Effects of Antibiotic Stewardship Program on Antibiotic Consumption and the Incidence of Clostridioides difficile Infection
Joung Ha Park, Juhee Kim, Juyeon Lee, Hyemin Chung, Min-Chul Kim

TL;DR
An antibiotic stewardship program in South Korea reduced antibiotic use and slowed the rise of Clostridioides difficile infections over a year.
Contribution
This study demonstrates the impact of an ASP on antibiotic consumption and C. difficile infection trends in a hospital setting.
Findings
Antibiotic use increased pre-ASP but decreased significantly post-ASP implementation.
C. difficile infection incidence showed a slower upward trend after ASP introduction.
Each additional antibiotic day of therapy correlated with a small increase in C. difficile cases after a 4-week lag.
Abstract
Background/Objectives: Growing concerns about antibiotic-associated adverse events, including Clostridioides difficile infection, prompted implementation of an antibiotic stewardship program (ASP) in South Korea in November 2024. One year post-implementation, we evaluated changes in antibiotic consumption and C. difficile infection incidence. Methods: This study was conducted at Chung-Ang University Gwangmyeong Hospital, South Korea. Segmented regression and interrupted time series analyses were performed using weekly data on antibiotic use (days of therapy [DOT] per 1000 patient-days) and C. difficile infection or colonization (cases per 1000 patient-days) over 157 weeks (November 2022–October 2025). Weeks 1–105 defined the pre-ASP period, and weeks 106–157 the post-ASP period. A 4-week lag between antibiotic use and subsequent C. difficile infection was hypothesized. Results: Before…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
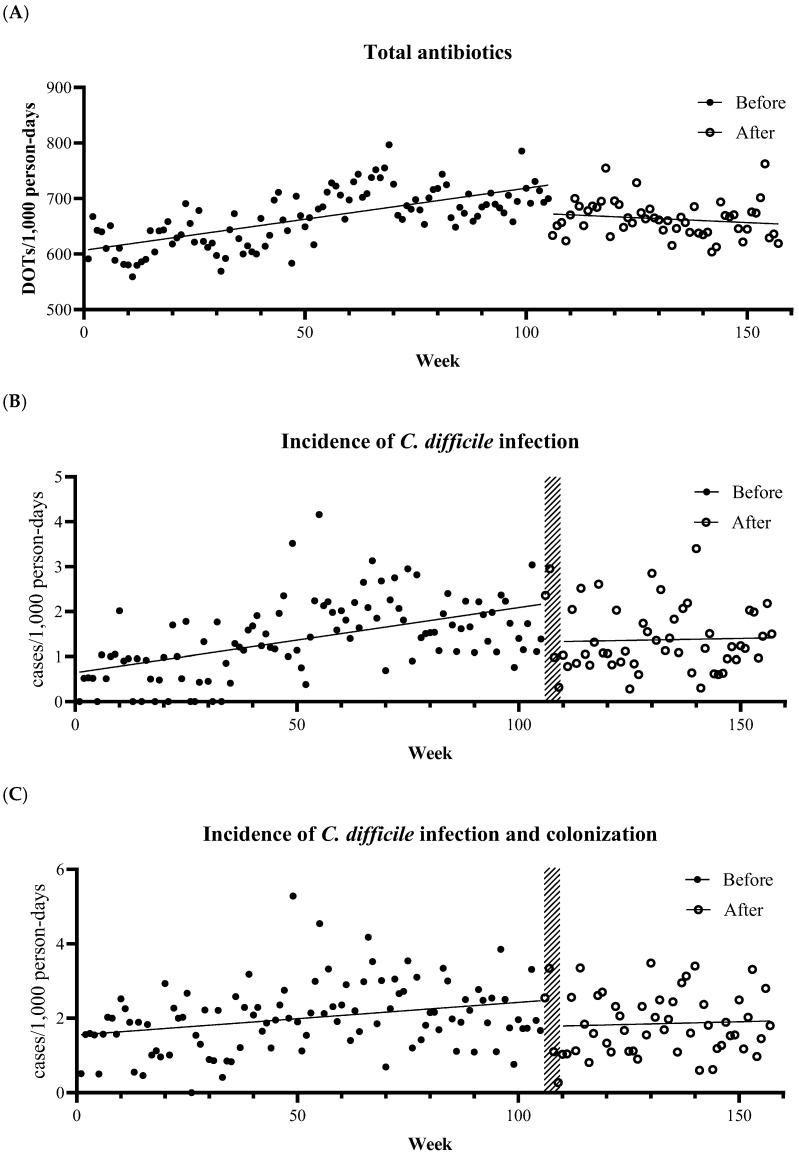 Figure 1
Figure 1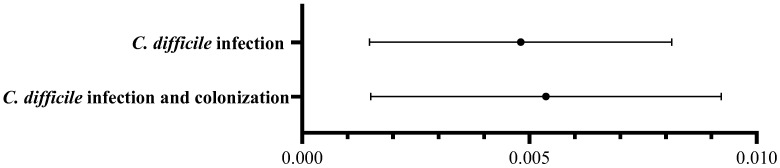 Figure 2
Figure 2- —Chung-Ang University Research Grants
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Clostridium difficile and Clostridium perfringens research · Antibiotic Resistance in Bacteria
1. Introduction
Clostridioides difficile infection is a major cause of healthcare-associated diarrhea and can range from mild disease to life-threatening complications. According to recent data from the Health Insurance Review and Assessment Service in South Korea, the incidence of C. difficile infection increased from 1.0 to 5.1 per 10,000 patient-days in tertiary hospitals and from 0.6 to 5.0 per 10,000 patient-days in general hospitals over a 13-year period (from 2008 to 2020), with similar global trends reported [1,2,3]. As C. difficile infection can be transmitted to other patients through both direct and indirect contact, implementing infection control strategies, including contact