A cross-sectional analysis of all vena cava filter placement over 9-years in Brazil: trends and mortality rates in a population of over 200 million
Clara Sanches Bueno, Hedra Marques Santos, Júlia Freire Castanheira, Bruno Jeronimo Ponte, Felipe Soares Oliveira Portela, Marcelo Fiorelli Alexandrino da Silva, Marcelo Passos Teivelis, Alexandre Fioranelli, Nelson Wolosker

TL;DR
This study analyzes vena cava filter placement trends and mortality in Brazil over nine years, highlighting disparities between public and private healthcare systems.
Contribution
The study provides the first nationwide analysis of vena cava filter use in Brazil’s dual healthcare system.
Findings
The private sector performed 57% of vena cava filter procedures despite covering only 25% of the population.
The Southeast region accounted for 70% of private procedures and 40.5% of public procedures.
Mortality rates were similar between public and private systems (6.7% vs. 7.4%).
Abstract
•The private sector performs the majority of procedures despite serving a minority of the population.•National procedure volume more than doubled (140% increase) in almost a decade.•The Southeast region is responsible for 70% of all private procedures. The private sector performs the majority of procedures despite serving a minority of the population. National procedure volume more than doubled (140% increase) in almost a decade. The Southeast region is responsible for 70% of all private procedures. Venous Thromboembolism (VTE) is a major global health concern, with Vena Cava Filters (VCFs) serving as an alternative to anticoagulation in high-risk patients. Brazil’s VCF trends remain understudied, particularly in its dual public-private healthcare system. This database study allows a broad overview of the Brazilian healthcare landscape. This cross-sectional nationwide analysis used…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
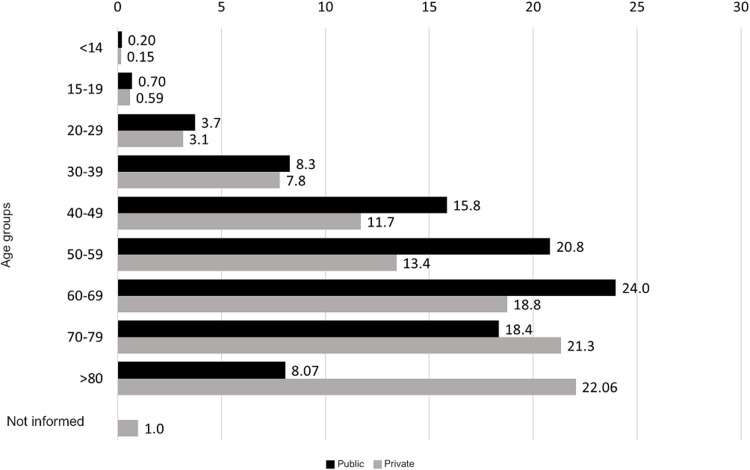 Figure 1
Figure 1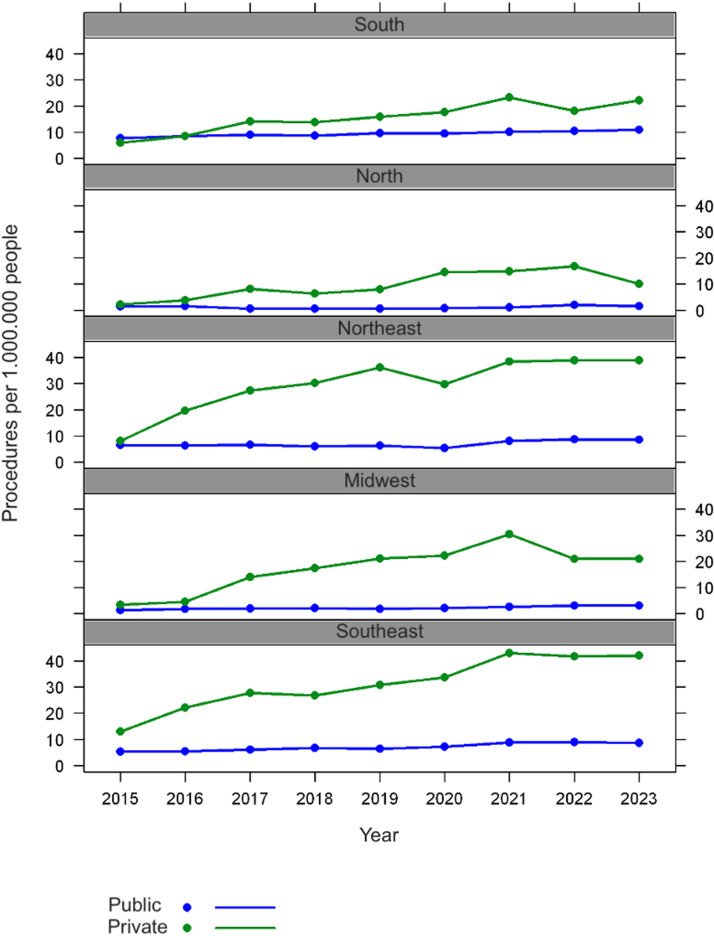 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Atrial Fibrillation Management and Outcomes · Central Venous Catheters and Hemodialysis
Introduction
Venous Thromboembolism (VTE), which includes Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE),1 represents a significant global health burden, with an estimated 5% lifetime prevalence in adult populations.2 The rising incidence of VTE reflects demographic and epidemiological transitions, including aging populations, increasing prevalence of obesity, sedentary lifestyles, and enhanced diagnostic sensitivity through advanced imaging techniques and biomarker assays.3^,^4 Anticoagulation therapy remains the gold standard of VTE treatment. However, Vena Cava Filters (VCF) are an important alternative for specific scenarios, such as when a patient has acute VTE and an absolute contraindication to anticoagulation or when recurrent PE occurs despite adequate anticoagulant therapy.5, 6, 7
