Antibiotic Resistance Pattern and Surgical Outcome in Complicated Intra-Abdominal Infections Due to Colorectal Perforation
Jacopo Giuliani, Camilla Cremonini, Serena Musetti, Giuseppe Zocco, Ismail Cengeli, Dario Tartaglia, Massimo Chiarugi, Alice Salamone, Ettore Melai, Francesco Forfori, Benedetta Tuvo, Iacopo Franconi, Antonella Lupetti, Lorenzo Ghiadoni, Federico Coccolini

TL;DR
This study examines antibiotic resistance and surgical outcomes in intra-abdominal infections caused by colorectal perforation, finding that resistant bacteria and polymicrobial infections increase hospital stays but not mortality.
Contribution
The study provides insights into the relationship between antibiotic resistance patterns and surgical outcomes in complicated intra-abdominal infections due to colorectal perforation.
Findings
Polymicrobial infections and multi-drug-resistant organisms are linked to longer hospital stays.
Documented intra-abdominal infections are associated with prolonged postoperative hospitalization.
Antibiotic resistance rates exceed 20% for many pathogens, but do not directly affect mortality.
Abstract
Background: Intra-abdominal infections (IAIs) are one of the leading causes of non-traumatic death in emergency surgery units. The appropriateness of empirical antibiotic therapy is fundamental for outcomes and for limiting the spread of resistance. This study aimed to assess the epidemiology and antibiotic resistance patterns of microorganisms recovered from complicated intra-abdominal infections due to colorectal perforation at an Italian University Hospital during a nine-year period. Methods: This study evaluated a cohort of patients subjected to emergency surgery for colonic perforation with collected intrabdominal fluid samples from 2015 to 2024. Patterns of isolated bacteria and antibiotic resistance status were collected and correlated to patient outcomes. Results: 321 patients were enrolled; the average age was 70.2 years. The main diagnoses were complicated diverticulitis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