precautions and hand hygiene, is essential for preventing disease transmission in healthcare settings. In addition, antibiotic consumption is a well-established risk factor for C. difficile infection because antibiotics can alter the gut microbiota, which mediates colonization resistance against C. difficile [4,5]. Therefore, minimizing unnecessary antibiotic use is a key strategy for preventing C. difficile infections.
Growing concerns about the adverse effects of antibiotics, such as C. difficile infection and the emergence of multidrug-resistant organisms (MDRO), have prompted the worldwide adoption of antimicrobial stewardship programs (ASP). Since 2014, the US Centers for Disease Control and Prevention (CDC) has released core elements of hospital antibiotic stewardship programs to optimize antibiotic use [6]. In general, strategies to improve antibiotic prescribing are categorized into restriction (pre-prescription approval) and enablement interventions (education, post-prescription feedback, and audits) [7,8]. At our center, which opened in March 2022, we controlled the use of broad-spectrum antibiotics, such as carbapenems, through a policy requiring preauthorization for their prescription. To reflect global trends, South Korea launched a nationwide ASP pilot program in November 2024 to reinforce antibiotic stewardship. One year after ASP implementation in our center, we aimed to evaluate changes in both antibiotic consumption and C. difficile infection incidence before and after ASP introduction. Furthermore, using an interrupted time-series analysis of real-world data, we assessed the impact of changes in antibiotic use on the incidence of C. difficile infection.
2. Results
2.1. Effect of ASP on Antibiotic Consumption
Over 157 weeks, the total antibiotic use (days of therapy [DOT] per 1000 patient-days) showed a segmented trend around ASP initiation (week 106) (Table S1 and Figure 1A). Before ASP, weekly total antibiotic use increased (β1 = 1.14, 95% CI 0.76 to 1.51, p < 0.001). After ASP implementation, the change in slope was negative (β3 = −1.50, 95% CI −3.62 to −0.39, p = 0.009). In segmented regression, the post-ASP slope equals the sum of the pre-ASP slope (β1) and the slope change after ASP (β3). Based on the above estimates, the post-ASP slope is β1 + β3 = −0.36 DOT per 1000 patient-days. The class-specific consumption results were consistent for penicillins, anti-pseudomonal penicillins and cephalosporins, and fluoroquinolones (Table S2 and Figure S1). In contrast, cephalosporin use did not change significantly during the pre-ASP period but increased in the post-ASP period. The use of carbapenems and glycopeptides did not change significantly in either the pre- or post-ASP periods.
