Poor Outcome of Metastatic Cutaneous Squamous Cell Carcinoma: A Swedish Retrospective Study
Charlotta L. PALMQVIST, Mathias VON BECKERATH

TL;DR
This study examines metastatic cutaneous squamous cell carcinoma in Sweden, finding that it affects elderly patients and has a high mortality rate.
Contribution
This is the first published study on metastatic cutaneous squamous cell carcinoma in Sweden.
Findings
Metastatic cutaneous squamous cell carcinoma occurs in elderly but generally healthy patients.
Most metastases are diagnosed within two years of the primary tumor diagnosis.
Overall survival at two years is 56%.
Abstract
The incidence of cutaneous squamous cell carcinoma is increasing rapidly, and 1.5–5% of cases develop metastatic disease, which is associated with a markedly worse prognosis. This study aimed to describe the characteristics of the primary tumour, the patients, and the metastases, as well as treatment and outcomes in patients with metastatic cutaneous squamous cell carcinoma. A total of 137 patients with a diagnosis of metastatic cutaneous squamous cell carcinoma within the Stockholm region during 2012–2020 were identified and included. Median age was 81; 79% were male; 70% had a WHO performance status of 0–1. 50% of the primary tumours were classified as high-risk tumours according to the Brigham and Women’s Hospital system. The median time between diagnosis of the primary tumour and the diagnosis of regional metastases was 7 months and 90% of the metastases were diagnosed within 2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
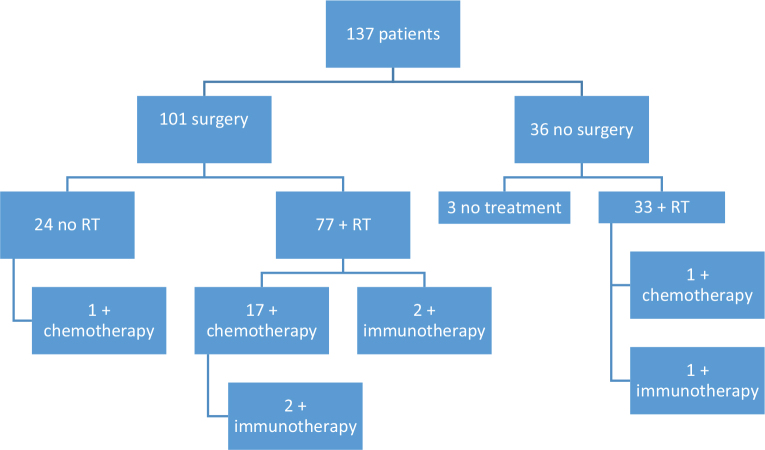 Fig. 1
Fig. 1| Variable | |
|---|---|
| Number of patients | 137 (100) |
| Age, years | |
| ≤ 60 | 4 (3) |
| 60–80 | 61 (45) |
| > 80 | 72 (53) |
| Sex | |
| Female | 29 (21) |
| Male | 108 (79) |
| Smoking | |
| Active smoker | 8 (6) |
| Previous smoker | 58 (42) |
| Never smoked | 71 (52) |
| Immunosuppression | |
| No | 103 (75) |
| Yes (total) | 34 (25) |
| CLL | 18 |
| Organ transplant | 8 |
| Other blood disease | 6 |
| Other | 2 |
| WHO performance status | |
| Ps 0 | 66 (48) |
| Ps 1 | 30 (22) |
| Ps 2 | 24 (18) |
| Ps 3 | 15 (11) |
| Ps 4 | 2 (1) |
| Previous diagnosis of cSCC | |
| Yes | 44 (32) |
| No | 93 (68) |
| Variable | |
|---|---|
| Number of known primary tumours | 135 (100) |
| Site | |
| Ear | 28 (21) |
| Temple | 26 (19) |
| Cheek | 21 (16) |
| Scalp | 18 (13) |
| Periauricular | 14 (10) |
| Forehead | 9 (7) |
| Lip (vermilion) | 7 (5) |
| Neck | 6 (4) |
| Nose | 5 (4) |
| Chin | 1 (1) |
| Size | |
| < 2 cm | 51 (39) |
| ≥ 2 cm | 80 (61) |
| unknown | 4 (3) |
| Degree of pathological differentiation | |
| Low | 52 (41) |
| Moderate | 66 (52) |
| High | 9 (7) |
| Unknown | 8 (6) |
| Perineural invasion | |
| Yes | 21 (16) |
| No/unknown | 114 (84) |
| Growth beyond fat | |
| Yes | 51 (38) |
| No/unknown | 84 (62) |
| BWH | |
| T1 | 27 (21) |
| T2a | 38 (30) |
| T2b | 57 (45) |
| T3 | 5 (4) |
| Unknown | 3 |
| Radical margins | |
| Positive | 49 (39) |
| Negative | 76 (61) |
| Unknown | 2 (1) |
| Non-surgical treatment of primary tumour | 8 (6) |
| Variables | |
|---|---|
| Type of advanced cSCC | |
| Metastases | 128 (93) |