Although the placement of VCFs is a minimally invasive, percutaneous procedure, it is not risk-free. Rare but potentially serious complications can occur, such as filter migration, venous wall penetration, and adjacent organ involvement (e.g., duodenal perforation).8 Historically, there has been a trend in the United States toward the overuse of VCFs, with studies indicating that over 50% of procedures were for questionable indications in the early 2000s.9 In contrast, studies from the same period in Brazil did not show this trend; VCF placement there was more selective and based on well-established criteria.10
Brazil's universal healthcare system, known as Sistema Único de Saúde (SUS), is a publicly funded program designed to provide full-spectrum medical care to all citizens.11 Although the constitution guarantees free healthcare access to all citizens, around 25% of the population opts for additional private health services (Private), often funded through employer-sponsored plans. As a result, approximately 75% of Brazilians rely exclusively on the public healthcare system.12
The Public system maintains a national anonymized database that tracks surgical procedures, including all VCF implantations performed in public hospitals. Recently, data on procedures performed within the Private has become publicly available, covering interventions from 2015 to 2023. This new information allows for comparative studies between public and private healthcare systems and provides a broad overview of the Brazilian healthcare landscape. The analysis does not include only out-of-pocket payment data, which represent a minority of expenditures (less than 5%).13 Consequently, it enables a thorough assessment of the utilization of VCF in Brazil.
Notably, no population-level study on raw data (as opposed to estimation-based) has yet evaluated VCF placement across an entire nation. Globally, the most extensive analysis of VCF use comes from the U.S. Nationwide Inpatient Sample (NIS), which provides estimates based on a stratified 20% sample of discharges from hospitals participating in the Healthcare Cost and Utilization Project (HCUP).14^,^15 In Brazil, while some studies have examined VCF placement using SUS databases, none have encompassed both Public and Private datasets, leaving a gap in understanding the full scope of procedural trends, disparities, and outcomes.10^,^16
Our study represents a significant advancement by offering the first complete national assessment of VCF utilization patterns, covering all 26 states of this continental-scale nation. Our analysis uniquely incorporates data from both the Public and Private. This approach enables unprecedented insights into large-scale VCF implementation across diverse healthcare subsystems.17
Objectives
To study all cases requiring VCF placement in Brazil, within the Public and Private, from 2015 to 2023, using a big data system. The authors intended to analyze variations in the number of procedures over time, trends by geographic region, patient characteristics, and in-hospital mortality rates.