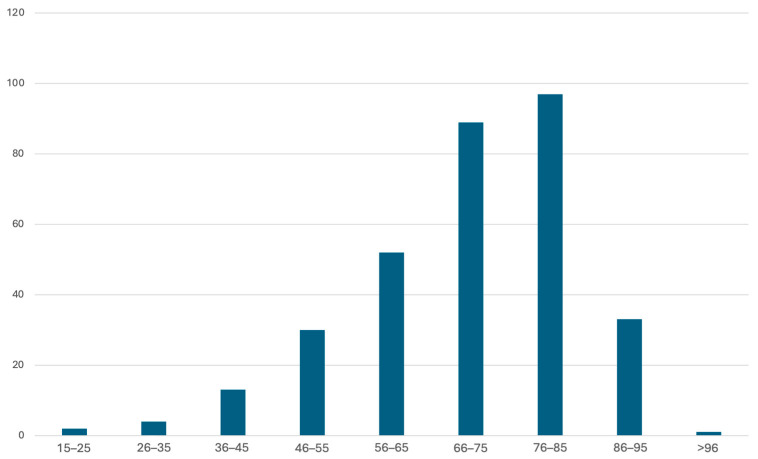 Figure 1
Figure 1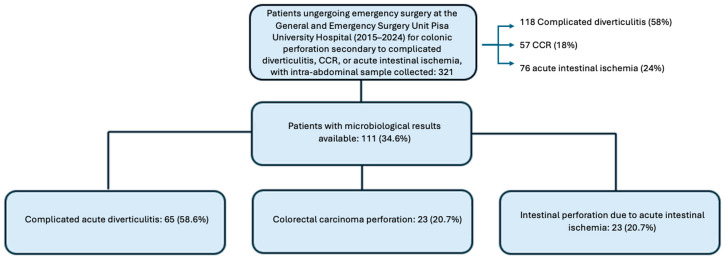 Figure 2
Figure 2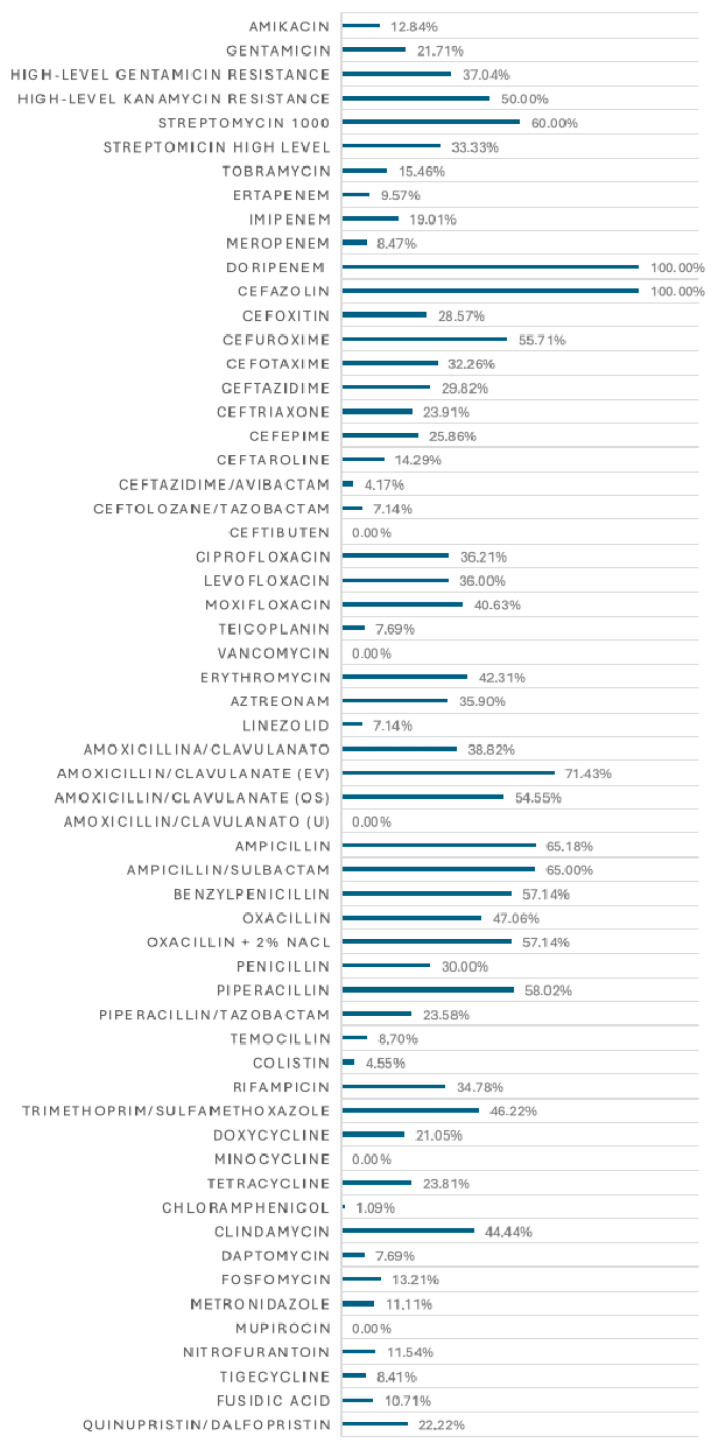 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiverticular Disease and Complications · Abdominal Surgery and Complications · Appendicitis Diagnosis and Management
1. Introduction
Intra-abdominal infections (IAIs) are common surgical emergencies and represent one of the leading causes of non-traumatic death in emergency surgery units worldwide. These infections comprise a broad and heterogeneous group of conditions characterized by an infectious process involving an abdominal organ or tissue [1]. The infection may be confined to the abdominal organ of origin (uncomplicated intra-abdominal infection) or extend to adjacent peritoneal or retroperitoneal structures or the peritoneal cavity itself (complicated intra-abdominal infections).
In uncomplicated forms, the infection remains confined within an organ, with no anatomical alterations of the gastrointestinal tract and without breaching the organ barrier. In complicated forms, the disease extends beyond the visceral peritoneum into the peritoneal space, resulting in abscess formation and/or peritonitis, which may be localized or diffuse [2]. These are severe clinical conditions that can involve diffuse peritoneal inflammation and carry the risk of progression to sepsis, septic shock, multi-organ failure, and death, with a reported global mortality rate of 9.2%. Despite a reduction in mortality over the past 15–20 years due to the implementation of early diagnosis and intensive care support, many patients today develop chronic critical illness, resulting in prolonged hospital stays, high resource utilization, and frequent discharge to post-acute care facilities.
