Successful Bridging to Rituximab With Plasma Exchange in a Pediatric Patient With Severe Lupus Nephritis
Taro Yoshida, Hiroshi Sugahara, Keisuke Oikawa, Chinatsu Onodera, Manami Akasaka

TL;DR
A 14-year-old girl with severe lupus nephritis improved after plasma exchange and a combination of immunosuppressive treatments, including rituximab.
Contribution
Demonstrates the effectiveness of early plasma exchange in enabling rituximab treatment for severe pediatric lupus nephritis.
Findings
Plasma exchange reduced autoantibodies and improved renal function in a pediatric lupus nephritis patient.
The patient achieved complete remission with normalization of serologic markers and urinary findings.
Combination therapy allowed successful discontinuation of corticosteroids after 18 months.
Abstract
We report a case of a 14-year-old girl diagnosed with class IV-G (A) lupus nephritis (LN), presenting with severe clinical manifestations, including nephrotic syndrome, acute kidney injury, and life-threatening hyperkalemia. The condition was managed with early initiation of plasma exchange (PE), followed by a combination of immunosuppressive therapies: high-dose corticosteroids, mycophenolate mofetil, rituximab, tacrolimus, and hydroxychloroquine. PE was promptly introduced after methylprednisolone pulse therapy to reduce circulating pathogenic autoantibodies and mitigate renal inflammation. Renal function gradually improved, accompanied by a marked decline in antibody levels. During recovery, the patient developed deep vein thrombosis and pulmonary embolism, which were managed with anticoagulation therapy. Belimumab was subsequently added to facilitate steroid tapering and maintain…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
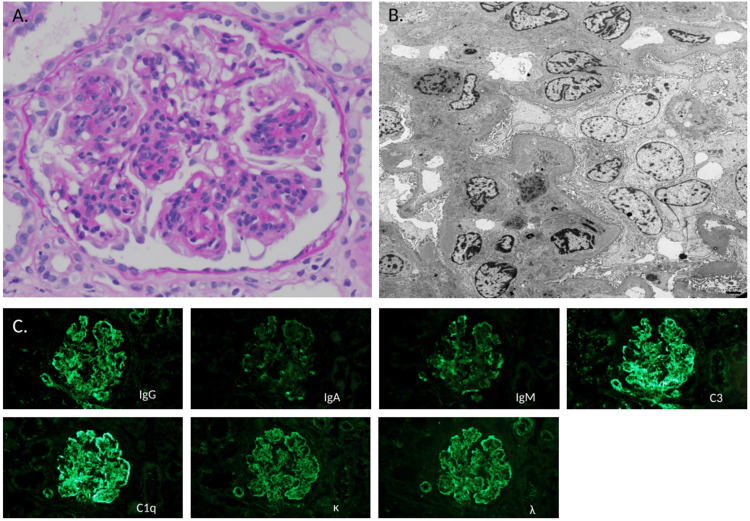 Figure 1
Figure 1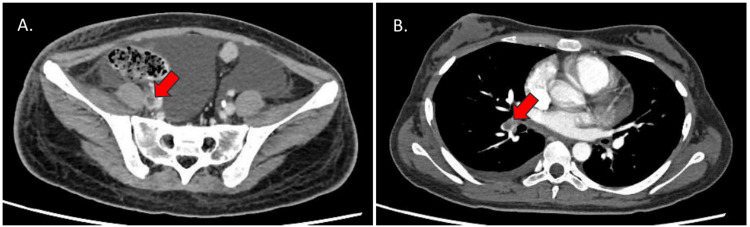 Figure 2
Figure 2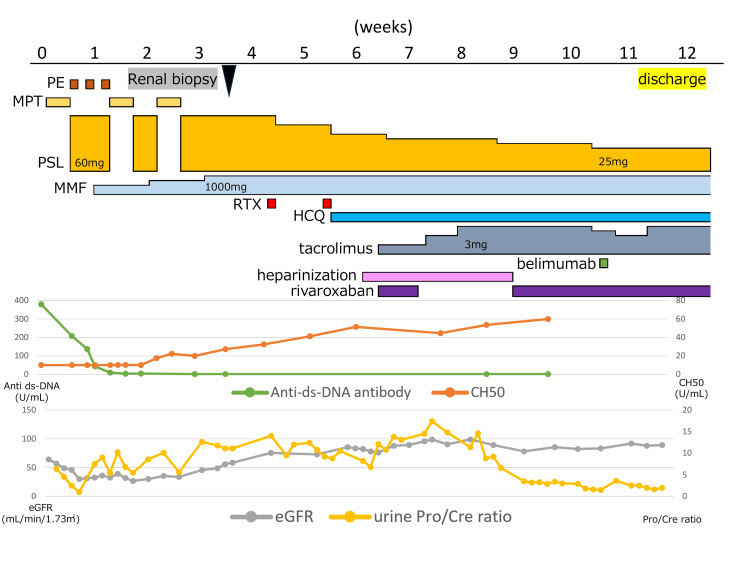 Figure 3
Figure 3| Category | Parameter | Observed value | Reference range | Unit |
| Hematology | WBC | 3,120 | 3,500–9,000 | /µL |
| Neutrophils | 58.4 | 40–70 | % | |
| Lymphocytes | 25.6 | 20–45 | % | |
| Monocytes | 7.5 | 2–10 | % | |
| Hemoglobin | 10 | 11.5–15.5 | g/dL | |
| Platelet count | 13.9 | 15–35 | ×10⁴/µL | |
| Reticulocytes | 3.5 | 2–8 | ×10⁴4/µL | |
| Coagulation | PT-INR | 0.85 | 0.9–1.1 | - |
| APTT | 33.8 | 25–40 | seconds | |
| Fibrinogen | 389 | 200–400 | mg/dL | |
| FDP | 9 | <5 | µg/mL | |
| Antithrombin III | 44 | 80–120 | % | |
| Biochemistry | Total protein | 4.3 | 6.5–8.0 | g/dL |
| Albumin | 1.5 | 3.8–5.3 | g/dL | |
| BUN | 31.9 | 7–20 | mg/dL | |
| Cre | 0.97 | 0.4–0.9 | mg/dL | |
| AST | 115 | 10–40 | IU/L | |
