Long‐term results of the Musset surgical technique in the treatment of recto‐vaginal fistulas
Joy Bloomfield, Bassam Haddad, Geoffroy Canlorbe, Cyril Touboul, Edouard Lecarpentier, Yohann Dabi

TL;DR
This study evaluates the long-term effectiveness of the Musset surgical technique for treating recto-vaginal fistulas, finding moderate success but high complication rates.
Contribution
The study provides the first detailed long-term evaluation of the Musset surgical technique for recto-vaginal fistulas.
Findings
The Musset technique had a 48.4% success rate in curing recto-vaginal fistulas.
High complication (54.8%) and reintervention (35.7%) rates were observed.
Patients reported improved quality of life and satisfaction post-surgery.
Abstract
Recto‐vaginal fistulas (RVF) are a rare pathology, mostly affecting developing countries. They are mainly obstetrical (88% of cases) and have an incidence of 0.5%. Musset's surgical technique in the management of RVF has been the subject of few studies and there is little data in the literature concerning the evaluation of its long‐term efficiency and its morbidity. The aim of our study was to investigate the long‐term results of patients who underwent Musset's surgery for cure of RVF. We conducted a monocentric cohort study between January 1, 2002, and December 31, 2020 including patients who had undergone a RVF cure by the Musset technique. These patients were recalled in consultation to be examined and completed a questionnaire designed for this study with validated functional and quality‐of‐life scores. For patients who did not respond to this solicitation, information was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
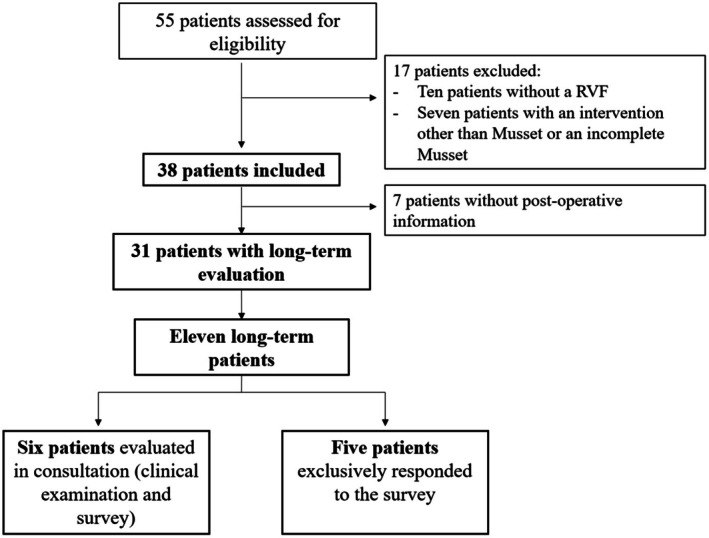 FIGURE 1
FIGURE 1| Characteristics | Number ( | Percentage (%) IQR |
|---|---|---|
| Age | 35.5 | 30.3–39.8 |
| Geographic origin | ||
| Europe | 11/22 | 50 |
| North Africa | 2/22 | 9 |
| Sub‐Saharan Africa | 8/22 | 36.4 |
| Asia | 1/22 | 4.6 |
| Parity | 2 | 1–4 |
| Delivery mode | ||
| Absence of delivery | 3/38 | 7.9 |
| Spontaneous vaginal delivery | 37/61 | 60.7 |
| Instrumental delivery | 13/61 | 21.3 |
| Emergency cesarean section | 7/61 | 11.5 |
| Planned cesarean section | 1/61 | 1.6 |
| Perineum | ||
| Intact | 9/49 | 18.4 |
| First and second‐degree tear | 2/49 | 4.1 |
| Third‐degree tear | 4/49 | 8.2 |
| Fourth‐degree tear | 23/49 | 46.9 |
| Episiotomy | 11/49 | 22.4 |
| Etiology of RVF | ||
| Obstetrical | 31/38 | 81.6 |
| Postoperative | 3/38 | 7.9 |
| Local infection | 2/38 | 5.3 |
| Crohn's disease | 1/38 | 2.6 |
| Local trauma | 1/38 | 2.6 |
| Previous recto‐vaginal repair | 12/38 | 31.6 |
| Number of previous interventions | 0 | 0–1 |
| Type of previous interventions | ||
| Musset technique | 6/21 | 28.6 |
| Fistulotomy | 5/21 | 23.8 |
| Martius flap | 4/21 | 19 |
| Collagen plug | 3/21 | 14.3 |
| Colostomy | 2/21 | 9.5 |
| Seton‐assisted fistula repair | 1/21 | 4.8 |
| Symptoms | ||
| Stool and gas incontinence | 28/38 | 73.6 |
| Gas incontinence | 5/38 | 13.2 |
| Local infection | 5/38 | 13.2 |
| Delay between beginning of incontinence symptoms and consultation (months) | 38 | 12–180 |
| Characteristics | Number ( | Percentage (%) |
|---|---|---|
| RVF visualized during consultation | 29/32 | 90.6 |
| Diameter | ||
| ≤2 cm | 14/28 | 50 |
| >2 cm | 14/28 | 50 |
| Localization | ||
| <2/3 lower portion of the vaginal wall | 14/29 | 48.3 |
| ≥1/3 upper portion of the vaginal wall | 15/29 | 51.7 |
| Rectal endoscopic ultrasound | 17/38 | 44.7 |
| Visualization of sphincter lesions | 16/17 | 94.1 |
| Other examinations | 7/38 | 18.4 |
| Pelvic MRI | 3/38 | 7.9 |
| Anorectal manometries | 3/38 | 7.9 |
| Anal sphincter electromyographies | 2/38 | 5.3 |
| Characteristics | Number ( | Percentage (%) IQR |
|---|---|---|
| Number of Musset technique stages | ||
| 1 stage | 24/38 | 63.2 |
| 2 stages | 14/38 | 36.8 |