Treatment for these conditions is based on three fundamental pillars: early initiation of antibiotic therapy, effective anatomical and physiological source control, and adequate fluid resuscitation and supportive care, especially in patients presenting with sepsis or septic shock [1]. Without an aggressive approach, there is a risk of progression to sepsis, septic shock, multi-organ dysfunction, and death [3,4,5,6].
“Source control” is the core of treatment: without it, the effectiveness of antibiotic therapy is limited, mortality rates can reach 100% and stabilizing the patient becomes challenging. During source control, the collection of samples from peritoneal fluid or abscesses for microbiological analysis (culture and antibiotic susceptibility testing) is essential to optimize antibiotic therapy [3,7,8].
The appropriateness of antibiotic therapy is crucial in determining clinical outcomes in these patients. Inappropriate antibiotic therapy is associated with prolonged hospital stays and increased mortality [1,3]. Antibiotic therapy must be initiated early and is therefore empirical in its initial phase [9]. Drug selection at this stage is guided by microbiological epidemiology, including the expected pathogens and patterns of antibiotic resistance [10,11,12,13]. Consequently, monitoring antibiotic resistance patterns is essential for appropriate therapeutic decisions [3].
The prevalence of antibiotic-resistant bacterial infections is steadily increasing, presenting a major challenge in antimicrobial therapy and a significant global health issue [1].
The use of adequate antibiotics is critical not only for individual patient outcomes, where it determines treatment efficacy, but also at the population level, as it minimizes the spread of antibiotic-resistant microorganisms. Optimizing empirical probabilistic antibiotic therapy and adjusting it based on culture results aligns with the principles of antibiotic stewardship. Once culture results are available (from intra-abdominal or blood samples), the antibiotic regimen can be adjusted, either by broadening or narrowing the spectrum of activity [1,14,15,16].
Antibiotic stewardship programs aim to develop guidelines for antibiotic use that address the growing challenge of antibiotic resistance [17,18,19].
The optimization of antibiotic use does not end with the selection of the most appropriate drug but also encompasses numerous other aspects: in 2023, the Global Alliance for Infections in Surgery (GAIS) [17] developed a ten-rule guideline for appropriate antimicrobial use in hospitals.
This study is therefore designed with the intention of implementing the knowledge of local bacteria epidemiology that may potentially improve the surveillance and monitoring of antibiotic resistance and the selection of the correct antibiotic.
2. Results
2.1. Patients’ Characteristics
A total of 321 patients were enrolled in the analysis. 136 (42.4%) were males and 185 (57.6%) females. The mean age was 70.2 years, with a median age of 73 years (SD ± 14.1) (Figure 1).
Out of the 321 analysed patients, 118 (58%) had a diagnosis of complicated acute diverticulitis, 57 (18%) had colorectal carcinoma perforation, and 76 (24%) presented with intestinal perforation due to acute bowel ischemia.
Microbiological analyses were available for a total of 111 patients, including 65 (58.6%) with complicated acute diverticulitis, 23 (20.7%) with colorectal carcinoma perforation, and 23 (20.7%) with intestinal perforation due to acute intestinal ischemia (Figure 2).
Among the sample, 63 patients (19.6%) were immunocompetent, while 258 patients (80.4%) had some degree of immunosuppression. Within the immunosuppressed group, 254 (98%) met the criteria for moderate immunosuppression, and 53 (20.5%) fulfilled the criteria for severe immunosuppression.
The average LOS was 15.6 days (median 12 days, SD ± 13.3), with a mean postoperative course duration of 13.8 days (median 10 days, SD ± 12.7 days).
During the postoperative period, 196 patients (60.1%) experienced various postoperative surgical complications with varying severity (Calvien–Dindo scores ≥ 2), which were distributed as follows: 91 (46.4%) with score 2, 26 (13.2%) with score 3, 11 (5.6%) with score 4, 67 (34.2%) with score 5 (death).
Out of the total cohort, 244 (70.0%) patients were discharged, while 67 (20.9%) patients died during hospitalization.
In-hospital mortality varied significantly across the three disease groups: Complicated diverticulitis: 21 deaths among 118 patients (17.7%); colorectal carcinoma perforation: 9 deaths among 57 patients (15.7%); intestinal perforation due to acute intestinal ischemia: 37 deaths among 76 patients (48.7%).