| Regional metastases | 123 |
| Distant metastases only | 5 |
| Distant metastases | 29 |
| Locally advanced disease without metastases | 9 |
| cTNM | |
| T1 | 53 (39) |
| T2 | 19 (14) |
| T3 | 60 (44) |
| T4 | 1 (1) |
| Tx | 4 (3) |
| N0 | 16 (12) |
| N1 | 21 (15) |
| N2a | 4 (3) |
| N2b | 23 (17) |
| N2c | 5 (4) |
| N3a | 0 (0) |
| N3b | 68 (50) |
| M0 | 119 (87) |
| M1 | 14 (10) |
| Mx | 4 (3) |
| Stage (excluding lip) | |
| I | 0 (0) |
| IIa | 12 (9) |
| IIb | 0 (0) |
| IIIa | 16 (12) |
| IIIb | 27 (21) |
| IV | 75 (58) |
| Stage lip cancer | |
| I | 0 |
| II | 0 |
| III | 3 (43) |
| IVa | 2 (29) |
| IVb | 2 (29) |
| Variable | |
|---|---|
| Type of treatment | |
| Surgery only | 23 (17) |
| Surgery + RT | 58 (42) |
| Surgery + RT + chemotherapy | 15 (11) |
| Surgery + RT + chemotherapy + immunotherapy | 2 (1) |
| Surgery + RT + immunotherapy | 2 (1) |
| Surgery + chemotherapy | 1 (1) |
| RT only | 31 (23) |
| RT + chemotherapy | 1 (1) |
| RT + immunotherapy | 1 (1) |
| None | 3 (2) |
| Number of patients who underwent surgery | 101 (74) |
| Type of surgery | |
| Parotidectomy + neck dissection | 48 (48) |
| Parotidectomy + lumpectomy | 13 (13) |
| Neck dissection only | 21 (21) |
| Parotidectomy only | 7 (7) |
| Other surgery | 12 (12) |
| Location site of the metastasis | |
| Parotic gland | 49 (49) |
| Region I | 20 (20) |
| Region II | 32 (32) |
| Region III | 12 (12) |
| Region IV | 3 (3) |
| Region V | 15 (15) |
| Overall survival 2 years | |
| After primary tumour | 76/135 |
| After regional metastases | 51/123 (41) |
| After distant metastases | 7/29 (24) |
| Overall survival 2 years after primary diagnosis | |
| Surgery, no RT | 12/23 |
| Surgery + RT | 54/77 (70) |
| RT, no surgery | 10/32 |
| No treatment | 0/3 (0) |
| Overall survival 2.5 years | |
| After primary tumour | 68 /135 |
| After regional metastases | 45/123 (37) |
| After distant metastases | 5/29 (17) |
| Overall survival 2.5 years among immunosuppressed | |
| After primary tumour | 14/34 (41) |
| After regional metastases | 9/30 (30) |
| After distant metastases | 2/8 (25) |
| Overall survival 2.5 years after primary diagnosis | |
| Surgery, no RT | 11/23 |
| Surgery + RT | 49/77 (64) |
| RT, no surgery | 9/32 |
| No treatment | 0/3 (0) |
| Dead in July 2023 | 109/137 (80) |
| Dead in July 2023 among immunosuppressed | 30/34 (88) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNonmelanoma Skin Cancer Studies · Cancer Diagnosis and Treatment · Cutaneous Melanoma Detection and Management
Cutaneous squamous cell carcinoma (cSCC) is the second most common cancer in Sweden and its incidence is increasing rapidly. In Sweden during 2023, over 12,000 new cases of cSCC were reported and its incidence is calculated at 137 new cases per 100,000 people for men and 107 for women (1). Cumulative UV radiation, old age, and male sex are the most important risk factors for developing cSCC (2–8). The increasing incidence is believed to be caused by an ageing population and increased exposure to UV radiation. Approximately 80% of cSCC cases are localized to the head and neck region, accounting for a large proportion of consultations in the ENT department (5, 8–10).