| Duration of hospitalization (days) | 4 | 2.3–5 |
| Postoperative complications (Clavien‐Dindo classification) | ||
| None | 14/31 | 45.2 |
| Grade I | 4/31 | 12.9 |
| Grade II | 6/31 | 19.3 |
| Grade IIIa | 1/31 | 3.2 |
| Grade IIIb | 7/31 | 19.4 |
| Grade IV and V | 0/31 | 0 |
| Reintervention | 5/14 | 35.7 |
| Delay (days) | 9 | 3.5–22.5 |
| Type of reintervention | ||
| Musset technique | 3/5 | 60 |
| Fistulotomy | 2/5 | 40 |
| Characteristics | Number ( | Percentage (%) IQR |
|---|---|---|
| Recurrence of symptoms | 16/31 | 51.6 |
| Gas incontinence | 7/16 | 43.8 |
| Stool incontinence | 3/16 | 18.7 |
| Gas and stool incontinence | 6/16 | 37.5 |
| Dyspareunia | 1/11 | 9.1 |
| Aesthetic result | 21/27 | 77.8 |
| Subsequent pregnancy | 5/14 | 35.7 |
| Delay surgery—pregnancy (months) | 48 | 28–48 |
| Follow‐up (months) | 7 | 1.5–48 |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | Patient 9 | Patient 10 | Patient 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Delay follow‐up (years) | 4 | 4 | 11 | 15 | 16 | 19 | 5 | 4 | 17 | 2 | 3 |
| Incontinence (Cleveland score) | |||||||||||
| Solid stool incontinence | |||||||||||
| Preoperative | 0 | 0 | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 4 | — |
| Postoperative | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | — |
| Liquid stool incontinence | |||||||||||
| Preoperative | 1 | 3 | 3 | 1 | 1 | 1 | 1 | 3 | 4 | 4 | — |
| Postoperative | 0 | 2 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | — |
| Gas incontinence | |||||||||||
| Preoperative | 4 | 4 | 2 | 1 | 1 | 1 | 1 | 4 | 4 | 4 | — |
| Postoperative | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 3 | 0 | 0 | — |
| Pads | |||||||||||
| Preoperative | 0 | 3 | 4 | 0 | 1 | 1 | 4 | 3 | 4 | 0 | — |
| Postoperative | 0 | 0 | 4 | 0 | 1 | 1 | 4 | 0 | 0 | 0 | — |
| Lifestyle alteration | |||||||||||
| Preoperative | 3 | 4 | 4 | 2 | 2 | 3 | 1 | 0 | 0 | 4 | — |
| Postoperative | 1 | 0 | 0 | 3 | 0 | 0 | 4 | 4 | 4 | 0 | — |
| Global satisfaction | |||||||||||
| PGI‐I | 1 | 1 | 1 | 3 | 2 | 1 | 1 | 2 | 1 | 1 | 1 |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | |
|---|---|---|---|---|---|---|
| Genital hiatus (cm) | 5 | 3.5 | 3 | 3.5 | 3 | 4 |
| Perineal body (cm) | 2.5 | 1 | 2 | 1.5 | 4 | 3 |
| Presence of a perineal gap | Yes | Yes | No | Yes | No | No |
| Levator ani avulsion | No | Yes | No | No | No | No |
| Levator ani contraction (/5) | 2 | 2 | 3 | 1 | 4 | 4 |
| Rectal sensibility | Yes | Yes | Yes | Yes | Yes | Yes |
| Rectal contraction (/5) | 2 | 1 | 4 | 3 | 5 | 4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnorectal Disease Treatments and Outcomes · Pelvic floor disorders treatments · Diverticular Disease and Complications
INTRODUCTION
1
Recto‐vaginal fistulas (RVF) are a rare pathology and mainly concern developing countries where they have an incidence of 1.57 per 1000 women in age to procreate.1 It is estimated that 88% of RVF are obstetrical2 due to the poor access to health care facilities, which is responsible for prolonged labor and dystocia. In a study by Goldaber et al.,3 on 24 000 vaginal births, there was an incidence of RVF of 0.5%. The prevalence of obstetric fistulas is difficult to estimate,4 but is thought to affect over 2 million women worldwide,5 with 50 000 to 100 000 new cases per year in Africa alone.6 In Africa, it is estimated that two to three patients suffer from fistulas per 1000 deliveries, with a prevalence of 0.3% in countries where maternal mortality is higher than 500 per 100 000 live births.7 The second most common cause of RVF is Crohn's disease, where RVF can occur in up to 10% of patients.8 The symptomatology of RVF is variable: they can be paucisymptomatic and therefore be responsible for diagnostic errancy, or they can cause severe symptoms, such as an emission of gas and/or feces through the vagina, responsible for an important alteration in the quality of life of these patients.