Materials and methods
This retrospective population-based study analyzed publicly available data from the TabNet platform, of the Department of Informatics of the Unified Health System (DATASUS) and from the Private (D-TISS). TabNet provides open-access data on procedures performed in the Public system, which accredited hospitals must report for reimbursement. Similarly, the platform (D-TISS), managed by the National Supplementary Health Agency (ANS), provides open-access procedure data for the Private health system, excluding out-of-pocket payments.
This research was deemed exempt by the institutional ethics committee and was institutionally registered under the number 10337 (Sistema Gerenciador de Projetos de Pesquisa, SGPP). All data provided by TabNet and D-TISS are anonymous and publicly available. For this reason, the Institutional Review Board (Conselho de Revisão Institucional) waived the requirement for informed consent forms. This study was conducted in accordance with the STROBE statement.18
Data on VCF placement were collected from both platforms (TabNet and D-TISS), covering a 9-year period from 2015 to 2023, excluding 2024 due to incomplete DATASUS data for the period. The collected data included geographic region, the number of procedures performed, and in-hospital mortality rates. Statistics on in-hospital deaths were selected from the hospital mortality sections of TabNet and D-TISS. The data was grouped by geographic region and distributed over the years.
For data extraction within Public, the authors used a specific code assigned to this procedure established by the Public Procedure, Medicine, and OPM Management System (SIGTAP): 04.06.04.014–1. Data collection for the Private was obtained from the D-TISS Data Panel, published by ANS, and procedures were analyzed according to the Private coding system, which includes Vena Cava Filter (VCF) placement (code 30907080) and VCF implantation for pulmonary embolism prevention (code 40813240).
The steps for data collection, platform field selection, and Table adjustment were performed using the selenium-webdriver packages (v. 3.1.8, Selenium HQ, several collaborators worldwide) and pandas (v. 2.7.13, Lambda Foundry, Inc., and PyData Development Team, New York, USA). The Mozilla Firefox browser (v. 59.0.2, Mountain - California - USA) and geckodriver webdriver (v. 0.18.0, Mozilla Corporation, Bournemouth, England) were used. Following collection and treatment, all data were organized and grouped in a spreadsheet using Microsoft Office Excel 2016® (v. 16.0.4456.1003, Redmond - Washington - USA) software. These computer programs allowed automated content access (web scraping), the automated navigation codes were programmed in Python language (v. 2.7.13, Beaverton - Oregon - USA) using the Windows 10 Single Language operating system.
The examined variables included the total number of procedures, patient demographics (gender and age distribution), regional disparities in service provision, and associated mortality rates. For statistical analysis, generalized linear models with a Gamma distribution19 were performed to assess the relationship between the rate of procedures and average values with year, source of procedures (public or private), and region. For the death rate, a generalized linear model with a Poisson distribution was used, with the number of procedures as an offset. The results were presented as rate ratios, 95% Confidence Intervals, and p-values. The analyses were performed using R, version 4.1.1 (R Core Team. R: A Language and Environment for Statistical Computing. 2024. R version 4.4.1).