Among the 67 patients who died postoperatively, 46 (68.7%) died during their stay in the intensive care unit (ICU), while the remaining 13 (19.4%) died in the general ward.
Of the 244 discharged patients 196 (80.3%) were discharge at home; 19 (7.8%) were transferred to post-acute care or rehabilitation facilities and 24 (9.8%) were transferred to other departments for further treatments.
2.2. Microbiological Analysis and Antimicrobial Susceptibility
Microbiological positivity was observed in 111 (34.6%) out of 321 patients. In this subgroup, 63 patients (56.7%) exhibited mono-microbial cultures, while 48 patients (43.3%) had multi-microbial cultures. The culture examinations performed on the collected samples identified 29 distinct bacterial/fungal species. A detailed distribution of the various bacterial and fungal species is presented in Table 1.
The microbiological samples were tested for antimicrobial susceptibility. A total of 53 antibiotics and 9 antifungal agents were evaluated. The percentages of antibiotic resistance for the various isolated genera are presented in, highlighting antibiotic resistance rates exceeding 20%.
Cumulative antibiotic resistance rates were calculated based on the total number of isolates as well as on the total number of isolates tested for each antibiotic, as shown in Figure 3.
Antifungal resistance rates are reported separately for C. albicans and other Candida species. This distinction was made due to the significantly higher prevalence of C. albicans.
2.3. Clinical Outcome Analysis
The results of the multivariate analysis concerning the LOS (Table 2) show a statistically significant correlation between the type of diagnosis and the duration of hospitalization (p < 0.001). Moreover, a statistically significant correlation was observed between prolonged hospitalization and the presence of resistant and multidrug-resistant (MDR) organisms (p = 0.011; CR = 6.780).
The results of the multivariate analysis regarding the duration of the postoperative course (Table 3) confirm a positive correlation between a longer postoperative course and the presence of MDR organisms in the microbiological isolates (p = 0.003; CR = 8.075). In addition, a statistically significant association was found between prolonged postoperative recovery and the presence of multiple pathogens isolated from the same patient’s microbiological sample (p = 0.030; CR = 3.278).
The multivariate analysis regarding in-hospital mortality (Table 4) demonstrates a significant statistical correlation between mortality and patient age (p < 0.031), with older patients exhibiting a worse prognosis. In-hospital mortality was also significantly correlated with a diagnosis of intestinal ischemia (p < 0.001), indicating that the type of intra-abdominal infection influences patient prognosis due to the distinct pathophysiological alterations associated with sepsis.
An unexpected finding in this study was that mortality did not correlate with the characteristics of the analysed microbiological samples, including the number of isolates, the presence of resistant organisms, or the presence of MDR organisms.
The multivariate analysis concerning the occurrence of postoperative complications (Table 5) did not reveal any statistically significant correlation with the patient’s characteristics or the microbiological culture findings under investigation. No single factor appeared to have a predominant influence on the development of a complicated postoperative course.
3. Discussion
The sample distribution by sex and age group reflects the epidemiology of complicated IAI, with a peak prevalence between 75–85 years and a higher incidence in females [20,21,22]. Complicated acute diverticulitis accounts for more than half of the cases, while colorectal carcinoma perforation and intestinal ischemia represent 1/5 and 1/4 of the sample, respectively. This distribution is attributable to the higher prevalence of complicated acute diverticulitis in the general population (approximately 50% of colorectal perforation cases are diverticular) compared to colorectal carcinoma perforation and intestinal ischemia (particularly colonic ischemia), which are inherently less frequent events [23].
In the analysed sample, the percentage of patients with an immunocompromised state exceeds that of the general population [24]. This observation is influenced by the sample’s characteristics: the age of patients, the presence of active neoplastic disease, associated therapies and comorbidities [25]. The conditions under study, in fact, affect a population that is generally in the later decades of life and thus reflects the impact of associated comorbidities.
The most frequently isolated bacteria/yeast belonged to the normal intestinal flora, including Escherichia coli, Enterococci, Candida albicans, Enterobacteriaceae, and Citrobacter freundii [26]. Staphylococcus and Streptococcus species were also isolated, as well as Serratia marcescens, though less commonly. Pseudomonas aeruginosa and Klebsiella pneumoniae emerged as important pathogens, particularly in immunocompromised patients or those with prior antibiotic therapy [26]. While the association between infections by K. pneumoniae or P. aeruginosa and previous antibiotic administration was not specifically evaluated, colonization by these pathogens in hospitalized patients [26,27] may influence the selection of empirical antibiotic therapy.