2.2. Incidence of C. difficile Infection and Colonization
Patients with C. difficile infection or colonization had a median age of 69 years (interquartile range, 53–81). To account for a biologically plausible delay after ASP implementation, weeks 106–109 were excluded as wash-in periods. These observations were plotted as points but were excluded from trend fitting (Figure 1B,C), and the post-ASP segment was fitted from week 110 onward. While pre-ASP C. difficile infection incidence increased (α_1_ = 0.01, 95% CI 0.01 to 0.02, p < 0.001), the change in slope after ASP was not significant (α_3_ = −0.01, 95% CI −0.03 to 0.004, p = 0.13) (Table S3A and Figure 1B). The trends in C. difficile infection and colonization incidence were similar (Table S3B and Figure 1C).
2.3. Lagged Effect of Antibiotic Use on C. difficile Infection
After additional analysis of the total effect of antibiotic use on C. difficile infection occurrence with 1-, 2-, 4-, and 8-week lags, we selected a 4-week lag for the primary analysis. In the primary ITS exposure–response model with a 4-week lag for antibiotic use, we analyzed the relationship between antibiotic use (DOT per 1000 patient-days) 4 weeks earlier and subsequent C. difficile infection and colonization after adjusting for calendar time. C. difficile infection incidence increased by 0.005 cases per 1000 patient-days with an increase of 1 DOT per 1000 patient-days of total antibiotics 4 weeks earlier. C. difficile infection and colonization incidence also increased by 0.005 cases per 1000 patient-days with an increase of 1 DOT per 1000 patient-days in total antibiotics (Figure 2).
2.4. Sensitivity Analysis—Antibiotic Class-Specific Effects on C. difficile Infection Occurrence at Fixed Total Antibiotic Use
We performed a sensitivity analysis to estimate the compositional effect, in which an increase of 1 DOT in a given antibiotic class was interpreted as displacing 1 DOT from the remaining classes while holding the total DOT constant. When total antibiotic use was held constant, an additional 1 DOT per 1000 patient-days of fluoroquinolone use was associated with 0.02 more cases of C. difficile infection and colonization per 1000 patient-days (Figure S2). However, the association between fluoroquinolone use and C. difficile infection incidence was not statistically significant. In contrast, an additional 1 DOT per 1000 patient-days of cephalosporin use was associated with 0.008 fewer cases of C. difficile infection per 1000 patient-days and 0.01 fewer cases of C. difficile infection and colonization per 1000 patient-days. Similarly, glycopeptide use was associated with 0.02 fewer cases of C. difficile infection and colonization per 1000 patient-days per 1 DOT increase. The other classes did not show significant associations with C. difficile infection or colonization.
3. Discussion
3.1. Main Findings
In this single-center ITS analysis conducted over 157 consecutive weeks, we identified three main findings. First, total antibiotic consumption decreased following ASP implementation compared to the pre-ASP period, which relied on restriction strategies. In particular, the use of anti-pseudomonal penicillins and cephalosporins, and fluoroquinolones markedly declined after the intervention. Second, although the incidence of C. difficile infection steadily increased before ASP implementation, this upward trend was attenuated after the intervention; however, the change in slope did not reach statistical significance. The incidence of C. difficile infection and colonization was similar. Third, the exposure–response model demonstrated a lagged association between antibiotic use and C. difficile infection occurrence. The incidence of C. difficile infection increased by 0.005 cases per 1000 patient-days for every 1 DOT per 1000 patient-days increase in total antibiotic consumption four weeks earlier.