For the majority of patients, the disease is easily treated by surgical excision. Unfortunately, 1.5–5% of cSCC metastasize and in these cases the patients’ prognosis worsens radically (11–22).
Risk factors for developing metastatic cSCC (mcSCC) include tumour size ≥ 2 cm, invasion depth, degree of differentiation, perineural invasion, intravascular invasion, subcutaneous invasion, immunosuppression, tumour relapse, and tumour location (11, 14, 15, 19, 23–30). In the national guidelines of Sweden, the Brigham and Women’s Hospital (BWH) staging system is used to identify high-risk tumours postoperatively (16, 31). For mcSCC the TNM-system (UICC 8) is used.
The great majority of metastases occur within the first 2 years after the diagnosis of the primary tumour and most often affect the parotid gland or the lymph nodes of the neck (14, 15, 18–20, 26, 32, 33). A literature review from 2018 stated that disease-specific 5-year survival was between 58% and 83% and a large Australian retrospective cohort from 2024 showed a 5-year Disease Specific Survival (DSS) of 77.6% (22, 34). There is currently no reported survival rate in Sweden, but unpublished Swedish data point towards a 52% overall survival within 18 months, which is similar to the results of a recent Finnish study by Knuuttila et al. (18). Little is known about mcSCC in Sweden as it is not recorded in a national registry as a unique diagnosis and no recent studies have been published.
As we expect an even higher incidence of cSCC in the future we can assume that mcSCC will cause a significant patient burden in ENT cancer departments. In this study we aim to describe the patient characteristics, tumour characteristics, treatment, and outcome of Swedish patients with mcSCC in Stockholm region during the study period 2012–2020.
MATERIALS AND METHODS
The study was approved by the Swedish ethical committee. Stockholm region’s charting system Take Care was searched for adult patients who were diagnosed with metastasized or locally advanced cSCC between 2012 and 2020. The charting system was searched for the ICD-10 diagnostic code C44 (skin tumour) in combination with C77 (lymph node metastases) and C44 in combination with surgical codes ELB40 (parotic resection), ELB50 (parotidectomy), or PJD51 (neck dissection). Patients were included if they had cSCC in the head and neck area and locally advanced or metastatic disease. Their medical records were reviewed, and data (see list of variables in Table I) were collected.
RESULTS
The search identified 309 patients of whom 172 were excluded because they had cancer diagnoses other than cSCC, their primary tumours were located outside the head and neck area, or they were treated for their metastasized or locally advanced cSCC at a hospital outside of the study period or outside of the Stockholm region. This resulted in 137 patients who were included in the study.
Patient characteristics
The average age at the time of the primary tumour diagnosis was 80 years (81 median). On average each patient had 3.4 comorbidities; 70% had a WHO performance status of 0–1 and 30% 2–4. The remaining patient characteristics are summarized in Table I.
