Clinical Effectiveness of Barrier Preparations in the Management of Diaper Dermatitis: A Systematic Review and Meta-Analysis
Zainab Z Alkhamis, Muskaan Bhagchandani, Mumin Idris, Yusuf Bhyat, Sara M Alsani, Arfa I Pasha, Ahmed Hesham Atif Ali, Dhuha Ali Eledresi, Alaa Ahmed Mahdi, Fatimah Ridha Almohamedhusain

TL;DR
This study reviews how well barrier preparations work for treating diaper rash in infants and preschoolers.
Contribution
The study provides a meta-analysis of barrier preparations' effectiveness in managing diaper dermatitis.
Findings
Clotrimazole and zinc oxide paste were effective in reducing diaper dermatitis.
Petroleum jelly or Vaseline showed no efficacy in one study.
Effectiveness varies by preparation and study design.
Abstract
The inflammatory skin condition known as diaper dermatitis (DD) often affects infants and preschoolers. Barrier preparations are commonly used in their management, but their effectiveness remains unclear. This systematic review aimed to evaluate the extent to which barrier preparations reduce DD compared to a placebo or other therapies. To gather relevant information, we conducted electronic searches on databases such as Medical Literature Analysis and Retrieval System Online (MEDLINE) via PubMed, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar for data extraction. We included studies based on randomized controlled trials (RCTs), quasi-randomized controlled studies, and cohort studies. The collected data were analyzed using RevMan version 5.3 (The Cochrane Collaboration, London, United Kingdom) for Windows. This study included a total…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
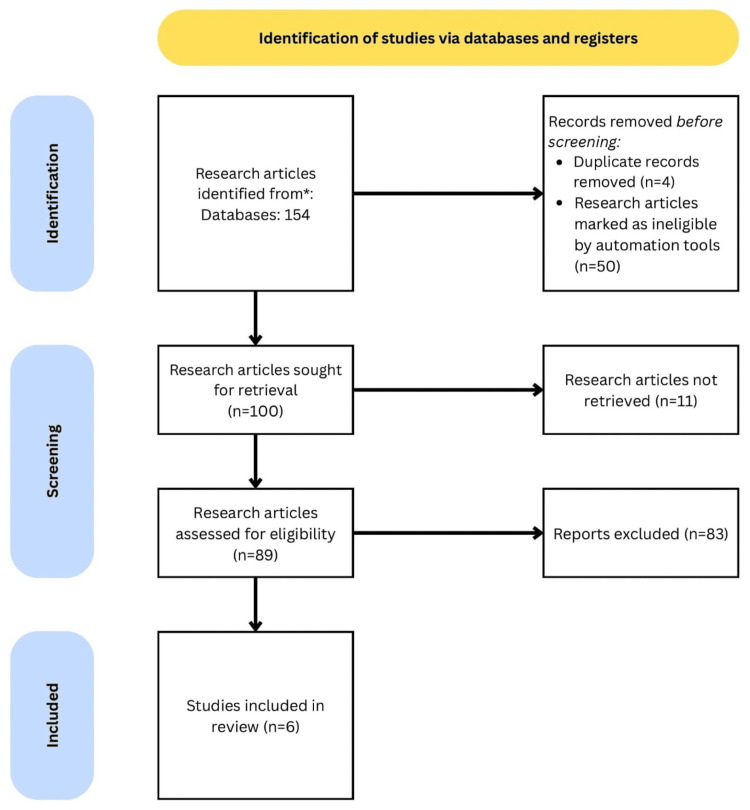 Figure 1
Figure 1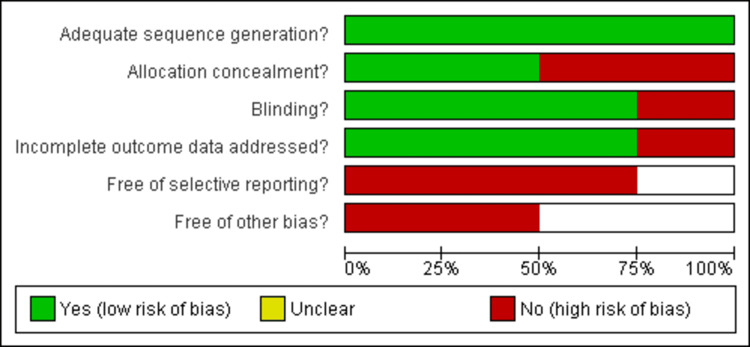 Figure 2
Figure 2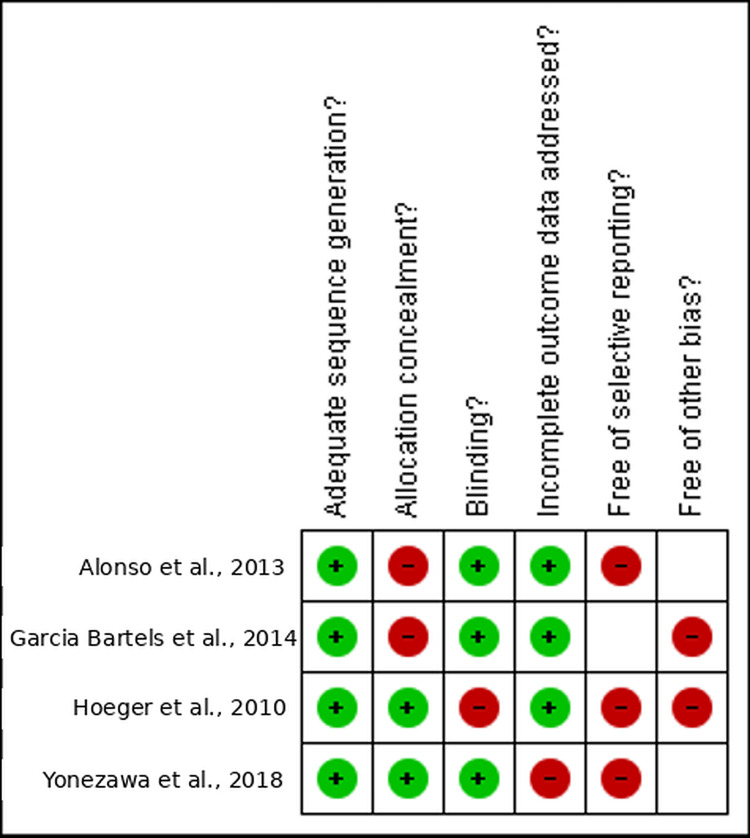 Figure 3
Figure 3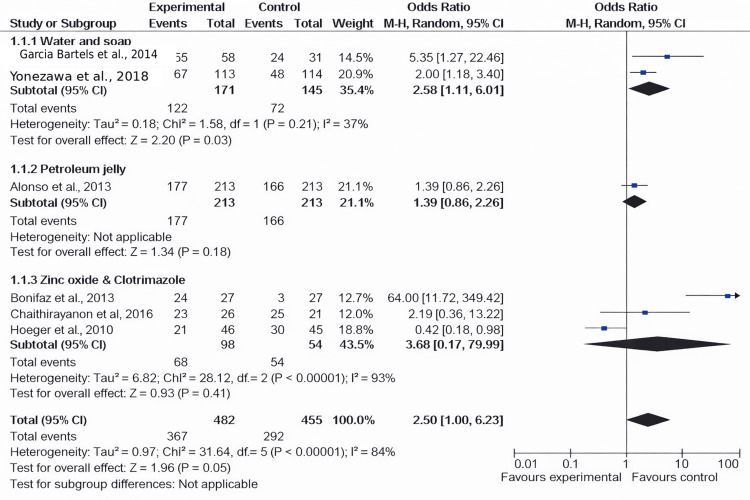 Figure 4
Figure 4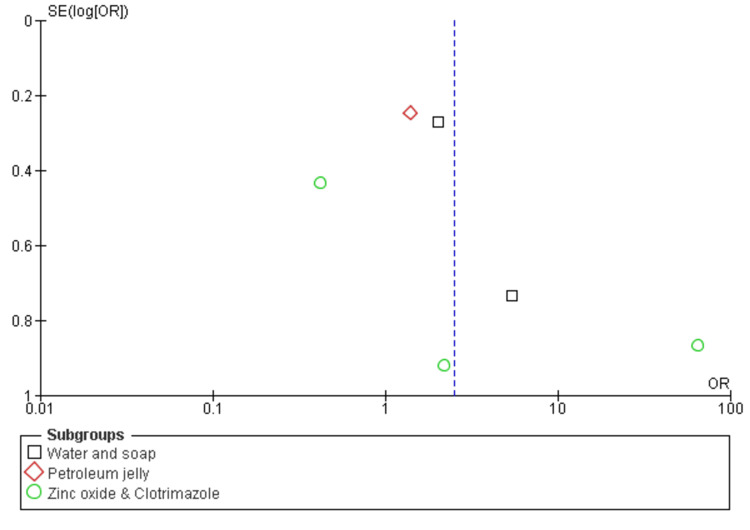 Figure 5
Figure 5| Questions |
