Vaginal endometriosis following uterine transplantation in a patient with Mayer–Rokitansky–Küster–Hauser syndrome: A unique case report
Jana Moravcova, Roman Chmel, Jana Maluskova, Eva Sticova

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
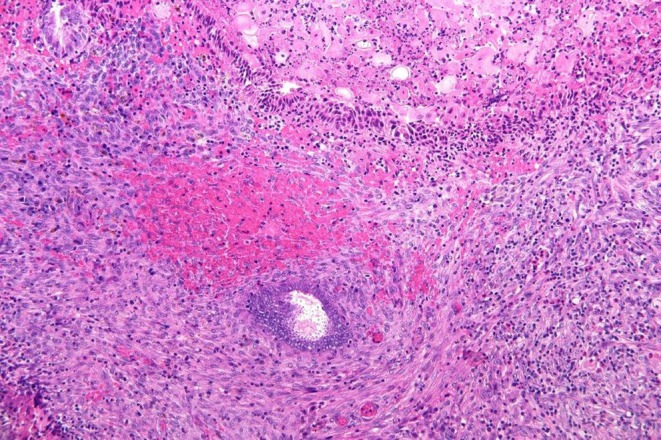 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGynecological conditions and treatments · Reproductive System and Pregnancy · Endometriosis Research and Treatment
Endometriosis is an estrogen‐dependent condition characterized by the presence of endometrial‐like tissue outside the uterus, most frequently involving the ovaries, uterosacral ligaments, and rectovaginal septum.1 Vaginal involvement usually occurs in the setting of deep infiltrating disease or following prior surgical intervention.2
Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome is a congenital malformation that manifests as uterovaginal agenesis.3 Uterine transplantation (UTx) has emerged as a reproductive option for women with absolute uterine factor infertility (AUFI), including those with MRKH syndrome.4
In the present study, we report a rare case of vaginal endometriosis in a woman with a neovagina after UTx. To our knowledge, this is the first documented case of endometriosis occurring in the setting of UTx.
A 23‐year‐old woman with MRKH syndrome was referred for UTx. Suspicion of uterovaginal agenesis was raised at the age of 15 due to primary amenorrhea. Magnetic resonance imaging confirmed the absence of a uterus, demonstrating small uterine remnants with no evidence of functional endometrium. In 2012, the patient underwent laparoscopic assisted neovagina creation using the modified Vecchietti technique.5 In 2017, she received a uterine graft from her 47‐year‐old mother,6 who showed no intraoperative or histologic evidence of endometriosis. The postoperative course was uneventful, with no rejection observed on surveillance biopsies. Immunosuppression was maintained with a triple‐drug regimen consisting of prednisolone, tacrolimus, and azathioprine.
Following transplantation, the patient reported regular menstruation of normal intensity, and endometrial biopsy was not deemed necessary until uterine graft explantation.
Two months after transplantation, the patient experienced progressive narrowing of the uterine–vaginal anastomosis. The resulting vaginal stricture was managed with surgical incision and temporary placement of a self‐expanding metallic stent. Nine months after transplantation, asymptomatic reactive tissue growth was incidentally observed during gynecologic examination beneath the distal edge of the inserted stent. Given its friable and highly vascular appearance, vaginal biopsy was performed.
Histologic examination revealed granulation tissue containing glandular structures surrounded by endometrial‐type spindle cell stroma, along with scattered hemosiderin‐laden macrophages (Figure 1). Both the glandular and stromal components demonstrated nuclear immunoreactivity for estrogen and progesterone receptor, and the stromal cells showed strong CD10 expression. These findings confirmed the diagnosis of endometriosis involving the neovaginal mucosa.
Several unsuccessful embryo transfer attempts were subsequently performed through a canal less than 10 mm in diameter at the site of the vaginal stricture. Although the graft initially remained stable, histologic evidence of severe rejection emerged several months later and proved refractory to intensified immunosuppressive therapy. It was ultimately explanted, and histologic assessment revealed no evidence of endometriosis or neoplastic transformation.
Endometriosis involving the neovagina of a woman with MRKH syndrome is highly unusual, given the history of uterine and vaginal agenesis. A plausible explanation for the presence of ectopic endometrial tissue is iatrogenic seeding and implantation of endometrial cells from the donor uterus into the neovaginal mucosa, which had been injured by the insertion of a metallic stent. Repeated stent placement and manipulation within the neovagina may have contributed to the worsening of the stricture, as well as to the survival of ectopic cells in the altered mucosal environment. Similar iatrogenic mechanisms have been proposed in cases of endometriosis arising within abdominal wall scars following cesarean delivery or other gynecologic procedures.7
No endometriosis was identified in the explanted graft, reinforcing the link to local trauma from the stent rather than incidental spread. This interpretation is further supported by the facts that the uterine premenopausal donor had no history or intraoperative findings suggestive of abdominal endometriosis and the recipient had no evidence of functional endometrium in the uterine remnants.