| ALT | 146 | 5–40 | IU/L | |
| LD | 268 | 120–240 | IU/L | |
| T-Bil | <0.1 | 0.2–1.2 | mg/dL | |
| Na | 136 | 135–145 | mmol/L | |
| K | 6.6 | 3.5–5.0 | mmol/L | |
| Cl | 114 | 98–108 | mmol/L | |
| Ca | 7.6 | 8.8–10.2 | mg/dL | |
| P (inorganic phosphate) | 4.9 | 3.5–5.5 | mg/dL | |
| CRP | <0.1 | <0.3 | mg/dL | |
| Immunology | IgG | 1209 | 700–1600 | mg/dL |
| IgA | 217 | 70–400 | mg/dL | |
| IgM | 192 | 40–230 | mg/dL | |
| BNP | 17 | <18 | pg/mL | |
| Ferritin | 843 | 10–150 | ng/mL | |
| CH50 | <10 | 30–45 | U/mL | |
| C3 | 27 | 80–160 | mg/dL | |
| C4 | 2 | 15–45 | mg/dL | |
| Direct Coombs test | Positive | Negative | ||
| Autoantibodies | ANA | 1,280 | Negative | Titer |
| anti-ssDNA | >800 | Negative | U/mL | |
| anti-dsDNA | 380 | Negative | U/mL | |
| anti-RNP | 5.2 | Negative | U/mL | |
| anti-Scl-70 | <1 | Negative | U/mL | |
| anti-SS-A | 512.3 | Negative | U/mL | |
| anti-SS-B | 5.6 | Negative | U/mL | |
| anti-Sm | <1.0 | Negative | U/mL | |
| MMP3 | 30 | <60 | ng/mL | |
| Anticardiolipin IgG | <4.0 | Negative | µg/mL | |
| Urinalysis | Red blood cells | >100 | 0–4 /HPF | /HPF |
| White blood cells | 30–49 | 0–4 /HPF | /HPF | |
| Granular casts | 1+ | Negative | ||
| Epithelial casts | 2+ | Negative | ||
| Waxy casts | 1+ | Negative | ||
| Red blood cell casts | 1+ | Negative | ||
| Urine sodium | 20 | N/A | mEq/L | |
| Urine potassium | 59.3 | N/A | mEq/L | |
| Urine chloride | 20 | N/A | mEq/L | |
| Urine creatinine | 177 | N/A | mg/dL | |
| U-NAG | 31.9 | ≤10 | U/L | |
| U-Protein/Cre | 6.4 | <0.2 | ||
| β2MG | <100 | <300 | µg/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Systemic Lupus Erythematosus Research · Complement system in diseases
Introduction
Lupus nephritis (LN) is a common and serious manifestation of systemic lupus erythematosus (SLE), particularly in the pediatric population, where it is associated with increased disease activity and worse renal outcomes compared to adults [1]. Despite advances in immunosuppressive therapy, if not promptly controlled, a subset of patients develops aggressive disease that progresses rapidly to end-stage kidney disease [2]. Early intervention and careful selection of therapeutic strategies are critical. Plasma exchange (PE) has been used selectively in severe complications of SLE, such as rapidly progressive glomerulonephritis or catastrophic antiphospholipid syndrome [3], but its broader role remains under investigation. In this report, we describe a pediatric patient with severe LN who was successfully treated with early PE and rituximab, highlighting the potential benefits of early aggressive intervention.