Bonifaz et al., 2013 [ |
Chaithirayanon et al., 2016 [ |
| Were the two groups similar and recruited from the same population? | Yes | No |
| Were the exposures measured similarly to assign people to both the exposed and unexposed groups? | Yes | Yes |
| Was the exposure measured in a valid and reliable way? | Yes | No |
| Were confounding factors identified? | No | Yes |
| Were strategies to deal with confounding factors stated? | Yes | No |
| Was the follow-up time reported and sufficient to be long enough for outcomes to occur? | No | Yes |
| Was an appropriate statistical analysis used? | No | Yes |
| Were strategies to address incomplete follow-up utilized? | Yes | No |
| Was a follow-up completed, and if not, were the reasons for failure to follow-up described and explored? | Yes | Unclear |
| Were the outcomes measured in a valid and reliable way? | Yes | Unclear |
| Were the groups/participants free of the outcome at the start of the study? | No | Yes |
| Were strategies to address incomplete follow-up utilized? | No | Yes |
| Author and year | Country | Study population and sample size | Age of the children | Type of design | Type of barrier preparation | Number of infants with a decrease in the severity of nappy dermatitis | Prevention of diaper dermatitis |
|
Alonso et al., 2013 [ | Spain | 426 neonate population: 213 in experimental neonates and 213 in control | 18 months | Randomized controlled trial | Petroleum jelly | Petroleum jelly (Vaseline group): 177; control group: 166 | Not significantly lowered |
|
Yonezawa et al., 2018 [ | Japan | 227 babies: 113 in the experimental group and 114 in the control | One week and three months | Randomized controlled trial | Water and soap | Water and soap: 67; control: 48 | Improved skin dermatitis effectively |
|
Hoeger et al., 2010 [ | Germany | 96 infants: 46 in the zinc oxide paste group and 45 in clotrimazole | 6-18 months | Randomized controlled trial | Zinc oxide paste and clotrimazole (hydrozole) | Zinc oxide paste: 21; clotrimazole: 30 | Both improved symptoms, but the efficacy of zinc oxide paste is notably low than clotrimazole (hydrozole) |