Clinical examination is essential in this pathology as it establishes the diagnosis of RVF and allows the RVF to be classified as simple or complex according to the classification of Rothenberger9 which orientates the surgical management.
Currently, there is little data concerning the efficiency and outcomes after RVF repair surgery based on the different methods available. Studies analyzing these surgical techniques are often retrospective with a small number of patients included. For example, the studies by Pitel et al.10 concerning the Martius flap and by Hull et al.11 concerning the gracilis flap in RVF repairs were both retrospective and include only 20 and 22 patients, respectively. Additionally, studies concerning RVF repair surgeries have short‐term median follow‐ups and generally do not evaluate their postoperative long‐term results. In the studies cited above, the median follow‐up was 35 and 7 months, respectively, and none reported their long‐term results.
The Musset technique, initially described in 1971,12 is one of the many surgical methods used to treat RVF. This technique has proven to be efficient but has often been studied in combination with other surgical techniques. When studied alone, research concerning this technique has short follow‐up periods with a small number of patients included. In a study of Leroy et al.,13 only nine patients having had a RVF repair by the Musset technique were evaluated in order to verify that there was no recurrence of symptoms and the delay of evaluation was 6 to 8 weeks after the operation. In the retrospective study of Chew and Rieger,14 seven patients were recalled by a telephone interview with a median follow‐up period of 24 months but none underwent clinical examination in order to assess anatomical and functional outcomes. In a study published in 2001 by Soriano et al.,15 48 patients had a RVF repair by the Musset technique with a follow‐up period between 1 to 3 years postoperatively. Among these patients, five had a reintervention and stool continence was obtained in 98% of patients. Quality of life, mental health, satisfaction rates and sexual function were not evaluated in these patients.
The aim of our study was to study the global outcomes of patients who had undergone repair of their RVF by Musset's technique.
MATERIALS AND METHODS
2
Study population
2.1
A monocentric cohort study was carried out including patients treated in our tertiary referral center of Intercommunal hospital of Creteil between January 1, 2002, and December 31, 2020. All patients that had undergone a RVF cure by the Musset technique were selected. Patients having had this procedure were identified according to the coding of their surgical procedure. Patients that had a repair of RVF using another technique than Musset and those that did not have a RVF were excluded. Data concerning the included patients were retrieved retrospectively from the medical records.
The committee for the protection of persons gave its approval for this study to be carried out on October 7, 2021 (file no.: 21.00386.000023).
Description of the Musset technique
2.2
The first stage is a horizontal incision of the perineum with the removal of the fistula by scalpel and marker threads are placed on the vaginal and rectal mucosal limits. A transverse incision thanks to the exposure of the four marker threads is then made in order to allow the dissection of the rectovaginal plane. The anal canal and sphincter, the vagina and the perineum are then successively closed with absorbable sutures. The technique is visually represented in Figure 1.16 This surgical technique can be performed in one or two steps. If performed in two steps, there is a healing period of several months between the first stage and the rest of the operation. Postoperatively, there is daily local care with a hospitalization which lasts 3–4 days and constipation is prevented by laxatives.
Flow chart.
Outcome assessment
2.3
Patients were recalled for this study using email and telephone calls and had to be evaluated at least 6 months postoperatively. Those answering these solicitations were given a specific survey established for this study and were invited to a consultation for a physical examination. Patients who did not wish to do the consultation were asked to complete the survey only. This survey included questions concerning symptoms, postoperative fertility outcomes, and had validated scores for symptoms of fecal incontinence (Cleveland score), overall satisfaction of the patients (patient global impression of improvement PGI‐I score), quality of life (SF‐36 questionnaire), mental health (WHOQOL‐Bref questionnaire) and sexual life (FSFI questionnaire) (Appendix S1).17, 18, 19, 20 The measures realized during the clinical examination were based on the POP‐Q system.21
Data concerning the included patients were retrieved in two manners: prospectively for the patients having had a long‐term evaluation (n = 11) and retrospectively from the postoperative consultations in the medical records for the patients who did not respond to the solicitations (n = 27). The surgical technique was considered successful if the patient was continent for gas and stool at the time of evaluation. Additional analysis on quality of life, mental health, sexual life and anatomical results was done on the recalled patients.
