Clinical Images: Sarcoidosis revealed by recurrent dactylitis
Thomas Subervie, Thibault Willaume, Amin Maazouzi, Jacques‐Eric Gottenberg, Jean Sibilia, Noëlle Weingertner, Eden Sebbag, Marc Scherlinger

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
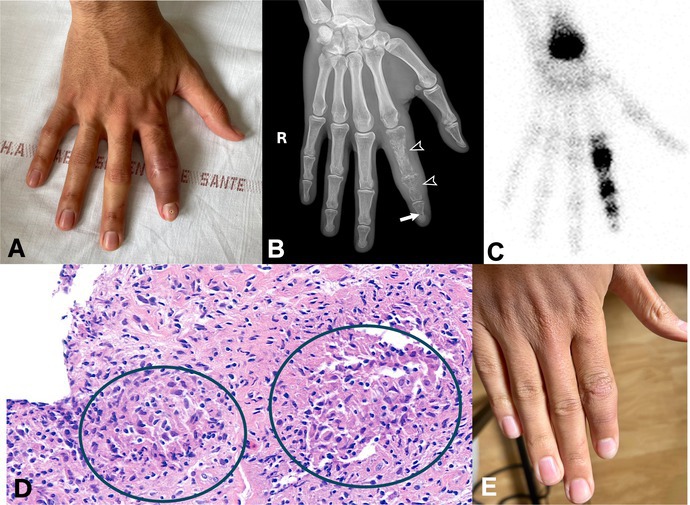 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Ocular Diseases and Behçet’s Syndrome · Research on Leishmaniasis Studies
(A) A 21‐year‐old man presented with chronic and recurrent dactylitis of the index finger. (B) The conventional radiography showed osteolytic changes in the three phalanges of the right index finger, with a characteristic honeycomb (or lattice) appearance in P1 and P2 (black arrowheads) and a cystoid lesion in P3 (white arrow) associated with thickening of the surrounding soft tissues. Of note, there is no joint space narrowing in the metacarpophalangeal and interphalangeal joints. (C) Technetium‐99 scintigraphy identified multiple areas of increased uptake. (D) Histopathological analysis of biopsies obtained by a hand surgeon showed chronic aseptic osteitis and noncaseating granulomas (green circles) within the synovium, consistent with a diagnosis of sarcoidosis. Interferon‐γ release assay for Mycobacterium tuberculosis was negative, as was culture for mycobacteria and M tuberculosis polymerase chain reaction. Additional findings supporting the diagnosis of systemic sarcoidosis included hypermetabolic mediastinal and hilar lymphadenopathies on positron emission tomography–computed tomography with pulmonary micronodules, elevated angiotensin‐converting enzyme, hypergammaglobulinemia, and lymphopenia. Bone involvement may be present in 1% to 15% of patients with sarcoidosis and is often asymptomatic.1 The spine is the most commonly affected site, followed by the pelvis.2, 3 The classic lesions in the small bones of the hands and feet like in this case are known as Perthes and Jüngling disease.2 (E) The patient was treated with a tapering course of glucocorticoids and methotrexate, and there was improvement in the dactylitis.
Supporting information
Disclosure Form
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kucharz EJ . Osseous manifestations of sarcoidosis. Reumatologia 2020;58:93–100.32476682 10.5114/reum.2020.95363 PMC 7249525 · doi ↗ · pubmed ↗
- 2Hassine IB , Rein C , Comarmond C , et al. Osseous sarcoidosis: a multicenter retrospective case‐control study of 48 patients. Joint Bone Spine 2019;86:789–93.31374357 10.1016/j.jbspin.2019.07.009 · doi ↗ · pubmed ↗
- 3Zhou Y , Lower EE , Li H , et al. Clinical characteristics of patients with bone sarcoidosis. Semin Arthritis Rheum 2017;47(1):143–148.28274482 10.1016/j.semarthrit.2017.02.004 · doi ↗ · pubmed ↗