3.2. Interpretation
We demonstrated that ASP implementation was associated with decreased total antibiotic consumption, showing an immediate decline at the time of implementation, followed by a significantly decreased slope thereafter. A previous systematic review also reported an approximately 10% decrease in antibiotic prescriptions following ASP implementation, consistent with our findings [9]. The marked immediate decline at the time of implementation was likely attributable to heightened institutional awareness and vigilance among prescribing physicians. We also evaluated antibiotic class-specific changes after ASP implementation. The use of carbapenems and glycopeptides did not change significantly in the post-ASP period. It is likely that broad-spectrum antibiotics, such as carbapenems and glycopeptides, were already controlled by pre-existing restriction strategies. Our center participated in the Korea National Antimicrobial Use Analysis System (KONAS) in November 2024 and reported quarterly carbapenem consumption. According to the KONAS report, carbapenem use was already lower (39.6 DOT per 1000 patient-days) than that of other hospitals of similar size (61.1 DOT per 1000 patient-days), even before ASP implementation. These findings suggest that pre-existing restriction strategies effectively limit the use of targeted antibiotics, including carbapenems. Therefore, further reductions in carbapenem use after ASP implementation may have been inherently limited. Previous studies have shown that restriction strategies markedly reduce targeted antibiotic use [10,11], whereas discontinuation of these strategies could lead to a return to prior patterns of antibiotic consumption [12]. However, these restriction strategies may not affect the use of other antibiotics and may even lead to a balloon effect [13]. Given this limitation, we endorsed reinforced ASP policies in November 2024. Consequently, the use of anti-pseudomonal penicillins and cephalosporins, and fluoroquinolones markedly decreased. The increased use of total cephalosporins may be explained by the substitution effect following de-escalation strategies using narrow-spectrum cephalosporins such as cefazolin or ceftriaxone, which is consistent with the goals of ASP [14]. Unlike previous restriction strategies that relied on prescription request forms for restricted antibiotics, the newly implemented ASP adopted more active approaches by monitoring all antibiotic use daily and providing repeated education and prompt feedback on inappropriate prescriptions to prescribing physicians. This proactive ASP approach appears to be effective in reducing unnecessary antibiotic use.
Antibiotic exposure is a well-known risk factor for C. difficile infection, and a time lag between antibiotic use and subsequent C. difficile infection is commonly observed [4,15,16]. The time-lag period aligns with the incubation period for C. difficile infection and the time required for antibiotic-induced dysbiosis to facilitate spore germination and toxin production in the gut, supporting the biological plausibility [5]. Thus, in this study, C. difficile infection incidence was analyzed considering a 4-week lag effect following antibiotic consumption. In this model, C. difficile infection incidence increased by 0.005 cases per 1000 patient-days for every 1 DOT per 1000 patient-days increase in antibiotic use. This finding is consistent with those of previous studies showing positive correlations between antibiotic use and C. difficile infection incidence [17,18,19]. Previous systematic reviews have identified a 32–52% reduction in C. difficile infection after ASP implementation [17,18]. In addition, a cross-sectional analysis demonstrated a 4.4% increase in hospital-onset C. difficile infection every 50 DOT per 1000 patient-day increase in total antibiotic use [19]. Although some studies reported that C. difficile infection incidence did not decline despite reductions in antibiotic consumption [20,21], the effect size observed in our study—an additional 0.25 cases per 1000 patient-days for every 50 DOT increase per 1000 patient-days—supports the notion that reducing antibiotic consumption through ASP meaningfully contributes to lowering C. difficile infection incidence. However, C. difficile infection is influenced not only by antibiotic consumption but also by other factors, including diagnostic testing strategies, infection control measures, and patients’ clinical characteristics [22]. As we could not analyze the effects of these confounding factors on C. difficile infection, the observed change in incidence cannot be attributed solely to reductions in antibiotic use.
Several previous studies have identified specific antibiotic classes that are more likely to induce C. difficile infection, particularly second- and third-generation cephalosporins, fluoroquinolones, and clindamycin [22,23]. In the present study, although the independent effect of each antibiotic class on C. difficile infection incidence could not be demonstrated, we assessed the relative effect of class-specific antibiotic use under the assumption that total antibiotic consumption remained constant. In this context, an increase of 1 DOT in a specific class implies a corresponding decrease of 1 DOT in the other classes. Similarly to previous studies, an increase of 1 DOT of fluoroquinolones, a well-known high-risk class [22,24], significantly increased the incidence of C. difficile infection and colonization in our analysis. In contrast, the increased use of cephalosporins and glycopeptides was associated with a decrease in C. difficile infection incidence. This finding differs from that of a previous study, which classified second- and third-generation cephalosporins as high-risk antibiotics for C. difficile infection [24]. These discrepancies may be attributed to the fact that this study was unable to independently evaluate the inherent effects of each antibiotic class.