Results
Between 2015 and 2023, a total of 21,630 CVF procedures were performed in Brazil, distributed between the Public and the Private. During this period, the Private system accounted for 57% (12,323) of all procedures, while the Public system accounted for 43% (9307). Notably, despite Private covering only 25% of the population, it performed a significantly higher proportion of CVF procedures (Table 1).12Table 1. Absolute number of CVF procedures performed and incidence per 1 million beneficiaries in Public and Private health system between 2015 and 2023.Table 1 dummy alt textYearnPublic UsersIncidencenPrivate UsersIncidence2015819154,358,5995.3150148,045,04310.432016864157,552,5135.4888546,319,41219.112017932159,814,8185.83119545,396,73926.322018947161,386,0875.87120245,142,95126.632019965162,907,5495.92141344,992,55031.412020978164,004,4125.96149345,160,47733.0620211234163,553,1697.54193046,550,47341.4620221296162,944,5857.95183247,918,39838.2320231272162,943,7377.81187248,751,42138.40Average1034161,051,7196.42136946,475,27429.45
Analyzing the incidence of CVF procedures per 1 million beneficiaries (Table 1), the private system exhibited a consistently higher incidence rate (average of 29.45 per 1 million beneficiaries) compared to the public system (average of 6.42). While the absolute number of procedures in the public system showed moderate growth (from 819 to 1272), the private system experienced a sharp increase (from 501 to 1872), peaking in 2021 (incidence: 41.46). Notably, the public system’s incidence rose during the pandemic (7.45 in 2021).
A predominance of women was observed in CVF procedures across both systems (Table 2). In Public, out of 9307, 59.15% were women (5506 cases) and 40.84% men (3801 cases). In Private (12,323), 56.25% were women (6932 cases) and 42.75% men (5268 cases). Overall, of 21,507 procedures with reported gender, 57.83% were women (12,438 cases) and 42.17% were men (9069 cases). Gender was unreported in only 123 cases (0.57%).Table 2. Distribution by sex of CVF placement.Table 2 dummy alt textSexPublicPrivateTotaln%n%n%Men380140.84526842.75906941.93Women550659.15693256.2512,43857.5Not informed12311230.57
Fig. 1 presents the age distribution of procedures in Public and Private. In the Public system, the largest share (23.98%) fell in the 60‒69-year-old group. By contrast, in Private, the over-80-year-old cohort accounted for the highest proportion (2718 cases; 22.06%), versus 751 Public cases (8.07%). Additionally, 122 Private procedures (0.99%) lacked age data.Fig. 1. Distribution by age group of procedures carried out in Public and Private healthcare systems.Fig 1 dummy alt text
Table 3 presents the procedures performed by region. In Public, the Southeast led with 3771 procedures (40.518%), followed by the Northeast with 3074 (33.029%). In Private, the Southeast region again dominated with 8620 procedures (69.950%), then the Northeast with 1942 (15.759%), and the South with 1033 (8.383%).Table 3. Procedures by region of the country.Table 3 dummy alt textRegionPublicPrivateTotaln%n%n%North1281.381631.322911345Northeast307433.031.94215.76501623,190Midwest3323.575654.588974147Southeast377140.528.62069.9512,39157,286South200221.5110338.38303514,031Total9307100.0012,323100.0021,630100,000
Both systems show a predominance of procedures in the Southeast, substantial contributions from the Northeast and South, and minimal activity in the Midwest and North, a pattern consistent over time in the Brazil areas with the lowest demographic density (Fig. 2).Fig. 2. Procedures per 1.000.000 people.Fig 2 dummy alt text
The adjusted model for the procedure rate, accounting for the region of origin, shows a significant change over the years (p-value < 0.001), with an estimated annual increase of 11% in the rate. Regarding the source of care, the procedure rate under Private is estimated to be 4.357 times higher than Public (p-value < 0.001) (Table 4).Table 4. Procedure rate for 1.000.000 patients.Table 4 dummy alt textMean rate (95% CI)p-valueYear1.110 (1.074; 1.149)<0.001Source PublicReference Private4.357 (3.654; 5.193)<0.001Region SoutheastReference Midwest0.424 (0.325; 0.553)<0.001 Northeast0.971 (0.745; 1.267)0.831 North0.225 (0.172; 0.294)<0.001 South0.931 (0.712; 1.218)0.600 Not adjusted by regionSource PublicReference Private3.652 (2.883; 4.626)<0.001CI, Confidence Interval.