Statistical analysis
2.4
Due the small number of patients included the analysis was only descriptive. For quantitative variables, medians and interquartile ranges were calculated. For qualitative variables, number and percentages are reported.
RESULTS
3
A total of 38 patients benefited from RVF repair using the Musset technique. Postoperative results were retrieved for 31 patients. Among the included patients, 11 responded to the long‐term follow‐up (n = 11/38, 28.9%). Among the 11 recalled patients, six came to the consultation and underwent physical examination.
Results of patients having had a RVF repair by Musset's surgical technique (n = 38)
3.1
The median age of the patients was 35.5 years (30.3–39.8 years). The majority of the RVFs treated were obstetrical (n = 31/38, 81.6%). The perineal status of the 31 patients with obstetrical RVF was: 21 fourth‐degree tears, four third‐degree tears, one tear that was labeled second‐degree, four episiotomies, and one unknown perineal status. A total of 12 patients (n = 12/38, 31.6%) had at least one previous procedure for their RVF. Concerning the symptoms that motivated the consultation, 73.6% of the patients had a gas and stool incontinence (n = 28/38) (Table 1).
TABLE 1: Characteristics of the patients having had a recto‐vaginal fistula repair by Musset's surgical technique (n = 38).
<table><col align="left"/><col align="left"/><col align="left"/><thead><tr><th align="left" rowspan="1" colspan="1">Characteristics</th><th align="left" rowspan="1" colspan="1">Number (<italic>n</italic>)</th><th align="left" rowspan="1" colspan="1">Percentage (%) IQR</th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">Age</td><td align="left" rowspan="1" colspan="1">35.5</td><td align="left" rowspan="1" colspan="1">30.3–39.8</td></tr><tr><td align="left" colspan="3" rowspan="1">Geographic origin</td></tr><tr><td align="left" rowspan="1" colspan="1">Europe</td><td align="left" rowspan="1" colspan="1">11/22</td><td align="left" rowspan="1" colspan="1">50</td></tr><tr><td align="left" rowspan="1" colspan="1">North Africa</td><td align="left" rowspan="1" colspan="1">2/22</td><td align="left" rowspan="1" colspan="1">9</td></tr><tr><td align="left" rowspan="1" colspan="1">Sub‐Saharan Africa</td><td align="left" rowspan="1" colspan="1">8/22</td><td align="left" rowspan="1" colspan="1">36.4</td></tr><tr><td align="left" rowspan="1" colspan="1">Asia</td><td align="left" rowspan="1" colspan="1">1/22</td><td align="left" rowspan="1" colspan="1">4.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Parity</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1–4</td></tr><tr><td align="left" colspan="3" rowspan="1">Delivery mode<xref> <sup>a</sup> </xref> </td></tr><tr><td align="left" rowspan="1" colspan="1">Absence of delivery</td><td align="left" rowspan="1" colspan="1">3/38</td><td align="left" rowspan="1" colspan="1">7.9</td></tr><tr><td align="left" rowspan="1" colspan="1">Spontaneous vaginal delivery</td><td align="left" rowspan="1" colspan="1">37/61</td><td align="left" rowspan="1" colspan="1">60.7</td></tr><tr><td align="left" rowspan="1" colspan="1">Instrumental delivery</td><td align="left" rowspan="1" colspan="1">13/61</td><td align="left" rowspan="1" colspan="1">21.3</td></tr><tr><td align="left" rowspan="1" colspan="1">Emergency cesarean section</td><td align="left" rowspan="1" colspan="1">7/61</td><td align="left" rowspan="1" colspan="1">11.5</td></tr><tr><td align="left" rowspan="1" colspan="1">Planned cesarean section</td><td align="left" rowspan="1" colspan="1">1/61</td><td align="left" rowspan="1" colspan="1">1.6</td></tr><tr><td align="left" colspan="3" rowspan="1">Perineum</td></tr><tr><td align="left" rowspan="1" colspan="1">Intact</td><td align="left" rowspan="1" colspan="1">9/49</td><td align="left" rowspan="1" colspan="1">18.4</td></tr><tr><td align="left" rowspan="1" colspan="1">First and second‐degree tear</td><td align="left" rowspan="1" colspan="1">2/49</td><td align="left" rowspan="1" colspan="1">4.1</td></tr><tr><td align="left" rowspan="1" colspan="1">Third‐degree tear</td><td align="left" rowspan="1" colspan="1">4/49</td><td align="left" rowspan="1" colspan="1">8.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Fourth‐degree tear</td><td align="left" rowspan="1" colspan="1">23/49</td><td align="left" rowspan="1" colspan="1">46.9</td></tr><tr><td align="left" rowspan="1" colspan="1">Episiotomy</td><td align="left" rowspan="1" colspan="1">11/49</td><td align="left" rowspan="1" colspan="1">22.4</td></tr><tr><td align="left" colspan="3" rowspan="1">Etiology of RVF</td></tr><tr><td align="left" rowspan="1" colspan="1">Obstetrical</td><td align="left" rowspan="1" colspan="1">31/38</td><td align="left" rowspan="1" colspan="1">81.