Although not directly implicated, long‐term immunosuppression may have contributed to a permissive tissue environment, given the recognized role of immune dysregulation in endometriosis pathogenesis.1 However, we consider local mucosal vulnerability around the implanted metal stent a more plausible factor in the development of neovaginal endometriosis.
Although the presence of endometriotic lesions complicated atraumatic embryo transfer, the associated vaginal stricture, likely exacerbated by repeated stent placement, appears to have represented the main obstacle to achieving pregnancy.
Other contributing factors to anastomotic stricture may include a short, narrow neovagina and the use of an excessive number of absorbable sutures. These observations underscore the need for an individualized surgical approach, especially in patients with MRKH syndrome, to minimize anastomotic complications and optimize reproductive outcomes.8
Preventing stricture formation at the anastomotic site after transplantation is essential, as it may impede the passage of the embryo transfer catheter through the cervical canal and ultimately jeopardize the primary goal of UTx–the delivery of a healthy infant.
The UTx was performed under a research protocol approved by The Ethics Committee of the Institute for Clinical and Experimental Medicine and Thomayer Hospital (protocol no. 2044/15, NM‐15‐01). Written informed consent was obtained from the patient for participation in the study and for publication of the accompanying clinical data.
AUTHOR CONTRIBUTIONS
Moravcova Jana, Maluskova Jana and Sticova Eva: Performed histopathologic analysis. Chmel Roman: Participated in collecting the laboratory and clinical data. Moravcova Jana, Sticova Eva and Chmel Roman: Were responsible for writing the manuscript. All authors revised and edited the draft and are in agreement with the content of the manuscript.
FUNDING INFORMATION
No financial support was used.
CONFLICT OF INTEREST STATEMENT
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Taylor HS , Kotlyar AM , Flores VA . Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021;397(10276):839‐852.33640070 10.1016/S 0140-6736(21)00389-5 · doi ↗ · pubmed ↗
- 2Nelson P . Endometriosis presenting as a vaginal mass. BMJ Case Rep. 2018;2018:bcr 2017222431.10.1136/bcr-2017-222431 PMC 578690229367370 · doi ↗ · pubmed ↗
- 3Herlin MK , Petersen MB , Brännström M . Mayer‐Rokitansky‐Küster‐Hauser (MRKH) syndrome: a comprehensive update. Orphanet J Rare Dis. 2020;15(1):214.32819397 10.1186/s 13023-020-01491-9PMC 7439721 · doi ↗ · pubmed ↗
- 4Cospain A , Dion L , Bidet M , et al. Optimizing care for MRKH patients: from malformation screening to uterus transplantation eligibility. Acta Obstet Gynecol Scand. 2025;104(3):514‐521.39382201 10.1111/aogs.14985 PMC 11871100 · doi ↗ · pubmed ↗
- 5Fedele L , Bianchi S , Frontino G , Fontana E , Restelli E , Bruni V . The laparoscopic Vecchietti's modified technique in Rokitansky syndrome: anatomic, functional and sexual long‐term results. Am J Obstet Gynecol. 2008;198(4):377.e 1–6.10.1016/j.ajog.2007.10.80718241821 · doi ↗ · pubmed ↗
- 6Chmel R , Novackova M , Janousek L , et al. Revaluation and lessons learned from a first 9 cases of a Czech uterus transplantation trial: four deceased donor and 5 living donor uterus transplantations. Am J Transplant. 2019;19(3):855‐864.30151893 10.1111/ajt.15096 · doi ↗ · pubmed ↗
- 7Gunes M , Kayikcioglu F , Ozturkoglu E , Haberal A . Incisional endometriosis after caesarean section, episiotomy and other gynaecologic procedures. J Obstet Gynaecol Res. 2005;31(5):471‐475.16176520 10.1111/j.1447-0756.2005.00322.x · doi ↗ · pubmed ↗
- 8Chmel R , Novackova M , Pastor Z . Lessons learned from the Czech uterus transplant trial related to surgical technique that may affect reproductive success. Aust N Z J Obstet Gynaecol. 2020;60(4):625‐627.32573763 10.1111/ajo.13184 · doi ↗ · pubmed ↗