|
Chaithirayanon et al., 2016 [ | Thailand | 50 infants: 25 in zinc oxide and 25 in talcum | 6-12 months | Cohort study | Talcum and zinc oxide cream | Recovery time: 3.7 + 3.3 days in the zinc oxide group and 2.7 + 0.5 days in talcum and 23 in the zinc oxide group and 21 in talcum | Zinc oxide was effective in treating symptoms with less adverse events |
|
Bonifaz et al., 2013 [ | Mexico | 27 infants | 2-22 months | Prospective study | Clotrimazole | 24 recovered out of 27 | Clotrimazole is effective for disease management |
|
Garcia Bartels et al., 2014 [ | Germany | 89 healthy infants: 58 with cream of clotrimazole and 31 with wet wipes | Nine months | Randomized controlled trial | Water and moisturized wipes | 55 recovered; 24 recovered | Clotrimazole is more effective than wet wipes or clothes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal skin health care · Infant Development and Preterm Care · Wound Healing and Treatments
Introduction and background
Diaper dermatitis (DD) is a broad term used to describe the acute inflammatory skin response caused by irritation from urine, feces, moisture, or friction in the diaper area of infants and children. It is also known as diaper rash, nappy rash, or irritant nappy dermatitis and typically occurs at least once during diaper usage [1-4]. This condition affects between 7% and 35% of infants, although some studies report rates as high as 50% at some point, leading to significant discomfort, distress, and disrupted sleep, which can be distressing for both the infant and the caregiver [5]. The prevalence of DD varies significantly across different countries: it ranges from 10% to 20% in the USA [6], 36% in Thailand [7], 14.9% in Germany [8], 1.3%-43.8% in China [9], 67% in Turkey [10], 38.9% in Nigeria [11], and 25% in Japan [12].