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Postoperative</td><td align="left" rowspan="1" colspan="1">3/38<xref> <sup>b</sup> </xref> </td><td align="left" rowspan="1" colspan="1">7.9</td></tr><tr><td align="left" rowspan="1" colspan="1">Local infection</td><td align="left" rowspan="1" colspan="1">2/38</td><td align="left" rowspan="1" colspan="1">5.3</td></tr><tr><td align="left" rowspan="1" colspan="1">Crohn's disease</td><td align="left" rowspan="1" colspan="1">1/38</td><td align="left" rowspan="1" colspan="1">2.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Local trauma</td><td align="left" rowspan="1" colspan="1">1/38</td><td align="left" rowspan="1" colspan="1">2.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Previous recto‐vaginal repair</td><td align="left" rowspan="1" colspan="1">12/38</td><td align="left" rowspan="1" colspan="1">31.6<xref> <sup>c</sup> </xref> </td></tr><tr><td align="left" rowspan="1" colspan="1">Number of previous interventions</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0–1</td></tr><tr><td align="left" colspan="3" rowspan="1">Type of previous interventions</td></tr><tr><td align="left" rowspan="1" colspan="1">Musset technique</td><td align="left" rowspan="1" colspan="1">6/21</td><td align="left" rowspan="1" colspan="1">28.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Fistulotomy</td><td align="left" rowspan="1" colspan="1">5/21</td><td align="left" rowspan="1" colspan="1">23.8</td></tr><tr><td align="left" rowspan="1" colspan="1">Martius flap</td><td align="left" rowspan="1" colspan="1">4/21</td><td align="left" rowspan="1" colspan="1">19</td></tr><tr><td align="left" rowspan="1" colspan="1">Collagen plug</td><td align="left" rowspan="1" colspan="1">3/21</td><td align="left" rowspan="1" colspan="1">14.3</td></tr><tr><td align="left" rowspan="1" colspan="1">Colostomy</td><td align="left" rowspan="1" colspan="1">2/21</td><td align="left" rowspan="1" colspan="1">9.5</td></tr><tr><td align="left" rowspan="1" colspan="1">Seton‐assisted fistula repair</td><td align="left" rowspan="1" colspan="1">1/21</td><td align="left" rowspan="1" colspan="1">4.8</td></tr><tr><td align="left" colspan="3" rowspan="1">Symptoms</td></tr><tr><td align="left" rowspan="1" colspan="1">Stool and gas incontinence</td><td align="left" rowspan="1" colspan="1">28/38</td><td align="left" rowspan="1" colspan="1">73.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Gas incontinence</td><td align="left" rowspan="1" colspan="1">5/38</td><td align="left" rowspan="1" colspan="1">13.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Local infection</td><td align="left" rowspan="1" colspan="1">5/38</td><td align="left" rowspan="1" colspan="1">13.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Delay between beginning of incontinence symptoms and consultation (months)</td><td align="left" rowspan="1" colspan="1">38</td><td align="left" rowspan="1" colspan="1">12–180</td></tr></tbody></table>The RVF was not visualized during clinical examination in 9.4% of cases (n = 3/32) and among the RVF visualized, 50% had a diameter >2 cm (n = 14/28) (Table 2).
TABLE 2: Characteristics of the recto‐vaginal fistulas of the patients having had a recto‐vaginal fistula repair by Musset's surgical technique (n = 38).
<table><col align="left"/><col align="left"/><col align="left"/><thead><tr><th align="left" rowspan="1" colspan="1">Characteristics</th><th align="left" rowspan="1" colspan="1">Number (<italic>n</italic>)</th><th align="left" rowspan="1" colspan="1">Percentage (%)</th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">RVF visualized during consultation</td><td align="left" rowspan="1" colspan="1">29/32</td><td align="left" rowspan="1" colspan="1">90.6</td></tr><tr><td align="left" colspan="3" rowspan="1">Diameter</td></tr><tr><td align="left" rowspan="1" colspan="1">≤2 cm</td><td align="left" rowspan="1" colspan="1">14/28</td><td align="left" rowspan="1" colspan="1">50</td></tr><tr><td align="left" rowspan="1" colspan="1">>2 cm</td><td align="left" rowspan="1" colspan="1">14/28</td><td align="left" rowspan="1" colspan="1">50</td></tr><tr><td align="left" colspan="3" rowspan="1">Localization</td></tr><tr><td align="left" rowspan="1" colspan="1"><2/3 lower portion of the vaginal wall</td><td align="left" rowspan="1" colspan="1">14/29</td><td align="left" rowspan="1" colspan="1">48.3</td></tr><tr><td align="left" rowspan="1" colspan="1">≥1/3 upper portion of the vaginal wall</td><td align="left" rowspan="1" colspan="1">15/29</td><td