3.3. Limitations of the Study
This study had some limitations. First, the study was performed at a single center. As the hospital is a recently established institution in its fourth year of operation, the generalizability of the findings may be limited. However, studies involving large populations and multiple institutions often introduce substantial heterogeneity and confounding factors. The results of this study nonetheless provide meaningful insights. Second, although C. difficile infection can be influenced by various factors, such as proton-pump inhibitor use, length of hospital stay, and underlying diseases, we did not adjust for these potential confounders and focused on antibiotic consumption. Moreover, infection control measures (e.g., hand hygiene compliance and isolation protocols) were not considered, although the hospital’s infection control policy against C. difficile infection remained consistent throughout the study period. Further studies are required to evaluate the effects of these variables on C. difficile infection using multivariable ITS analyses. Third, we assessed antibiotic exposure solely using DOT and did not evaluate the defined daily dose (DDD). Because DOT does not reflect prescribed doses, we could not examine dose-dependent associations between antibiotic exposure and C. difficile infection. Finally, we did not consider the clinical severity of C. difficile infection, which may provide additional insights into the association between antibiotic consumption and clinical outcomes. In addition, as strain-specific virulence (e.g., ribotype 027) and antibiotic resistance data were available, we were unable to evaluate their contribution to the observed association between antibiotic consumption and C. difficile infection and colonization.
3.4. Conclusions
In conclusion, proactive ASP strategies were effective in significantly decreasing overall antibiotic consumption. Notably, the use of anti-pseudomonal penicillins and cephalosporins, and fluoroquinolones—which were not adequately controlled under previous restriction strategies—showed a substantial decline. Furthermore, this reduction in antibiotic consumption led to a decrease in the incidence of C. difficile infection or colonization. These findings highlight the importance of proactive ASP strategies in clinical practice. Further studies with longer follow-up periods are warranted to assess the sustainability of these results and evaluate additional factors that may influence C. difficile infection occurrence.
4. Materials and Methods
4.1. Study Design
This study was conducted at Chung-Ang University Gwangmyeong Hospital in Gyeonggi-do, Republic of Korea. Our center opened in March 2022. Since then, we have limited the prescription of broad-spectrum antibiotics, including ceftazidime-avibactam, ceftolozane-tazobactam, carbapenems, glycopeptides, colistin, daptomycin, linezolid, and tigecycline, to 3 days without approval from infectious disease specialists. In addition, clinicians discuss infectious disease cases in formal consultations with infectious disease specialists. After implementing the nationwide ASP pilot program in November 2024, we adopted a reinforced ASP policy, as described in Table 1. We performed segmented regression and interrupted time-series (ITS) analyses using weekly data on antibiotic use and cases of C. difficile infection and colonization over 157 consecutive weeks from November 2022 to October 2025 (weeks 1–157). We defined the pre-ASP period as weeks 1–105, and the post-ASP period as weeks 106–157. This study was approved by the Institutional Review Board of our center. The requirement for written informed consent was waived due to the retrospective nature of the study.
4.2. Definition
All antibiotics were monitored daily and are listed in Table S4. We included all antibiotics used in our hospital except oral vancomycin, as this drug is specifically administered for the treatment of C. difficile infections. Fidaxomicin, which is a treatment of choice of C. difficile infection, was not included in the analysis because it was not available in South Korea during the study period. We also analyzed the DOT according to antibiotic class, including penicillins, cephalosporins, carbapenems, glycopeptides, and fluoroquinolones. The anti-pseudomonal penicillins and cephalosporins included piperacillin-tazobactam, ceftazidime, and cefepime. DOT was defined as the number of days for which a patient received any specific antibiotic. Any amount of agent administered on a given day was counted as one DOT. C. difficile infection was defined as the presence of clinical symptoms (loose stool or diarrhea) and positive results for C. difficile toxin polymerase chain reaction (PCR) or enzyme immunoassay (EIA). C. difficile colonization was defined as cases with negative results for C. difficile toxin PCR and EIA and a positive result for C. difficile culture, since culture at our center identifies both toxigenic and non-toxigenic strains.