The rash seen in DD has multiple causes, stemming from the skin’s response to various systemic and local factors. When diapers are used, the skin’s alkalinity and moisture levels increase significantly. Prolonged exposure to moisture can lead to skin maceration, weakening the stratum corneum’s physical integrity and making it more susceptible to friction from the diaper’s surface. This prolonged moisture also increases the likelihood of developing additional skin damage and other issues due to exposure to irritants, especially urine and fecal lipases and proteases, which are known to be significant contributors to the development of DD [13-15].
Furthermore, frequent skin cleansing accelerates the loss of surface lipids and epidermal cells, disrupting the skin’s acid mantle and compromising its barrier function. Children who experience diarrhea, undergo ostomy takedown, or undergo colon surgery typically exhibit faster gastrointestinal transit, leading to the increased activity of fecal proteases and lipases. Consequently, these children are at a considerably higher risk of developing severe DD [13,14,16].
To address these challenges, the primary focus of management strategies for DD is to minimize inflammation and promote healing, a reassurance for caregivers and healthcare professionals [14,16]. Barrier preparations, such as topical ointments, creams, or pastes, aim to create a physical barrier on the skin’s surface. They have become a cornerstone in treating and preventing this common condition. In the context of DD, these products are designed to protect the skin from irritants such as urine, feces, and diaper friction. Common ingredients in barrier treatments include petrolatum, dimethicone, and zinc oxide (ZnO), each offering unique qualities that reduce friction, decrease irritation, and maintain skin hydration [17,18].
The introduction of disposable diapers, such as Pampers, in 1963 revolutionized diapering practices. Although disposable diapers are widely used (estimated at 80%-90% in affluent nations), they have not eliminated diaper rash [1,19]. Advancements, such as topical barrier creams and superabsorbent fabrics, aim to reduce the frequency and severity of diaper rash. Despite their widespread use, the current understanding of the therapeutic effectiveness of barrier preparations remains limited. Variations in methodology, techniques for applying barrier preparations, and outcome measures make it challenging to draw definitive conclusions about their overall efficacy.
Barrier product selection is often driven more by marketing claims than actual efficacy [20]. This highlights the importance for medical professionals, particularly those working with children, to stay up-to-date on the latest findings on over-the-counter (OTC) barrier therapies for DD. Through a comprehensive and quantitatively synthesized analysis of recent research on barrier preparations in DD, this systematic review and meta-analysis aims to address these limitations. They also strive to bridge knowledge gaps and provide caregivers and healthcare professionals with valuable evidence-based information. The results offer clarity on the role of barrier preparations in treating DD, which can inform therapeutic approaches. Ultimately, a deeper understanding of their efficacy can lead to improved therapy outcomes and better health for infants with this common condition.
Review
Materials and methods
The recent systematic review adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to ensure comprehensive reporting and methodological adherence [21].
Search Strategy
The meta-analysis and systematic review focused on the clinical effectiveness of barrier preparations in managing diaper rash, also known as diaper dermatitis. Relevant research papers were identified using electronic databases, including Medical Literature Analysis and Retrieval System Online (MEDLINE) via PubMed, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar, for data extraction. To ensure data authenticity, MeSH keywords such as “Diaper Dermatitis,” “Diaper Rash,” “Nappy Rash,” “Infant Skin Diseases,” “Irritant Dermatitis,” “Zinc Oxide,” and “Petroleum Jelly or Ointment” were used. The research timeline spanned from January 2004 to January 2024, gathering data from the past 20 years.
Eligibility Criteria
Inclusion criteria: Following the search across the mentioned electronic databases, our research team utilized predefined eligibility criteria to screen research articles for inclusion in the recent meta-analysis and systematic review. Specifically, we selected articles that met the following criteria: 1) addressed management strategies or barrier preparations; 2) involved a study population comprising infants and toddlers aged 0-2 years; 3) discussed nappy rash, diaper dermatitis, or diaper rash; 4) were based on randomized controlled trials (RCTs), quasi-randomized control studies, or cohort studies; and 5) were published in English with full-text availability [22].