align="left" rowspan="1" colspan="1">51.7</td></tr><tr><td align="left" rowspan="1" colspan="1">Rectal endoscopic ultrasound</td><td align="left" rowspan="1" colspan="1">17/38</td><td align="left" rowspan="1" colspan="1">44.7</td></tr><tr><td align="left" rowspan="1" colspan="1">Visualization of sphincter lesions</td><td align="left" rowspan="1" colspan="1">16/17</td><td align="left" rowspan="1" colspan="1">94.1</td></tr><tr><td align="left" rowspan="1" colspan="1">Other examinations</td><td align="left" rowspan="1" colspan="1">7/38</td><td align="left" rowspan="1" colspan="1">18.4</td></tr><tr><td align="left" rowspan="1" colspan="1">Pelvic MRI</td><td align="left" rowspan="1" colspan="1">3/38</td><td align="left" rowspan="1" colspan="1">7.9</td></tr><tr><td align="left" rowspan="1" colspan="1">Anorectal manometries</td><td align="left" rowspan="1" colspan="1">3/38</td><td align="left" rowspan="1" colspan="1">7.9</td></tr><tr><td align="left" rowspan="1" colspan="1">Anal sphincter electromyographies</td><td align="left" rowspan="1" colspan="1">2/38</td><td align="left" rowspan="1" colspan="1">5.3</td></tr></tbody></table>The majority of the RVF repairs were done during a single procedure (n = 24/38, 63.2%). Half of the patients (n = 14/31, 45.2%) had no postoperative complications. There was a reintervention in 35.7% of cases (n = 5/14): three were Musset techniques and two were fistulotomies (Table 3).
TABLE 3: Characteristics of surgical management of the patients having had a recto‐vaginal fistula repair by Musset's surgical technique (n = 38).
<table><col align="left"/><col align="left"/><col align="left"/><thead><tr><th align="left" rowspan="1" colspan="1">Characteristics</th><th align="left" rowspan="1" colspan="1">Number (<italic>n</italic>)</th><th align="left" rowspan="1" colspan="1">Percentage (%) IQR</th></tr></thead><tbody><tr><td align="left" colspan="3" rowspan="1">Number of Musset technique stages</td></tr><tr><td align="left" rowspan="1" colspan="1">1 stage</td><td align="left" rowspan="1" colspan="1">24/38</td><td align="left" rowspan="1" colspan="1">63.2</td></tr><tr><td align="left" rowspan="1" colspan="1">2 stages</td><td align="left" rowspan="1" colspan="1">14/38</td><td align="left" rowspan="1" colspan="1">36.8</td></tr><tr><td align="left" rowspan="1" colspan="1">Duration of hospitalization (days)</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">2.3–5</td></tr><tr><td align="left" colspan="3" rowspan="1">Postoperative complications (Clavien‐Dindo classification)</td></tr><tr><td align="left" rowspan="1" colspan="1">None</td><td align="left" rowspan="1" colspan="1">14/31</td><td align="left" rowspan="1" colspan="1">45.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Grade I</td><td align="left" rowspan="1" colspan="1">4/31<xref> <sup>a</sup> </xref> </td><td align="left" rowspan="1" colspan="1">12.9</td></tr><tr><td align="left" rowspan="1" colspan="1">Grade II</td><td align="left" rowspan="1" colspan="1">6/31<xref> <sup>b</sup> </xref> </td><td align="left" rowspan="1" colspan="1">19.3</td></tr><tr><td align="left" rowspan="1" colspan="1">Grade IIIa</td><td align="left" rowspan="1" colspan="1">1/31<xref> <sup>c</sup> </xref> </td><td align="left" rowspan="1" colspan="1">3.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Grade IIIb</td><td align="left" rowspan="1" colspan="1">7/31<xref> <sup>d</sup> </xref> </td><td align="left" rowspan="1" colspan="1">19.4</td></tr><tr><td align="left" rowspan="1" colspan="1">Grade IV and V</td><td align="left" rowspan="1" colspan="1">0/31</td><td align="left" rowspan="1" colspan="1">0</td></tr><tr><td align="left" rowspan="1" colspan="1">Reintervention</td><td align="left" rowspan="1" colspan="1">5/14</td><td align="left" rowspan="1" colspan="1">35.7</td></tr><tr><td align="left" rowspan="1" colspan="1">Delay (days)</td><td align="left" rowspan="1" colspan="1">9</td><td align="left" rowspan="1" colspan="1">3.5–22.5</td></tr><tr><td align="left" colspan="3" rowspan="1">Type of reintervention</td></tr><tr><td align="left" rowspan="1" colspan="1">Musset technique</td><td align="left" rowspan="1" colspan="1">3/5</td><td align="left" rowspan="1" colspan="1">60</td></tr><tr><td align="left" rowspan="1" colspan="1">Fistulotomy</td><td align="left" rowspan="1" colspan="1">2/5</td><td align="left" rowspan="1" colspan="1">40</td></tr></tbody></table>Half of the patients had a recurrence of their symptoms (n = 16/31, 51.6%), with mainly exclusive gas incontinence (n = 7/16, 43.8%). Five patients had pregnancies postoperatively (n = 5/14, 35.7%) and all deliveries were scheduled cesarean sections (Table 4).