Case presentation
A 14-year-old girl presented with a two-month history of facial rash and ear erythema, which progressed to generalized edema. Initial laboratory tests revealed thrombocytopenia (13.9 × 10⁴/μL), anemia (10.0 g/dL), hyperkalemia (6.6 mmol/L), elevated serum creatinine (0.97 mg/dL), hypoalbuminemia (1.5 g/dL), and nephrotic-range proteinuria (urinary protein/creatinine ratio: 6.6). Immunological evaluation demonstrated strongly positive antinuclear antibodies (ANA, 1:1,280) and marked hypocomplementemia (CH50 <10 U/mL, C3 27 mg/dL, and C4 2 mg/dL). Serological testing showed markedly elevated anti-dsDNA (380 U/mL) and anti-SSA (512.3 U/mL) antibody titers, with a Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score of 26. Additional baseline laboratory findings at presentation are summarized in Table 1.
A kidney biopsy was performed on hospital day 25. In the renal biopsy specimens, endocapillary hypercellularity was observed in 16 glomeruli (64%), mesangial cell proliferation in seven glomeruli (28%) (Figure 1a), intracapillary inflammatory infiltration in five glomeruli (20%), lobular appearance in three glomeruli (12%), and cellular crescents in two glomeruli (8%). A wire-loop lesion was found in one glomerulus (4%). Fibrinoid necrosis was not observed in all glomeruli. Interstitial fibrosis involved about 5% of the sampled cortex. Transmission electron microscopy revealed electron-dense deposits in the mesangial areas, as well as thesubepithelial and subendothelial areas of the glomerular basement membrane (Figure 1b). Immunofluorescence staining revealed positive reactivity along the glomerular capillary walls and in the mesangial areas in all staining markers (Figure 1c). Overall, renal biopsy findings were suggestive of diffuse LN: International Society of Nephrology/Renal Pathology Society 2018 modification: Class IV, Indices (Modified National Institutes of Health-NIH) of activity 8/24, and chronicity 2/12.
Histopathological findings of the renal biopsy specimens.(A) Mesangial proliferation is observed in the glomerulus (periodic acid-Schiff, 400×).(B) Transmission electron microscopy shows electron-dense deposits in the mesangial areas, as well as the subepithelial and subendothelial regions of the glomerular basement membrane (1,500×).(C) Immunofluorescence staining reveals positive reactivity along the glomerular capillary walls and in the mesangial areas across all the staining markers (200×).