Exclusion criteria: Excluded studies exhibited the following characteristics: 1) focused on management strategies for different types of rashes; 2) addressed populations outside the age range of 0-2 years old; 3) encompassed populations without diaper dermatitis or nappy rash; 4) were systematic reviews, meta-analyses, literature reviews, observational studies, scoping reviews, conference papers, or letters; and 5) were published in languages other than English (such as Chinese, Arabic, Spanish, and German) or were duplicate publications/non-full-text papers.
Data Extraction and Efficacy Measures
Data entry and processing were conducted using a standardized Excel sheet (Microsoft Corp., Redmond, WA), with two reviewers responsible for extracting data from the included studies. The extracted data encompassed several domains, including study years, the country of origin, study follow-up duration, sample sizes, types of barrier preparations used for management, and primary outcomes from the selected articles. The reviewers independently extracted data from the articles included, resolving any discrepancies through discussion.
Types of Intervention and Primary Outcomes
The recent systematic review and meta-analysis identified significant barrier types for managing diaper dermatitis among infants: soap and water, zinc oxide paste, petroleum jelly (Vaseline), lanolin, and hydrozole ointment [22]. The primary outcomes of the meta-analysis included preventing nappy dermatitis, the number of infants showing a decrease in nappy dermatitis severity, and the reduction in nappy dermatitis duration (measured in days). The severity of the rash was assessed using the following scale: severe (skin breakdown), mild/moderate (any rash present), and absent (no rash).
Risk of Bias Assessment
To assess the risk of bias in the included RCTs, we employed the Cochrane risk of bias assessment tool, which evaluates bias across seven domains: (a) allocation concealment, (b) selection bias or random sequence generation, (c) performance bias or blinding of participants and personnel, (d) detection bias or blinding of outcome assessment, (e) selective bias or selective reporting, and other biases [23]. Each domain’s score was categorized as low risk, high risk, or unclear.
For other cohort studies, we used the Joanna Briggs Institute (JBI) critical appraisal checklist to assess the methodological quality of the included prospective cohort studies. Additionally, we evaluated the methodological quality of included cross-sectional studies and the strategies they employed to address and minimize bias using the JBI critical assessment instrument [24].
Statistical Analysis
The statistical analysis of data from studies included in the recent meta-analysis and systematic review was conducted using RevMan 5.3 software (The Cochrane Collaboration, London, United Kingdom) [21]. A p-value of <0.05 was considered statistically significant when presenting results as odds ratios (ORs) with 95% confidence intervals (CIs). Additionally, heterogeneity was assessed using the Q test and I^2^ statistics. A fixed effects model was used when no significant heterogeneity was detected, while a random effects model was applied otherwise.
Results
Included Studies
The selection and screening of research papers on the clinical effectiveness of barrier preparations for managing diaper dermatitis were conducted according to the PRISMA guidelines in the recent meta-analysis. Initially, 154 research articles were identified from three electronic databases using the specified search strategy. Fifty-four articles were removed due to duplicate records or ineligibility, and 11 articles could not be retrieved. Following the PRISMA guidelines, 89 papers were then screened, and six research articles were included after applying the exclusion criteria (Figure 1) [24].
Screening and selection of the included studies by PRISMA guidelinesResearch articles were retrieved from the following databases: MEDLINE via PubMed, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar, including randomized controlled trials, quasi-randomized controlled studies, and cohort studiesPRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; MEDLINE, Medical Literature Analysis and Retrieval System Online*
Risk of Bias Assessment
Out of the six studies included, four were randomized controlled trials evaluated using the Cochrane Library tool. Among these, three out of four were deemed to have low to moderate risk [25-27], while one study was classified as high risk [28], as illustrated in Figure 2 and Figure 3. The remaining two studies were cohort studies, and their methodological quality assessment was conducted using the JBI criteria (Table 1) [29,30].
Risk bias of the included studies
Visual representation of risk bias summary for the included studiesData adapted from Alonso et al. [25], Yonezawa et al. [26], Garcia Bartels et al. [27], and Hoeger et al. [28]
Characteristics of the Included Studies
The articles included in the recent systematic review and meta-analysis were published between 2004 and 2024. All included trials were randomized controlled trials. To produce heterogeneity of results, the trials belong to five different countries: two in Germany [26,27], one in Spain [25], one in Japan [26], one in Thailand [29], and one in Mexico [30]. Table 2 provides detailed characteristics of the included studies.