Analyzing the mortality associated with VCF implantation procedures (Table 5), overall rates were 7.4% in Private (918/12,323 procedures) versus 6.7% in Public (625/9307 procedures). In Public, regional mortality rates ranged from 3.1% in the North to 12.7% in the Midwest; in Private, from 3.7% in the North to 8.1% in the Northeast. The largest Public-Private disparity appeared in the Midwest (12.7% vs. 6.4%). In both the Southeast (7.0% vs. 7.4%) and South (6.7% vs. 7.4%) Private rates were slightly higher than Public.Table 5. Absolute and relative distribution of deaths of patients undergoing surgical treatment per region for CVF placement in the SUS and PHS.Table 5 dummy alt textRegionPublicPrivateProceduresDeathsMortality rateProceduresDeathsMortality rateNorth12843.116363.7Northeast30741815.919421588.1Midwest3324212.7565366.4Southeast3771264786206427.4South20021346.71033767.4Total93076256.7212,3239187.45
However, the adjusted model for the mortality rate showed no evidence of differences between healthcare sources (public vs. private, p-value = 0.066) and no significant change over the years (p-value = 0.053). A lower mortality rate in the North region compared to the reference region was noted (Table 6).Table 6. Mortality rate per 1.000 procedures.Table 6 dummy alt textMean rate (95% CI)p-valueYear1.020 (1.001; 1.041)0.056Source PublicReference Private1.086 (0.975; 1.209)0.134Region SoutheastReference Midwest1.191 (0.937; 1.490)0.139 Northeast0.952 (0.836; 1.082)0.453 North0.474 (0.237; 0.835)0.019 South0.978 (0.836; 1.139)0.779 Not adjusted by regionSource PublicReference Private1.100 (0.994; 1.219)0.066CI, Confidence Interval.
Discussion
This retrospective study utilizes population data from TabNet (DATASUS) and D-TISS (ANS) to assess trends in VCF use in Brazil. Rather than analyzing a sample, it covers a great part of the Brazilian population over nine years from 2015 to 2023. It is the first study to analyze the entire population of a continental developing country.
A total of 21,503 VCFs were placed during this period: 9307 in Public and 12,196 in Private. While Public averaged 6.42 procedures per 1 million beneficiaries, Private ‒ serving only 25% of the population ‒ had a fivefold higher rate (29.45 per 1 million). This contrasts with U.S. data for Medicare beneficiaries, which showed a decrease from 1578.0 to 641.0 per million (2010 and 2021)20 due to stricter guidelines - yet peak U.S. rates were still 20 times higher than Brazil's private system.
There is no nationwide epidemiological study to compare Brazilian rates with other Low-Middle Income Countries (LMIC), in India there is only one study from a tertiary referral center that indicates stricter use, adherent to absolute indications for usage in most cases, only 31 cases were analyzed.21 Market data from South Africa shows a trend in growing device use, baseline country-wide rates are unavailable.22 The absence of multi-center or population-level data from LMICs comparable to Brazil´s national registry limits cross-country analyses.
This disparity reflects more fragile health information systems and chronic funding constraints, consequences of deeper structural and systemic challenges that hinder the collection and consolidation of health data. This context places Brazil in a unique position, as the existence of its national registry, despite its own limitations, represents a rare source of data among its peer nations.
European data show intermediate usage: in 2012, the “Big Five” nations (France, Germany, Italy, Spain, and the UK) reported 9070 VCF placements or 28 per million.23 These contrasts reflect major differences in clinical practice across healthcare systems.
