incorporating axonal misdirection as a required outcome in preclinical conduit evaluation, rather than relying solely on general markers like fiber count or functional indices.
5. Future Perspectives
The following recommendations should be considered in future research regarding advancement of NGCs and NSCs:
- Adopt standardized and comprehensive outcome reporting. Future studies should consistently include retrograde tracing alongside histomorphometry to assess both axonal dispersion and reinnervation accuracy.
- Improve methodological rigor. Prospective protocol registration, randomization, blinding, and complete outcome reporting should become standard practice in preclinical nerve regeneration research.
- Use larger animal models and longer follow-up periods. These steps would enhance the clinical relevance of findings and better simulate human nerve injury and repair conditions.
- Isolate structural effects. Future experimental designs should separate the impact of the conduit structure from functional enhancements such as growth factors, stem cells, etc., to clarify the contribution of architecture alone.
- Explore personalized, AI-assisted NGC design. Emerging imaging and 3D printing technologies, combined with machine learning, offer promising avenues for the development of patient-specific NGCs that replicate native fascicular anatomy.
- Improve biomaterials, to provide microenvironment for axonal growth, by maintaining its physical structure, while being able to dissolve immediately when axons reach the distal stump.
Personalized 3D printed conduits with tubular branching patterns that match the intraneural fascicular topography of a patient sound promising as a future advance in NGC designing strategy.
Johnson et al. [96] demonstrated the usage of a 3D scanner for the intraoperative visualization of rat proximal and distal nerve stump morphology, computational design modeling, and the printing of tailored NGCs to match the stump fascicular distribution. Zhu et al. [97] developed a rapid continuous 3D printing platform for the fabrication of NGCs with various architectures and the adjustment of structural parameters to match the mechanical properties of the injury site.
In one study, Yao et al. demonstrated the usage of micro-magnetic resonance imaging (micro-MRI) for the scanning of fresh human nerve samples and their incorporation into computer software for 3D reconstruction [98]. In another study, Yao et al. used 3T MRI to scan patients’ healthy nerves at the contralateral side and designed a tailored nerve graft according to information from a previously formed database, in accordance with the specific injury situation [99].
Chang et al. [100] used serial histology sections, 3D reconstruction software, and computer-aided design to create a tailored NGC based on the fascicular topography of a rat sciatic nerve. Machine learning may be used in NGC computational design according to data from the created database [101,102].
Diffusion tensor imaging (DTI) plays a crucial role in nerve repair surgeries by providing pre-surgical insights into nerve pathways and the extent of damage [103]. Given its current role in assessing nerve integrity, DTI may also be utilized in the future for precise NGC placement, further improving targeted nerve regeneration and repair outcomes.
6. Summary
No current evidence clearly identifies the significant impact or superiority of any of the ArtNG structural designs, as studies vary widely in design, materials, and outcome reporting. Structured conduits with longitudinally oriented channels or fibers tend to improve axonal guidance over unstructured hollow designs, but still fall short of the precision achieved with ANGs. While small gap tubulation repair by ArtNGs may offer clinical potential, more standardized and rigorous research is necessary to fully understand potential of different structures and their role in the development of advanced, multifunctional, personaliyed, and AI-calibrated conduits with ultimate tendency to overcome ANGs
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akbari H. Saraee A. Mirzaei L. Abolfazli M. Bagheri H. Akbari P. Comparison of Functionality Level, Disability and Quality of Life in Subjects with Peripheral Nerve Repair in the Upper Extremity World J. Plast. Surg.202413687310.61186/wjps.13.2.6839193248 PMC 11346686 · doi ↗ · pubmed ↗
- 2Wong C.R. Karpinski M. Davidge K.M. Klassen A. Dengler J. Patient-reported Outcome Measures for Peripheral Nerve Injuries: A Systematic Review Plast. Reconstr. Surg. Glob. Open 202412 e 640810.1097/GOX.000000000000640839703380 PMC 11658760 · doi ↗ · pubmed ↗
- 3Faroni A. Mobasseri S.A. Kingham P.J. Reid A.J. Peripheral nerve regeneration: Experimental strategies and future perspectives Adv. Drug Deliv. Rev.201582–8316016710.1016/j.addr.2014.11.01025446133 · doi ↗ · pubmed ↗
- 4Grosu-Bularda A. Vancea C.V. Hodea F.V. Cretu A. Bordeanu-Diaconescu E.M. Dumitru C.S. Ratoiu V.-A. Teodoreanu R.-N. Lascar I. Hariga C.-S. Optimizing Peripheral Nerve Regeneration: Surgical Techniques, Biomolecular and Regenerative Strategies-A Narrative Review Int. J. Mol. Sci.202526389510.3390/ijms 2608389540332790 PMC 12027958 · doi ↗ · pubmed ↗
- 5Costa N.N. Santos J.F.D. Aranha M. Coelho E.W.F. Paes V.L.S. Oliveira R.C.S. Repair methods in peripheral nerves after traumatic injuries: A systematic literature review Acta Cir. Bras.202540 e 40122510.1590/acb 40122540008718 PMC 11849802 · doi ↗ · pubmed ↗
- 6Bertelli J.A. Tuffaha S. Sporer M. Seltser A. Cavalli E. Soldado F. Hill E. Distal nerve transfers for peripheral nerve injuries: Indications and outcomes J. Hand Surg. Eur. Vol.20244972173310.1177/1753193423122616938296247 · doi ↗ · pubmed ↗
- 7Rasulic L. Savic A. Grujic J. Micic A. Radojevic S. Ivic J. Lepic M. Distal nerve transfer (PT-AIN, SUP-PIN) for regaining hand function in C 8, T 1 root injury following extirpation of the right C 8, T 1 schwannoma Neurosurg. Focus Video 20238 V 1010.3171/2022.10.FOCVID 2211036628090 PMC 9815237 · doi ↗ · pubmed ↗
- 8De Leonibus A. Rezaei M. Fahradyan V. Silver J. Rampazzo A. Bassiri Gharb B. A meta-analysis of functional outcomes in rat sciatic nerve injury models Microsurgery 20214128629510.1002/micr.3071333511636 · doi ↗ · pubmed ↗