Primary tumour characteristics
In 2/137 cases the primary tumour was unknown, resulting in 135 primary tumours to analyse. According to the BWH system 50% were classified as high-risk tumours after the primary surgery. The remaining tumour characteristics are summarized in Table II.
Metastases characteristics
The average time between diagnosis of the primary tumour and the diagnosis of regional metastases was 11 months and median time 7 months; 90% of the metastases were diagnosed within 2 years. The average time between the diagnosis of the primary tumour and the diagnosis of distant metastases was 26 months and median time 16 months. The average and median age at the diagnosis of regional metastases was 82 years. The average and median age at the time of distant metastases was 81 and 82 years respectively. The average and median disease-free survival (DFS) was 11 and 6 months respectively. The remaining characteristics of the metastases are summarized in Table III.
Treatment
A total of 101 patients received surgery due to regional metastases or locally advanced disease, 76% (94/123) of those with regional metastases and 78% (7/9) of those with locally advanced tumours. Radical excisions were performed in 45% (45/101) of the surgeries. 80% (110/137) of the patients had radiotherapy (RT); 14% (19/137) had chemotherapy; 4% (5/137) had immunotherapy. The patients’ treatments are shown in Fig. 1. The rest of the treatment data are summarized in Table IV.
Treatment.
Outcome
At the end of the study period (July 2023) an 80% (109/137) mortality rate was seen in the study population. Among the immunosuppressed an 88% (30/34) mortality rate was seen. Average time between the primary diagnosis of cSCC and death was 33 months and median 22 months. Average time between the identification of regional metastases and death was 21.5 months and median 13 months. Average time between diagnosis of distant metastases and death was 14 months and median 5 months; 51% (56/109) of the deaths were determined to be directly related to the cSCC diagnosis. In 18 cases the cause of death was unknown. Excluding unknown causes of deaths, 62% (56/91) of the deaths were assessed to be caused by cSCC. Other outcomes are summarized in Table V.
DISCUSSION
Cutaneous SCC is the second most common cancer in Sweden, its incidence is increasing, and metastasized disease has a high mortality rate. This is the first published study on mcSCC in Sweden and reports descriptions of this disease.
The most common sites of primary tumours among mcSCC in Sweden were ear and temple. This is similar to studies from other countries (11, 18).
The median age of the patient group was 81 but 70% were assessed as WHO-performance status 0-1, indicating that these patients are elderly but relatively healthy at the time prior of the treatment. Despite this, overall survival after 2.5 years from diagnosis of regional metastases was only 37%, which suggests the aggressiveness of the disease and/or the lack of effective treatment. With immunosuppression the prognosis is even worse.
In Sweden the BWH system is used to identify high-risk primary tumours. Other studies have reported a low sensitivity but a high specificity of the BWH system (16, 35–37). Knuuttila et al. could not find a correlation between BWH and prognosis (18). In our study only 50% of the primary tumours were assessed as BWH high-risk, which supports these other studies’ results reporting its low sensitivity. We encourage the development of a more sensitive risk stratification system to find high-risk primary cSCC.
Median time between primary tumour and regional metastases was 7 months and 90% of the metastases were diagnosed within 2 years. This data is in line with earlier studies, including Knuuttila et al., which reported 6.6 months and 85% respectively (13, 14, 18, 21, 26, 32, 38). This suggests that close monitoring of patients during the first 2 years following a high-risk cSCC is essential for the early detection of metastases.
Most metastases were located in the parotic gland and region I–II, which concurs with earlier studies (13). 58% of our patients were classified as TNM stage IV after their surgery. The majority (87%) were due to clinically extracapsular growth of the metastases. Ebrahimi et al. found that 81% of their study population had metastases with extracapsular growth and that this significantly affected the patient outcome. However, they suggested that the presence of extracapsular growth upstaged too many patients to TNM stage IV, despite many having curable disease (34).