The fivefold disparity in VCF rate between Private and Public may reflect distinct scenarios: overutilization in the private sector, where financial incentives could drive unnecessary procedures, or unmet clinical need in the public system, where resource constraints may limit access to appropriate interventions, not seen in private where insured patients generally access endovascular procedures more easily, as high-resolution imaging and endovascular surgery are more available in private centers.24 Without indication-specific data, however, this critical distinction remains unresolved, highlighting the need for future studies.
VCF placement requires a team trained in endovascular surgery, predominantly available in private or private-affiliated hospitals. Within the public sector, high-complexity services are less available, particularly in the North and Northeast regions, limiting access to such procedures.25
Private healthcare systems typically operate under reimbursement models that may encourage more procedures. Although no direct evidence confirms financial drivers for VCFs in Private, fee-for-service models likely affect decisions, unlike the Public’s limited budget.26 Demographics in the Private population (older, more comorbid, higher socioeconomic status) might slightly influence VTE risk, but these factors alone do not explain the large gap in VCF usage.27^,^28
Recent trends in VCF placement show a clear contrast between the United States and Brazil. In the U.S., VCF use significantly declined after FDA alerts in 2010 and 2014, and the implementation of stricter guidelines aimed at correcting overuse and emphasizing filter retrieval, dropping among Medicare beneficiaries from 1578 to 641 insertions per 1 million between 2010 and 2021.20 Conversely, Brazilian data from 2015 to 2023 indicate a general upward trend in both the absolute number of procedures (Private + Public, from 1320 in 2015 to 3144 in 2023) and in rates per million inhabitants, particularly in the private healthcare sector, which rose from 10.18 to 38.34 per million, and also in Public, which increased from 5.31 to 7.81 per million, with a more pronounced increase from 2021 onwards.
Several hypotheses can explain these trends. Firstly, Brazil began with a considerably lower VCF usage baseline than the U.S., and its 140% increase over eight years might reflect an expansion of access to appropriate technology as its healthcare system evolves. Secondly, a rising incidence of VTE, possibly worsened by the COVID-19 pandemic and its known VTE risk, may also have contributed to the post-2021 surge.29
During the early COVID-19 pandemic (2020), the increased risk of VTE in critically ill patients led to some cases of early and increased use of VCF.30 As clinical experience grew (2021‒2022), therapeutic anticoagulation became established as the primary strategy, significantly reducing VTE incidence and mortality.31^,^32 Consequently, VCF use returned to traditional indications (anticoagulation failure or contraindications), leading to stabilization in utilization rates.33 Our findings align with this trend, showing peak usage in 2020 followed by stabilization higher level than the previous baseline.
The extent to which this increased usage represents overuse versus appropriate utilization remains uncertain, as specific implantation indications were not examined. Notably, implantation rates in Brazil's public healthcare system remained substantially lower than both U.S. and European benchmarks throughout the study period.20^,^23 While private sector implantation rates increased post-pandemic, they remained well below levels observed in systems with known overuse tendencies like the U.S. The slightly higher rates compared to European countries may reflect limited availability of recent European data rather than true overutilization.
A clear finding is that VCF procedures were more frequent in women, who accounted for 57.50% (n = 12,438) of all VCF placements, versus 41.93% (n = 9069) in men. This trend was observed in both healthcare settings: 59.16% in Public and 56.25% in Private. These consistent results suggest that the conditions requiring VCFs are more prevalent in women, independent of healthcare coverage.10^,^34
This finding may reflect an increased risk of PTE in women exposed to hormonal contraceptives, pregnancy, postpartum, or hormone replacement therapies.10^,^20
VCF placement is primarily age-associated, with approximately 74% of procedures in patients aged 50 or older. This trend is attributed to the higher risk of PTEdue to chronic conditions like cancer and kidney disease.35, 36, 37 Additionally, older individuals often experience mobility limitations, especially following major surgeries, and frequently use medications that affect coagulation, such as hormone replacement therapies and oncological treatments.5
Age group analysis reveals differences between Public and Private. In Public, procedures concentrate in ages 60‒69 (23.98%), and 50‒59 (20.82%). In Private, the distribution skews older, with 80+ (22.06%) and 70‒79 (21.34%) as the leading groups. The predominance of very advanced age groups (> 70 and particularly > 80-years) in the Private may suggest that individuals with higher socioeconomic status, who are more likely to have private health insurance and greater longevity, seek or have facilitated access to specific procedures within the private sector during this life stage. In contrast with Public patients witch frequently have a low-income status and may have reduced longevity.