TABLE 4: Postoperative characteristics of the patients having had a recto‐vaginal fistula repair by Musset's surgical technique (n = 38).
<table><col align="left"/><col align="left"/><col align="left"/><thead><tr><th align="left" rowspan="1" colspan="1">Characteristics</th><th align="left" rowspan="1" colspan="1">Number (<italic>n</italic>)</th><th align="left" rowspan="1" colspan="1">Percentage (%) IQR</th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">Recurrence of symptoms</td><td align="left" rowspan="1" colspan="1">16/31</td><td align="left" rowspan="1" colspan="1">51.6</td></tr><tr><td align="left" rowspan="1" colspan="1">Gas incontinence</td><td align="left" rowspan="1" colspan="1">7/16</td><td align="left" rowspan="1" colspan="1">43.8</td></tr><tr><td align="left" rowspan="1" colspan="1">Stool incontinence</td><td align="left" rowspan="1" colspan="1">3/16</td><td align="left" rowspan="1" colspan="1">18.7</td></tr><tr><td align="left" rowspan="1" colspan="1">Gas and stool incontinence</td><td align="left" rowspan="1" colspan="1">6/16</td><td align="left" rowspan="1" colspan="1">37.5</td></tr><tr><td align="left" rowspan="1" colspan="1">Dyspareunia</td><td align="left" rowspan="1" colspan="1">1/11</td><td align="left" rowspan="1" colspan="1">9.1</td></tr><tr><td align="left" rowspan="1" colspan="1">Aesthetic result</td><td align="left" rowspan="1" colspan="1">21/27</td><td align="left" rowspan="1" colspan="1">77.8</td></tr><tr><td align="left" rowspan="1" colspan="1">Subsequent pregnancy<xref> <sup>a</sup> </xref> </td><td align="left" rowspan="1" colspan="1">5/14</td><td align="left" rowspan="1" colspan="1">35.7</td></tr><tr><td align="left" rowspan="1" colspan="1">Delay surgery—pregnancy (months)</td><td align="left" rowspan="1" colspan="1">48</td><td align="left" rowspan="1" colspan="1">28–48</td></tr><tr><td align="left" rowspan="1" colspan="1">Follow‐up (months)</td><td align="left" rowspan="1" colspan="1">7</td><td align="left" rowspan="1" colspan="1">1.5–48</td></tr></tbody></table>Long‐term evaluation of the recalled patients (n = 11)
3.2
Overall satisfaction
Most patients described having a better life postoperatively since the procedure (n = 10/11, 90.9%) and all patients were happy with their surgery (n = 11/11, 100%) (Table 5). All the patients described diagnostic errancy with the consultation of two to three specialists before the diagnosis of RVF was made.
TABLE 5: Results of the surveys in the recalled patients (n = 11).
<table><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><thead><tr><th align="left" rowspan="1" colspan="1"/><th align="left" rowspan="1" colspan="1">Patient 1</th><th align="left" rowspan="1" colspan="1">Patient 2</th><th align="left" rowspan="1" colspan="1">Patient 3</th><th align="left" rowspan="1" colspan="1">Patient 4</th><th align="left" rowspan="1" colspan="1">Patient 5</th><th align="left" rowspan="1" colspan="1">Patient 6</th><th align="left" rowspan="1" colspan="1">Patient 7</th><th align="left" rowspan="1" colspan="1">Patient 8</th><th align="left" rowspan="1" colspan="1">Patient 9</th><th align="left" rowspan="1" colspan="1">Patient 10</th><th align="left" rowspan="1" colspan="1">Patient 11</th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">Delay follow‐up (years)</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">11</td><td align="left" rowspan="1" colspan="1">15</td><td align="left" rowspan="1" colspan="1">16</td><td align="left" rowspan="1" colspan="1">19</td><td align="left" rowspan="1" colspan="1">5</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">17</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">3</td></tr><tr><td align="left" colspan="12" rowspan="1">Incontinence (Cleveland score)</td></tr><tr><td align="left" colspan="12" rowspan="1">Solid stool incontinence</td></tr><tr><td align="left" rowspan="1" colspan="1">Preoperative</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" rowspan="1" colspan="1">Postoperative</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" colspan="12" rowspan="1">Liquid stool incontinence</td></tr><tr><td align="left" rowspan="1" colspan="1">Preoperative</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" rowspan="1" colspan="1">Postoperative</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" colspan="12" rowspan="1">Gas incontinence</td></tr><tr><td align="left" rowspan="1" colspan="1">Preoperative</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" rowspan="1" colspan="1">Postoperative</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" colspan="12" rowspan="1">Pads</td></tr><tr><td align="left" rowspan="1" colspan="1">Preoperative</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" rowspan="1" colspan="1">Postoperative</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" colspan="12" rowspan="1">Lifestyle alteration</td></tr><tr><td align="left" rowspan="1" colspan="1">Preoperative</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" rowspan="1" colspan="1">Postoperative</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">0</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td align="left" colspan="12" rowspan="1">Global satisfaction</td></tr><tr><td align="left" rowspan="1" colspan="1">PGI‐I</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">1</td></tr></tbody></table>Incontinence (Cleveland score)
Three out of 11 patients (27.3%) had concomitant gas and stool continence. None of the patients had a solid stool incontinence postoperatively, whereas four patients had solid stool incontinence preoperatively (Table 5).