Infants With Reduced Symptoms
Among the six included studies, approximately four examined the decrease in dermatitis incidence rates in both the experimental and placebo groups [25-28]. A significant difference in the prevalence of dermatitis was noted between the intervention and placebo groups (odds ratio = 0.77; CI = 0.37-1.61; p = 0.0002), and heterogeneity was observed (degrees of freedom {df} = 3; I^2^ = 79%), as illustrated in Figure 4 and Figure 5.
Forest plot of the incidence of dermatitis among the experimental and placebo groupsData adapted from Alonso et al. [25], Yonezawa et al. [26], Garcia Bartels et al. [27], Hoeger et al. [28], Chaithirayanon et al. [29], and Bonifaz et al. [30]CI, confidence interval; df, degrees of freedom
The funnel plot of the incidence of dermatitis among the experimental and placebo groupsSE, standard error; OR, odds ratio
Prevention of Diaper Dermatitis
Among the six included studies, clotrimazole emerged as an effective management strategy, with a lower incidence of dermatitis compared to placebo [27,28,30]. Additionally, zinc oxide paste demonstrated effectiveness in managing diaper dermatitis among neonates or infants. Regarding prevention strategies, the use of diaper cream or moisturizers, along with soap, proved effective in controlling the incidence of nappy rash [28,29]. However, only one study reported no efficacy of petroleum jelly or Vaseline in reducing the severity and incidence of dermatitis symptoms [25].
Discussion
Diaper dermatitis (DD) remains a widespread concern for children and caregivers globally. Since its initial documented description in 1877, numerous studies have been undertaken to elucidate the condition’s causes, the most efficacious treatment approaches, and methods to prevent exacerbation. This systematic study aimed to comprehensively assess over-the-counter (OTC) barrier treatments for DD. By meticulously reviewing the literature, we aimed to furnish valuable insights to healthcare providers and families. DD’s peak incidence typically falls between nine and 12 months, making it one of early childhood’s most prevalent dermatological disorders, with an incidence ranging from 7% to 35% [1,19]. Consequently, it remains a concern shared by both caregivers and healthcare professionals. This concern has spurred a substantial industry, as evidenced by the array of products available for DD treatment and/or prevention, the multitude of online platforms dedicated to the topic, and the frequency of medical consultations [31].
Numerous products claim to protect the skin from damage caused by exposure to urine and feces. Compared to placebo, the meta-analysis showed a moderate reduction in DD incidence. However, significant variability was observed, suggesting that efficacy may vary depending on the barrier preparation and study methodology. The investigations explored a range of barrier preparations, including clotrimazole, petroleum jelly, water and soap, zinc oxide paste, and nappy creams/moisturizers [25-30].
Experts recommend barrier creams containing petrolatum or zinc oxide for their ability to protect the skin from moisture and potentially reduce the severity of DD [32]. In our studies, Hoeger et al. [28] found that zinc oxide (ZnO) paste was less effective than clotrimazole, whereas another study reported quicker recovery times than with talcum powder [29]. However, methodological quality assessment revealed missing critical information, raising the potential for bias in the findings. It is unclear whether this resulted from inadequate reporting rather than poor design, so conclusions are supported by low-level evidence (grade C), which urges caution in implementation [28]. In a separate study, the 2% eosin group showed significantly higher rates of full and partial healing compared to a corticosteroid and ZnO paste. ZnO paste also promoted healing, with 22% achieving complete healing and 44% partial healing [33].
The potential preventive effects of water and soap on DD have not been definitively demonstrated in published research, although a Japanese study concluded that their practical use improves DD [26]. There is insufficient evidence to suggest that these practices have a positive impact on the physiological skin parameters necessary for maintaining healthy skin in the diaper area. Antifungal medications such as nystatin and clotrimazole are recommended when candidal infections exacerbate the irritation of dermatitis [34]. Clotrimazole, in particular, emerged as an effective treatment for DD across multiple studies, with minimal incidence rates compared to placebo. This suggests that clotrimazole may be a beneficial treatment option, especially when fungal colonization is suspected [27,28,30]. Hoeger et al. compared the safety and effectiveness of two distinct antifungal pastes in infants with DD, finding that clotrimazole was more effective [28]. Bonifaz et al. indicated that DD candidiasis might be effectively treated with 2% tetraconazole cream, indirectly supporting the utility of antifungal medications in DD management [30]. Garcia Bartels et al. investigated how wet wipes and diaper cream affected an infant’s skin barrier, revealing that clotrimazole was superior to clothing or wet wipes for managing DD [27]. These studies, with lower dermatitis incidence rates than placebo, suggest that clotrimazole is an effective therapeutic strategy for DD.