4.3. Outcomes
We described the weekly use of total antibiotics, quantified as DOT per 1000 patient-days, during the pre- and post-ASP periods. We also examined the antibiotic class-specific DOT per 1000 patient-days, including penicillins, cephalosporins, anti-pseudomonal penicillins and cephalosporins, carbapenems, fluoroquinolones, and glycopeptides. We analyzed the weekly incidence of C. difficile infection and colonization, described as cases per 1000 patient-days. We excluded weeks 106–109 from the analysis of the weekly incidence of C. difficile infection and colonization because this period is considered a wash-in period. Furthermore, we analyzed the impact of changes in DOT per 1000 patient-days on changes in C. difficile infection and colonization with a 4-week lag.
4.4. Statistical Analysis
We performed a segmented regression analysis of the ITS to assess weekly observations over 157 consecutive weeks, aiming to evaluate changes associated with ASP implementation and quantify the lagged association between antibiotic use and C. difficile infection and colonization [25,26]. Week 106 was the first post-ASP week (the ASP was implemented immediately after week 105).
4.4.1. Time Variables
Let t = 1, …, 157 index weeks and define:
- timet = t.
- Post-ASP from week 106: interv106t = 1 (t ≥ 106) and post106t = max (0, t − 105).
- For wash-in handling when modeling C. difficile infection and colonization trends from week 110: interv110t = 1 (t ≥ 110) and post110t = max (0, t − 109).
- Lagged exposure for the exposure–response models: DOTt−4 (4-week lag).
4.4.2. Effect of ASP on Antibiotic Consumption
To estimate the changes in the level and slope of antibiotic consumption following ASP implementation, we fit the model as follows:
where β1 denotes the pre-ASP slope, β2 the immediate level change at week 106, and β3 the change in slope after ASP (post-ASP slope = β1 + β3). The same specifications were applied to the class-specific DOT for descriptive inference.
4.4.3. Incidence of C. difficile Infection and Colonization
To describe ASP-associated changes in C. difficile infection, we applied a 4-week wash-in immediately after ASP initiation and excluded outcome weeks 106–109. We considered that this period might have been affected by the DOT during the pre-ASP period. Thus, C. difficile infection trends were modeled from week 110 onward using the following equation:
Fit on weeks t ≤ 105 or t ≥ 110. The incidence of C. difficile colonization was modeled using the same specifications.
4.4.4. Lagged Effect of Antibiotic Use on C. difficile Infection and Colonization
We hypothesized that antibiotic use could affect subsequent C. difficile infection with a 4-week lag [15,16]. To select an optimal single-lag exposure–response structure, ITS models incorporating lag periods of 1, 2, 4, and 8 weeks were compared using maximum likelihood estimation and the Akaike and Bayesian information criteria (AIC/BIC). The lag minimizing both criteria was selected and refitted using the restricted maximum likelihood (REML) for inference. To quantify the relationship between antibiotic use and subsequent C. difficile infections, we modeled the following:
Using all weeks with defined lagged exposure (i.e., t ≥ 5). The coefficient γ4 represents the absolute change in C. difficile infection incidence (cases per 1000 patient-days) associated with a 1-unit increase in total antibiotic use (DOT per 1000 patient-days) 4 weeks earlier, adjusted for underlying time trends and ASP phase. Changes in C. difficile colonization incidence were estimated using the same specifications.