The description of antibiotic resistance rates for the isolated pathogens provides crucial insights into the local and regional microbiological epidemiology. This information must be considered when establishing empirical antibiotic therapy for patients with complicated intra-abdominal infections.
Enterobacteriaceae, including E. coli, Klebsiella spp., Enterobacter spp., and C. freundii, exhibited resistance rates to penicillins exceeding 20%, except for piperacillin–tazobactam (40% resistance in Klebsiella spp. and Citrobacter spp.). For second- and third-generation cephalosporins, resistance rates generally exceeded 20%, limiting the use of these drugs in empirical therapy. However, newer cephalosporins, such as ceftazidime–avibactam and ceftolozane–tazobactam, displayed lower resistance rates, making them viable therapeutic options. Klebsiella spp. also showed resistance to carbapenems, aminoglycosides, and fluoroquinolones.
Significant resistance was observed among Gram-positive cocci, including Enterococci, Staphylococci, and Streptococci, with resistance rates exceeding 20% for beta-lactams and fluoroquinolones. Nevertheless, no isolates exhibited resistance to tigecycline.
Pseudomonas aeruginosa showed notable resistance to imipenem, ceftazidime, cefepime, and piperacillin–tazobactam (29% resistance), as well as to fluoroquinolones such as ciprofloxacin and levofloxacin (24% and 41%, respectively). These findings are critical given the increasing prevalence of resistance among nosocomial bacteria [28].
Drugs like amoxicillin/clavulanate and amoxicillin displayed resistance rates exceeding 20%, limiting their use. However, the piperacillin–tazobactam combination retained good efficacy, though it is classified under the “Watch” category in the AWaRe classification [29]. Cephalosporins such as ceftazidime, cefazolin, and cefoxitin had resistance rates below 20%, while other third-generation cephalosporins exhibited resistance rates above 20%. The use of ceftazidime–avibactam and ceftolozane–tazobactam should be avoided in empirical therapy as they are classified as “Reserve” antibiotics in the AWaRe classification [29,30]. Aminoglycosides, such as amikacin and gentamicin, remain important therapeutic options but must be used cautiously due to their side effects.
Doxycycline and nitrofurantoin, with resistance rates below 20%, may represent interesting therapeutic alternatives. Doxycycline offers a broad spectrum of activity, and nitrofurantoin has historically been used for urinary tract infections [31,32]. These drugs could potentially be useful in complicated intra-abdominal infections, although further studies are necessary.
The prevalence of C. albicans (13.04%) aligns with the (%) observed in previous studies [33], whereas all C. albicans isolates were susceptible to fluconazole in this study. Azole resistance was detected particularly in C. glabrata and C. parapsilosis, with the latter showing rates of fluconazole resistance above 50% of isolates. Nevertheless, echinocandins remain the appropriate therapeutic choice for intra-abdominal fungal infections [33,34].
The analysis of clinical outcomes in patients undergoing surgery for complicated intra-abdominal infections highlights the influence of the underlying diagnosis on hospital stay duration and mortality. Patients with complicated acute diverticulitis and colorectal perforation exhibited longer hospital stays compared to those with intestinal necrosis, primarily due to the higher perioperative mortality rate in the latter group. This reflects the combined impact of ischemic and septic conditions, often resulting in shorter yet unfavorable hospital courses.
Moreover, the isolation of antibiotic-resistant or multi-drug-resistant (MDR) bacteria from microbiological samples correlates with longer hospital stays and extended postoperative courses. Multivariate analysis confirms that the presence of MDR bacteria is a determinant of prolonged hospitalization. Immunosuppressed patients also tend to have extended postoperative recoveries. These findings suggest that the increasing prevalence of antibiotic resistance complicates the management of intra-abdominal infections, with significant implications for healthcare costs.