Nearly 20 years have passed since Gupta and Bluhm investigated the regular use of petroleum-based barrier cream at each diaper change to prevent DD in high-risk children [35]. Their findings suggested that if the skin in the diaper area remained intact during cream application, using a petroleum-based cream was beneficial for preventing DD. However, more extensive controlled studies are needed due to the study’s limited sample size and the persistent issue of DD in this high-risk group. The inability to conduct a meta-analysis, even within the general newborn population, was due to differences in study design, resulting in narrowly focused conclusions. Similarly, a study from Spain found no significant advantage of petroleum jelly (Vaseline) in reducing the frequency or intensity of DD symptoms, challenging the widespread belief in its prophylactic role [25]. Further investigation is needed to determine the exact role of petroleum jelly in the treatment of DD.
Despite these findings, several limitations exist. The review may have overlooked crucial information from alternative study designs, such as cohort studies, as it primarily focused on RCTs, which are considered the gold standard of evidence. Moreover, the observed heterogeneity highlights the need for further investigation into the variables that influence the efficacy of barrier preparations. While the review identified potential benefits of ZnO and clotrimazole, the effectiveness of other barrier preparations, such as natural or organic alternatives, remains unknown. More research is necessary to determine the optimal application frequency and duration for various barrier preparations. The severity of DD may also impact the effectiveness of barrier preparations, and individual differences in skin type and potential allergies to the components of barrier treatments must be taken into account. Exploring how barrier preparations interact with regular diaper changes, hygiene practices, or other topical treatments may provide valuable insights.
Conclusions
This systematic review concluded that barrier preparations are effective in managing diaper dermatitis in infants. While the analysis indicated a moderate overall effect compared to placebo, there were notable variations across studies. Clotrimazole was identified as a promising barrier treatment for diaper dermatitis, particularly in suspected fungal infections. Although zinc oxide paste showed potential for treating diaper dermatitis, further research is needed to determine its optimal application. Petroleum jelly appeared to provide no significant benefits. Future investigations should include cost-effectiveness assessments and consider integrating barrier methods with other management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diaper dermatitis and associated factors among 1-24 months children visiting public health facilities of Arba Minch town, Gamo zone, southern Ethiopia Heliyon Bante A Girma M Ahmed M Aschalew Z 09202310.1016/j.heliyon.2023.e 20785 PMC 1058239437860555 · doi ↗ · pubmed ↗
- 2Diagnosis and management of diaper dermatitis Pediatr Clin North Am Shin HT 3673826120142463665110.1016/j.pcl.2013.11.009 · doi ↗ · pubmed ↗
- 3Diaper (napkin) dermatitis: a fold (intertriginous) dermatosis Clin Dermatol Tüzün Y Wolf R Bağlam S Engin B 4774823320152605106510.1016/j.clindermatol.2015.04.012 · doi ↗ · pubmed ↗
- 4Newborn infant skin: physiology, development, and care Clin Dermatol Visscher MO Adam R Brink S Odio M 2712803320152588912710.1016/j.clindermatol.2014.12.003 · doi ↗ · pubmed ↗
- 5A review study of diaper rash dermatitis treatments J Client-Centered Nurs Care Sharifi-Heris Z Amiri Farahani L Hasanpoor-Azghadi SB 11242018
- 6Prevention, treatment and parent education for diaper dermatitis Nurs Womens Health Merrill L 3243361920152626479710.1111/1751-486X.12218 · doi ↗ · pubmed ↗
- 7Diaper dermatitis: a survey of risk factors in Thai children aged under 24 months BMC Dermatol Sukhneewat C Chaiyarit J Techasatian L 71920193126228810.1186/s 12895-019-0089-1PMC 6604136 · doi ↗ · pubmed ↗
- 8Diaper dermatitis prevalence and severity: global perspective on the impact of caregiver behavior Pediatr Dermatol Carr AN De Witt T Cork MJ 1301363720203179309010.1111/pde.14047 PMC 7027557 · doi ↗ · pubmed ↗