After correction of hyperkalemia, methylprednisolone pulse therapy was initiated on day two and administered for three cycles. Given the severity of LN, characterized by nephrotic syndrome, acute kidney injury with life-threatening hyperkalemia, extremely high anti-dsDNA titers, and marked systemic inflammation with a SLEDAI score of 26, rapidly progressive immune complex-mediated renal injury was strongly suspected. Despite steroid pulse therapy, the patient developed worsening fluid overload requiring intermittent hemodialysis. Hemodialysis was performed on hospital days 4, 5, 7, 10-12, and 18-19, and was discontinued after day 19 as the patient’s fluid balance, respiratory status, and renal function improved. PE was initiated on day four as a bridging strategy to promptly reduce circulating immune complexes and pathogenic autoantibodies until the therapeutic effects of subsequent immunosuppressive agents could be achieved. Mycophenolate mofetil was introduced on day eight. Although anemia and thrombocytopenia were present at admission, these cytopenias did not worsen after the initiation of methylprednisolone pulse therapy and supportive care. Although the histopathological results were not available at the time of treatment escalation, rituximab was administered on days 30 and 37 based on the severity of the clinical and serological findings, followed by the addition of hydroxychloroquine and tacrolimus. The subsequent biopsy results revealed diffuse LN with high activity, which supported the appropriateness of the chosen therapeutic approach. An angiotensin-converting enzyme inhibitor and an angiotensin II receptor blocker (ARB) were added for renal protection. Anti-dsDNA antibody levels declined rapidly after PE, and complement levels improved by day 11 and normalized by day 36. Belimumab was introduced on day 72. In accordance with the prescribing information, belimumab was administered at a dose of 200 mg per infusion, with the first three doses given at two-week intervals, followed by maintenance dosing every four weeks, adjusted according to disease activity. After sustained stabilization of clinical symptoms, renal function, and serological markers, mycophenolate mofetil was discontinued on hospital day 184, and tacrolimus was discontinued on hospital day 211.
On hospital day 42, the patient developed right lower leg edema and cough, prompting evaluation for thromboembolic complications. Contrast-enhanced CT revealed thrombi in the right common iliac vein and right external iliac vein, as well as a pulmonary artery embolism (Figure 2).
Contrast-enhanced CT findings of iliac vein thrombosis and pulmonary embolism.(A) Contrast-enhanced CT of the pelvis demonstrates thrombi in the right common iliac vein (arrows).(B) Contrast-enhanced CT of the chest reveals filling defects in the pulmonary arteries, consistent with pulmonary embolism (arrows).
Anticoagulation therapy with heparin followed by rivaroxaban was initiated. The common iliac vein thrombus resolved by day 72; however, a mural thrombus in the external iliac vein persisted, requiring continued anticoagulation. The patient was discharged on day 82 (Figure 3). Proteinuria improved by day 114, while urinary casts and hematuria resolved by days 309 and 526, respectively. Corticosteroids were tapered to 5 mg by day 365 and completely discontinued by day 555. At the last follow-up, the patient was maintained on hydroxychloroquine, belimumab, and an ARB alone, with a sustained SLEDAI score of 0.
Clinical course of the patient.Alb: albumin; HCQ: hydroxychloroquine; MMF: mycophenolate mofetil; MPT: methylprednisolone pulse therapy; PE: plasma exchange; Pro/Cre: protein/creatinine; PSL: prednisolone; RTX: rituximab
Discussion
This case illustrates the potential utility of early PE as a bridging therapy to rituximab in the management of severe pediatric LN. PE may rapidly reduce levels of pathogenic circulating immune complexes and autoantibodies, helping stabilize renal function during the critical early phase of treatment [4]. In our case, PE was initiated within the first week of admission, allowing timely rituximab administration and effective disease control. This strategy may be particularly beneficial in patients with impaired renal function, where immediate immunosuppression alone may be insufficient. Although the KDIGO 2024 guidelines recommend PE in cases of thrombotic microangiopathy or rapidly progressive glomerulonephritis in SLE [5], broader indications for its use remain unclear [6-8].
Given the patient’s young age, concerns regarding potential gonadotoxicity were substantial. Recent evidence has demonstrated that mycophenolate mofetil provides efficacy comparable to cyclophosphamide for induction therapy in LN, including pediatric populations. Therefore, we adopted a treatment strategy combining mycophenolate mofetil with early PE and rituximab to achieve rapid disease control while minimizing exposure to cyclophosphamide.
In recent years, the use of rituximab has increased in pediatric patients with refractory or severe LN, and favorable outcomes have been reported when rituximab is introduced in combination with PE as a bridging strategy [9,10]. Based on these considerations, rituximab was selected as an adjunctive therapy to provide effective immunosuppression during the acute phase without cyclophosphamide-associated toxicity.