An analysis of the regional distribution of healthcare procedures in Brazil reveals that the Southeast region accounts for most procedures, with 40.5% in the Public and 70% in the Private. This concentration can be attributed to the region's higher population density, widespread availability of supplementary health plans, and disproportionate share (51.9%) of the nation's vascular surgeons, representing one of the highest specialist densities per 100,000 inhabitants nationally.28 In contrast, the Midwest and North regions account for less than 5% of Public procedures and 6% of Private procedures, while containing only 3.0% and 9.7% of vascular surgeons, respectively (lowest per capita concentrations nationally). This highlights significant gaps in healthcare access, also reflecting demographic void. These disparities may lead to patients needing to travel interstate for complex cases and could necessitate the placement of VCFs.
The comparative analysis of in-hospital mortality following VCF placement in Brazil (2015‒2023) indicates that although the Private performed more procedures and consequently recorded a higher absolute number of deaths, its mortality rate was generally higher than that of the Public (7.42% vs. 6.63%). In 8- of 9-years analyzed, Private rates exceeded those of Public (2022 was the exception, and 2017 showed similar rates). Both systems exhibited fluctuations and peaks ‒ especially between 2020 and 2022 - likely influenced by the COVID-19 pandemic. However, these raw figures do not account for confounders such as case severity and complexity, differing eligibility criteria, and patient demographics. For example, Private patients may have access to more complex procedures or be transferred in a more critical condition, they may also have more comorbidities and cancer, while Public patients might face delayed access to care. Consequently, any inference about care quality requires a risk-adjusted analysis, which is currently unfeasible due to unavailable data. The lack of data on specific in-hospital mortality (VTE-related, procedure-related, or related to the underlying condition ‒ e.g., advanced malignancy, major trauma) remains unknown, further limiting the interpretability.
Overall, the in-hospital mortality rate for VCF placement is similar in both systems (6.7% in Public vs. 7.4% in Private). These rates largely reflect patients’ underlying severe conditions (e.g., VTE, cancer, or trauma), whereas mortality directly attribuTable to the VCF implantation procedure itself is usually below 1%,8^,^38 as shown in systematic reviews and clinical trials such as PREPIC.19^,^39 Direct comparisons across studies are complex due to variations in patient profiles, filter types, indications (therapeutic vs. prophylactic), and the definitions and follow-up periods for mortality. Regional variations observed in Brazil (Public rates ranging from 3.1% to 12.7% and Private rates from 3.7% to 8.1%) also suggest the influence of local factors and specific characteristics of each region’s population.
The mortality rates in Brazil between 2015 and 2023 find parallels in international studies for severe cohorts. In a large observational study in the USA (SAFE-IVC, with Medicare data from 2013‒2021) found a 30-day all-cause mortality rate of 14.6% in patients who received VCF; Brazil’s 6.7% and 7.4% rates are lower.20
Limitations
This study has several limitations inherent to the use of aggregated administrative databases (DATASUS and D-TISS), including susceptibility to coding errors, reporting inconsistencies, and potential misclassification or underreporting. Data anonymization prevented longitudinal tracking, precluding identification of unique patients and hindering analyses of multiple procedures per individual (e.g., implantation, retrieval, reintervention). Inconsistent coding and the absence of patient-level variables (e.g., VTE severity, filter indication/type, comorbidities, socioeconomic status, complications) limited risk adjustment and assessment of evidence-based appropriateness. Furthermore, the lack of follow-up data made it impossible to evaluate long-term outcomes such as PE recurrence or retrieval rates. Age-stratified data for the private sector were unavailable, and out-of-pocket procedures, although likely infrequent, were not captured, introducing possible residual bias. Together, these limitations constrain our ability to assess adherence to clinical guidelines and evaluate long-term safety.