Mortality within the examined sample was higher than reported in the literature, likely due to the inclusion of only patients with complicated infections [1]. Advanced age was associated with increased in-hospital mortality, with a higher mean age of 75 years observed in deceased patients compared to 68 years in those discharged. Multivariate analysis confirms this correlation. Although immunosuppression appeared to influence postoperative mortality, this relationship was not significant in the multivariate analysis. Mortality due to intestinal necrosis from acute ischemia (48%) aligns with the literature (50%) [35], suggesting that the underlying pathology and its associated factors significantly impact patient survival.
Unlike other variables, in-hospital mortality did not appear to be influenced by microbiological findings, such as antibiotic resistance or polymicrobial infections, indicating that current treatment protocols remain effective. The lack of association between microbiological resistance patterns and mortality rates can partly be attributed to the limitations of our current diagnostic techniques. Standard lab methods, like EUCAST or CLSI, usually only examine a tiny fraction of the total bacterial population at the infection site. As pointed out by Andersson et al. (2019) [36], these techniques might miss important issues like heteroresistance or the existence of small multi-drug-resistant (MDR) subpopulations. These undetected resistant strains could have a major impact on clinical outcomes and the effectiveness of empirical therapy, even if the overall isolate seems susceptible in vitro.
Despite the complexity of intra-abdominal infections, advancements in surgical techniques and antibiotic management have contributed to reducing mortality over time [1].
Postoperative complications were positively correlated with immunosuppression, advanced age, and the presence of resistant bacteria. However, multivariate analysis did not identify a significant relationship between these factors and postoperative morbidity. The lack of specific data on complications limits the interpretation of these findings.
Most of the patients (196–80.3%) were discharged at home, while some were transferred to rehabilitation facilities or other departments (43–17.6%).
The study has several limitations, including patient selection and its retrospective design, which hindered the collection of critical data such as intensive care unit stay duration and details of antibiotic treatments. Additionally, the heterogeneity of the sample across different diseases (acute diverticulitis, carcinoma perforations, and intestinal ischemia) represents another potential limitation. Lastly, it should be noted that the sample does not represent all treated patients but only a subset due to the inclusion only of those who had complete microbiological analysis. A study limitation that must be disclosed lies within the current laboratory routine workflow and the retrospective nature of the study. Authors acknowledge the important limitations of antimicrobial susceptibility testing via broth microdilution test which to date is still the gold standard in detecting resistant phenotypes, however in a broader and deeper view in terms of antimicrobial resistance, molecular methods along with whole genome sequencing show the highest sensitivity in depicting and deciphering underlying antimicrobial resistant patterns within the study population, as they can evaluate heteroresistant and tolerance genomic traits within the biological diversity present in the patient.
4. Methods
This study retrospectively analyzed data of patients who underwent emergency surgery at the General and Emergency Surgery Unit at Pisa University Hospital, Italy, between January 2015 and August 2024, with diagnoses of colonic perforation due to complicated acute diverticulitis, colorectal carcinoma, or acute intestinal ischemia, for whom intraoperative intra-abdominal cultures were available. Clinical data were extracted from the hospital electronic medical records. Microbiological results from these samples, including peritoneal fluid, blood, and other specimens (urine, broncho-aspirate, surgical wound swabs), were obtained from the microbiology department.
The analyses included culture tests, microbial species identification, and susceptibility testing via microbroth dilution, assessed based on minimum inhibitory concentration (MIC) values according to EUCAST guidelines (SIR system: sensitive, susceptible, increased exposure—previously defined as “intermediate susceptibility”—and resistant) [37]. Isolates of Candida spp. were interpreted following CLSI standards [38]. Sensititre YeastOne Y010© (Thermo Fisher Diagnostics B.V., Lansmeer, The Netherlands) was used for antifungal susceptibility testing. Yeast isolates were incubated at 37 °C for 24–48 h under aerobic conditions, then 3 to 5 separeted yeast colonies were suspended in sterile distilled water. The solution was vortexed and homogenized to reach a final concentration of 0.5 McFarland analyzed with a spectrophotometer. The final inoculum concentration was 0.5 × 10^3^–2.5 × 10^3^ cells/mL according to the CLSI guidance document. Colorimetric broth microtitration plate Sensititre YeastOne Y010© was incubated at 35–37 °C and checked for growth of the fungal microorganism at 24 h and 48 h according to different species.
Antibiotics with intermediate sensitivity were classified as “non-resistant” for calculating resistance percentages, which were based on the total number of microorganisms tested.