A notable outcome in our case was the successful tapering and discontinuation of corticosteroids, facilitated by the use of rituximab and maintenance therapy with hydroxychloroquine and belimumab. Given the long-term side effects of corticosteroids, particularly in children, steroid-sparing strategies are of great clinical importance [11]. Although the use of belimumab in pediatric LN is still under evaluation [12,13], our experience suggests its potential role in maintaining remission and preventing disease flare.
Additionally, this case underscores the importance of thromboprophylaxis in pediatric SLE patients with central venous access and prolonged immobility. Risk factors for thrombosis during SLE treatment include antiphospholipid antibodies, LN, absence of thrombocytopenia, and corticosteroid use [14,15]. Despite the absence of antiphospholipid antibodies, our patient developed deep vein thrombosis and pulmonary embolism. In this case, physiotherapy was initiated on hospital day 16; however, prolonged bed rest was unavoidable due to the placement of a femoral central venous catheter for blood purification therapy. The catheter remained in place from hospital day 4 to day 23. An increasing trend in D-dimer levels was noted from day 21 and persisted after catheter removal, preceding the onset of pulmonary embolism symptoms on day 42. In addition to high-dose corticosteroid therapy, these factors likely contributed to the development of thromboembolic complications. Awareness of these risks and the implementation of early preventive strategies should be integral to the management of pediatric SLE patients.
Taken together, this case highlights the effectiveness of individualized, multimodal therapy, including early PE and targeted biologics, in managing severe pediatric LN. This study also highlights the need for standardized treatment protocols and further research to optimize therapeutic sequencing, improve outcomes, and reduce treatment-related toxicities in this vulnerable population.
Conclusions
This case suggests that early PE may function as an effective bridging strategy to rituximab in pediatric patients with severe LN. Rapid removal of circulating immune complexes by PE appeared to facilitate disease stabilization and enable timely initiation of biologic therapy. Although the role of PE in LN remains controversial, this case highlights the importance of individualized, multimodal treatment approaches in high-risk pediatric patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lupus nephritis in children: novel perspectives Medicina (Kaunas) Pennesi M Benvenuto S 18415920233789355910.3390/medicina 59101841 PMC 10607957 · doi ↗ · pubmed ↗
- 2Kidney outcomes for children with lupus nephritis Pediatr Nephrol Oni L Wright RD Marks S Beresford MW Tullus K 137713853620213272554310.1007/s 00467-020-04686-1PMC 8084759 · doi ↗ · pubmed ↗
- 3Therapeutic plasma exchange for refractory SLE: a comparison of outcomes between different sub-phenotypes Eur J Rheumatol Soyuöz A KaradağÖ KaraağaçT KılıçL BilgenŞA Özcebe Oİ 3236520182965787210.5152/eurjrheum.2017.17088 PMC 5895148 · doi ↗ · pubmed ↗
- 4Basic principles of therapeutic plasma exchange Transfus Apher Sci Weinstein R 1036756220233684932210.1016/j.transci.2023.103675 · doi ↗ · pubmed ↗
- 5KDIGO 2024 Clinical Practice Guideline for the management of lupus nephritis Kidney Int 0105202410.1016/j.kint.2023.09.00238182286 · doi ↗ · pubmed ↗
- 6Comparative effects of plasmapheresis and intravenous cyclophosphamide on urinary podocyte excretion in patients with proliferative lupus nephritis Clin Nephrol Nakamura T Ushiyama C Hara M 1081135720021186311910.5414/cnp 57108 · doi ↗ · pubmed ↗
- 7Randomized controlled trial of pulse/synchronization cyclophosphamide/apheresis for proliferative lupus nephritis J Clin Apher Wallace DJ Goldfinger D Pepkowitz SH Fichman M Metzger AL Schroeder JO Euler HH 163166131998988679510.1002/(sici)1098-1101(1998)13:4<163::aid-jca 4>3.0.co;2-1 · doi ↗ · pubmed ↗
- 8A controlled trial of plasmapheresis therapy in severe lupus nephritis. The Lupus Nephritis Collaborative Study Group N Engl J Med Lewis EJ Hunsicker LG Lan SP Rohde RD Lachin JM 137313793261992156997310.1056/NEJM 199205213262101 · doi ↗ · pubmed ↗