Despite this, the study offers a novel, comprehensive nationwide overview of VCF utilization in Brazil (2015–2023) across both public and private healthcare systems. By consolidating official data, it provides valuable real-world insights into differences in procedure volumes, thereby contributing to a better understanding of clinical practice and financing of this technology in the country. Looking ahead, future enhancements to the database, potentially including metrics such as filter retrieval rates and the specific clinical indications for implantation, could further strengthen the evidence base for guiding health policy in this field.
Conclusions
In this analysis, based on real-world data from 2015 to 2023, a total of 21,630 VCF implantation procedures were performed in Brazil. This resulted in an average annual rate of 1.16 procedures per 10,000 inhabitants, considering the combined estimated populations covered by the Public and the Private.
The procedure rate per 10,000 inhabitants in the Private was 4.25 times higher than in the Public.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
CRediT authorship contribution statement
Clara Sanches Bueno: Writing – original draft, Formal analysis. Hedra Marques Santos: Writing – original draft, Formal analysis. Júlia Freire Castanheira: Writing – original draft. Bruno Jeronimo Ponte: Data curation. Felipe Soares Oliveira Portela: Data curation. Marcelo Fiorelli Alexandrino da Silva: Writing – review & editing. Marcelo Passos Teivelis: Writing – review & editing. Alexandre Fioranelli: Writing – review & editing. Nelson Wolosker: Writing – review & editing, Supervision, Visualization.
Conflicts of interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takara N.C.da Costa Ferreira N.Murakami B.M.Lopes C.T.Development and validation of an informative manual on venous thromboembolism for the lay population Einstein 182020 Eao 5425(São Paulo)3293582710.31744/einstein_journal/2020 AO 5425 PMC 7480492 · doi ↗ · pubmed ↗
- 2Spencer F.A.Emery C.Lessard D.The worcester venous thromboembolism study J Gen Intern Med 21720067227271680877310.1111/j.1525-1497.2006.00458.x PMC 1924694 · doi ↗ · pubmed ↗
- 3Heit J.A.Spencer F.A.White R.H.The epidemiology of venous thromboembolism J Thromb Thrombolysis 41120163142678073610.1007/s 11239-015-1311-6PMC 4715842 · doi ↗ · pubmed ↗
- 4Wendelboe A.Weitz J.I.Global health burden of venous thromboembolism Arterioscler Thromb Vasc Biol 4452024100710113865703210.1161/ATVBAHA.124.320151 · doi ↗ · pubmed ↗
- 5Konstantinides S.V.Meyer G.Becattini C.2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS)Eur Heart J 41420205436033150442910.1093/eurheartj/ehz 405 · doi ↗ · pubmed ↗
- 6Leiderman D.B.D.Zerati A.E.Vieira Mariz M.P.Wolosker N.Puech-Leão P.De Luccia N.The need for a Vena Cava filter in oncological patients with acute venous thrombosis: a marker of a worse prognosis Ann Vasc Surg 60201935443080257210.1016/j.avsg.2018.12.085 · doi ↗ · pubmed ↗
- 7Zerati A.E.Wolosker N.Yazbek G.Langer M.Nishinari K.Vena cava filters in cancer patients: experience with 50 patients Clinics 60520053613661625467110.1590/s 1807-59322005000500003 · doi ↗ · pubmed ↗
- 8Kaufman J.Kinney T.Streiff M.Guidelines for the use of retrievable and convertible vena cava filters: report from the Society of Interventional Radiology Multidisciplinary Consensus Conference Surg Obes Relat Dis 2220062002121692534610.1016/j.soard.2006.03.009 · doi ↗ · pubmed ↗