Immunocompromised status was defined according to the parameters established by the World Society of Emergency Surgery (WSES) [39].
Clinical outcomes analysed included in-hospital mortality, length of stay (LOS), postoperative course, and postoperative morbidity, defined as a complicated postoperative course (Clavien–Dindo score ≥ 2) [40]. Length-of-stay data were retrieved from clinical records in the electronic database. Missing data were considered as absent (missing) for analysis. The study protocol (n. 17575) was approved by the Regional Ethical Committee. The statistical analysis included the description of sample characteristics, microbiological epidemiology, and the association between clinical outcomes, immunosuppression, and microbiological patterns of isolates. Categorical data were described using absolute and relative frequencies (%), while continuous variables were expressed as mean and standard deviation (SD). Associations between qualitative variables were analysed using the chi-square test; for quantitative variables, t-tests or ANOVA were employed. Pearson’s correlation analysis was used for quantitative outcomes. Multivariate analysis was conducted using logistic regression models for categorical outcomes and linear regression models for quantitative outcomes, with statistical significance set at 0.05. Analyses were performed using SPSS version 29.
5. Conclusions
Microbiological characteristics of isolated bacteria do not directly influence mortality; however, the presence of polymicrobial infections and resistant pathogens directly affects the duration of hospitalization and often leads to the development of chronic disease conditions.
Despite its limitations, the study gives strong support to the necessity of continuously monitoring antibiotic resistance patterns to optimize empirical therapy selection for complicated intra-abdominal infections. Antibiotic resistance constrains the efficacy of many commonly used antibiotics, while identifying drugs with low resistance rates could guide future research in empirical therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sartelli M. Coccolini F. Kluger Y. Agastra E. Abu-Zidan F.M. Abbas A.E.S. Ansaloni L. Adesunkanmi A.K. Atanasov B. Augustin G. WSES/GAIS/SIS-E/WSIS/AAST global clinical pathways for patients with intra-abdominal infections World J. Emerg. Surg.2021164910.1186/s 13017-021-00387-834563232 PMC 8467193 · doi ↗ · pubmed ↗
- 2Khatri R. Sawyer R. Global Perspectives in Controversies Related to the Management of Intra-Abdominal Infections Surg. Infect.20202162663310.1089/sur.2020.17432543289 · doi ↗ · pubmed ↗
- 3Shirah G.R. O’Neill P.J. Intra-abdominal Infections Surg. Clin. N. Am.2014941319133310.1016/j.suc.2014.08.00525440126 · doi ↗ · pubmed ↗
- 4Moore L.J. Moore F.A. Jones S.L. Xu J. Bass B.L. Sepsis in general surgery: A deadly complication Am. J. Surg.200919886887410.1016/j.amjsurg.2009.05.02519969144 · doi ↗ · pubmed ↗
- 5Coccolini F. Kirkpatrick A.W. Cremonini C. Sartelli M. Source control in intra-abdominal infections: What you need to know J. Trauma. Acute Care Surg.2025 online ahead of print 10.1097/TA.000000000000465440492849 · doi ↗ · pubmed ↗
- 6Coccolini F. Sartelli M. Sawyer R. Rasa K. Viaggi B. Abu-Zidan F. Soreide K. Hardcastle T. Gupta D. Bendinelli C. Source control in emergency general surgery: WSES, GAIS, SIS-E, SIS-A guidelines World J. Emerg. Surg.2023184110.1186/s 13017-023-00509-437480129 PMC 10362628 · doi ↗ · pubmed ↗
- 7Bloos F. Thomas-Rüddel D. Rüddel H. Engel C. Schwarzkopf D. Marshall J.C. Harbarth S. Simon P. Riessen R. Keh D. Impact of compliance with infection management guidelines on outcome in patients with severe sepsis: A prospective observational multi-center study Crit. Care 201418 R 4210.1186/cc 1375524589043 PMC 4057316 · doi ↗ · pubmed ↗
- 8Mulier S. Penninckx F. Verwaest C. Filez L. Aerts R. Fieuws S. Lauwers P. Factors Affecting Mortality in Generalized Postoperative Peritonitis: Multivariate Analysis in 96 Patients World J. Surg.20032737938410.1007/s 00268-002-6705-x 12658477 · doi ↗ · pubmed ↗