The patients received different combinations of treatment, mostly surgery with adjuvant radiotherapy. Chemotherapy and immunotherapy were never given as single therapy, but were given as an addition to surgery and/or radiotherapy. The highest overall survival was among the patients receiving surgery + radiotherapy, where 64% were alive 2.5 years after the primary diagnosis. The overall survival was 48% for patients who received only surgery and 28% for those who received only radiotherapy. Obviously, the patient’s comorbidities and level of functioning are taken into consideration when choosing which treatment a patient will receive, but our results suggest a higher mortality rate without surgery. Earlier studies have also shown better prognosis if patients receive both surgery and radiotherapy compared with surgery alone (21, 34, 39).
Our overall survival rate (OS) at 2 years was 56% from primary tumour diagnosis and 41% from metastases diagnosis. These numbers are similar to the results of Knuuttila et al. where 2-year OS from primary tumour diagnosis and metastases diagnosis was 63.8% and 43.4% respectively (18). Other studies have shown OS at 2 years of 50–66% from time of metastases (32, 38).
Study limitations are mostly related to those expected in a retrospective cohort study. Some data were missing, and patients may have not been identified due to incorrect ICD coding of patients during treatment. Some patients may never have been referred to a hospital for treatment but rather received palliative treatment at home. Cause of death was rarely confirmed by autopsy and was therefore difficult to relate to the cSCC diagnosis. Another limitation is that only 4% of our patients received immunotherapy as this was not part of the European guidelines during the study period. Given that 32% of the patients had a medical history of a previous cSCC, the tumour defined as the primary source of metastasis may have been incorrectly identified.
Conclusion
Our study, which is the first reported in the Swedish population, shows that mcSCC occurs in elderly but otherwise generally healthy patients, that primary tumours with a high risk of causing mcSCC seem hard to identify, and that metastases occur within 2 years after primary tumour diagnosis. The patient group overall has a high mortality rate, particularly among those who do not undergo surgery. We encourage the development of a more sensitive risk stratification system to find high-risk primary cSCC, and close monitoring of patients during the first 2 years following a high-risk primary cSCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Socialstyrelsen. Statistikdatabas för cancer 2023. Available from: https://sdb.socialstyrelsen.se/if_can/resultat.aspx
- 2de Gruijl FR. Skin cancer and solar UV radiation. Eur J Cancer 1999; 35: 2003–2009. 10.1016/S 0959-8049(99)00283-X 10711242 · doi ↗ · pubmed ↗
- 3Rigel DS. Cutaneous ultraviolet exposure and its relationship to the development of skin cancer. J Am Acad Dermatol 2008; 58: S 129–S 132. 10.1016/j.jaad.2007.04.03418410798 · doi ↗ · pubmed ↗
- 4Armstrong BK, Kricker A. The epidemiology of UV induced skin cancer, J Photochem Photobiol B 2001; 63: 8–18. 10.1016/S 1011-1344(01)00198-111684447 · doi ↗ · pubmed ↗
- 5Xiang F, Lucas R, Hales S, Neale R. Incidence of nonmelanoma skin cancer in relation to ambient UV radiation in white populations, 1978–2012: empirical relationships. JAMA Dermatol 2014; 150: 1063–1071. 10.1001/jamadermatol.2014.76225103031 · doi ↗ · pubmed ↗
- 6Green AC, Olsen CM. Cutaneous squamous cell carcinoma: an epidemiological review. Br J Dermatol 2017; 177: 373–381. 10.1111/bjd.1532428211039 · doi ↗ · pubmed ↗
- 7Marks R, Staples M, Giles GG. Trends in non-melanocytic skin cancer treated in Australia: the second national survey. Int J Cancer 1993; 53: 585–590. 10.1002/ijc.29105304108436431 · doi ↗ · pubmed ↗
- 8Dal H, Boldemann C, Lindelof B. Trends during a half century in relative squamous cell carcinoma distribution by body site in the Swedish population: support for accumulated sun exposure as the main risk factor. J Dermatol 2008; 35: 55–62. 10.1111/j.1346-8138.2008.00416.x 18271799 · doi ↗ · pubmed ↗