4.4.5. Sensitivity Analysis: Antibiotic Class-Specific Effects on C. difficile Infection Occurrence at Fixed Total DOT
To evaluate the effect of antibiotic class-specific composition on subsequent C. difficile infections, we performed class-composition ITS modeling. The total DOT and one class-specific DOT, each lagged by 4 weeks, were entered concurrently in each model. For each antibiotic class k, the model was as follows:
where θ_k_ estimates the absolute change in C. difficile infection incidence (cases per 1000 patient-days) for a 1 DOT per 1000 patient-days increase in class k, holding total DOT constant. This represents a compositional effect, as the increased use of one class substitutes for others. The same approach was applied to C. difficile colonization incidence.
4.4.6. Error Structure and Estimation
All ITS models were estimated by generalized least squares (GLS) with first-order autoregressive errors to account for serial correlation in weekly residuals: ε_t_ = ϕε_t_−1 + u_t_ with u_t_~N(0, σ^2^). The models were fitted using REML. Regression coefficients were reported with two-sided p-values and 95% confidence intervals (CIs), and the AR(1) parameter ϕ was presented to quantify week-to-week residual correlation. Model adequacy was evaluated by inspecting normalized residuals (ACF/PACF) and applying the Durbin–Watson and Ljung–Box tests for residual autocorrelation. Models were excluded if the diagnostic results were unsatisfactory.
4.4.7. Software
Analyses were conducted using R software (version 4.5.1). Descriptive segmented lines were plotted using GraphPad Prism software (version 10.5.0). Plots were used for visualization only, whereas statistical inference was derived from the GLS ITS models.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Borren N.Z. Ghadermarzi S. Hutfless S. Ananthakrishnan A.N. The emergence of Clostridium difficile infection in Asia: A systematic review and meta-analysis of incidence and impact P Lo S ONE 201712 e 017679710.1371/journal.pone.017679728463987 PMC 5413003 · doi ↗ · pubmed ↗
- 2Kim J. Myung R. Kim B. Kim J. Kim T. Lee M.S. Kim U.J. Park D.W. Kim Y.S. Lee C.S. Incidence of Clostridioides difficile Infections in Republic of Korea: A Prospective Study With Active Surveillance vs. National Data From Health Insurance Review & Assessment Service J. Korean Med. Sci.202439 e 1183856517510.3346/jkms.2024.39.e 118PMC 10985502 · doi ↗ · pubmed ↗
- 3Marra A.R. Perencevich E.N. Nelson R.E. Samore M. Khader K. Chiang H.Y. Chorazy M.L. Herwaldt L.A. Diekema D.J. Kuxhausen M.F. Incidence and Outcomes Associated with Clostridium difficile Infections: A Systematic Review and Meta-analysis JAMA Netw. Open 20203 e 191759710.1001/jamanetworkopen.2019.1759731913488 PMC 6991241 · doi ↗ · pubmed ↗
- 4Britton R.A. Young V.B. Interaction between the intestinal microbiota and host in Clostridium difficile colonization resistance Trends Microbiol.20122031331910.1016/j.tim.2012.04.00122595318 PMC 3408078 · doi ↗ · pubmed ↗
- 5Peniche A.G. Savidge T.C. Dann S.M. Recent insights into Clostridium difficile pathogenesis Curr. Opin. Infect. Dis.20132644745310.1097/01.qco.0000433318.82618.c 623982235 · doi ↗ · pubmed ↗
- 6Centers for Disease Control and Prevention Core Elements of Hospital Antibiotic Stewardship Programs US Department of Health Human Services, C.D.C.Atlanta, GA, USA 2019
- 7Davey P. Marwick C.A. Scott C.L. Charani E. Mc Neil K. Brown E. Gould I.M. Ramsay C.R. Michie S. Interventions to improve antibiotic prescribing practices for hospital inpatients Cochrane Database Syst. Rev.20172 CD 00354310.1002/14651858.CD 003543.pub 428178770 PMC 6464541 · doi ↗ · pubmed ↗
- 8Yoon Y.K. Kwon K.T. Jeong S.J. Moon C. Kim B. Kiem S. Kim H.-S. Heo E. Kim S.-W. Guidelines on Implementing Antimicrobial Stewardship Programs in Korea Infect. Chemother.20215361765910.3947/ic.2021.009834623784 PMC 8511380 · doi ↗ · pubmed ↗