Quality of life
In the Cleveland score, quality of life was improved postoperatively and in the SF‐36 score, there were no limitations due to physical health nor due to emotional problems with a median score of 100 (87.50–100) and 100 (66.65–100), respectively.
Mental health (WHOQOL‐Bref score)
The median scores were elevated with a median score of 81 (62.50–84.50) regarding physical health, 75 (61–81) regarding psychological health, 75 (62.50–78) regarding social relationships and 75 (66–81) regarding the environment.
Sexual function (FSFI score)
All patients who completed the survey had a stable sexual partner. The median scores were 4.2 (3–4.20) regarding desire, 4.2 (3.15–4.95) regarding arousal, 4.8 (4.20–5.25) regarding lubrication, 4.8 (3–5) regarding orgasm, 5.2 (3.40–6) regarding satisfaction and 4.4 (2.60–5.60) regarding pain. The median total score of all the patients was 23.50/36.
Physical examination
Six patients were seen in consultation (n = 6/11, 54.5%). They had a normal cicatrization of their perineal scars and no fistula was visualized during examination. During the Valsalva maneuvers, there was no emission of gas or stool (Table 6).
TABLE 6: Characteristics of the clinical examination during the long‐term evaluation.
<table><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><col align="left"/><thead><tr><th align="left" rowspan="1" colspan="1"/><th align="left" rowspan="1" colspan="1">Patient 1</th><th align="left" rowspan="1" colspan="1">Patient 2</th><th align="left" rowspan="1" colspan="1">Patient 3</th><th align="left" rowspan="1" colspan="1">Patient 4</th><th align="left" rowspan="1" colspan="1">Patient 5</th><th align="left" rowspan="1" colspan="1">Patient 6</th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">Genital hiatus (cm)</td><td align="left" rowspan="1" colspan="1">5</td><td align="left" rowspan="1" colspan="1">3.5</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">3.5</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">4</td></tr><tr><td align="left" rowspan="1" colspan="1">Perineal body (cm)</td><td align="left" rowspan="1" colspan="1">2.5</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1.5</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">3</td></tr><tr><td align="left" rowspan="1" colspan="1">Presence of a perineal gap</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">No</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">No</td><td align="left" rowspan="1" colspan="1">No</td></tr><tr><td align="left" rowspan="1" colspan="1">Levator ani avulsion</td><td align="left" rowspan="1" colspan="1">No</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">No</td><td align="left" rowspan="1" colspan="1">No</td><td align="left" rowspan="1" colspan="1">No</td><td align="left" rowspan="1" colspan="1">No</td></tr><tr><td align="left" rowspan="1" colspan="1">Levator ani contraction (/5)</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">4</td></tr><tr><td align="left" rowspan="1" colspan="1">Rectal sensibility</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">Yes</td><td align="left" rowspan="1" colspan="1">Yes</td></tr><tr><td align="left" rowspan="1" colspan="1">Rectal contraction (/5)</td><td align="left" rowspan="1" colspan="1">2</td><td align="left" rowspan="1" colspan="1">1</td><td align="left" rowspan="1" colspan="1">4</td><td align="left" rowspan="1" colspan="1">3</td><td align="left" rowspan="1" colspan="1">5</td><td align="left" rowspan="1" colspan="1">4</td></tr></tbody></table>DISCUSSION
4
In our cohort, long term evaluation of Musset's surgical technique showed a success rate of 48.4% in RVF repair, with a rate of complications and reinterventions of 54.8% and 35.7%, respectively. In the patients having a recurrence of incontinence symptoms, it was mostly gas incontinence in 43.8% of cases. All the recalled patients felt a significant improvement in their quality‐of‐life following surgery and were satisfied with their operation. According to the FSFI score, the patients had satisfactory sexual intercourses postoperatively with a median score of 5.2/6 (3.4–6/6).
A study by Göttgens et al.22 recently highlighted the poor quality of the published studies concerning RVF repairs. The results are very variable, with closure rates ranging from 0% to over 80%. None of the studies are randomized and a meta‐analysis was not possible. The lack of high‐quality studies on RVF repair could be overcome by establishing expert centers that would allow appropriate multidisciplinary management with experienced surgeons and ensure prolonged follow‐up. Multidisciplinary care is important in the management of RVF since surgery should not only cure the symptoms of incontinence but also help patients to regain a normal self‐image.
The success rate in our study contrasts with that reported by Soriano et al.15 Indeed, in their cohort, among the 48 patients that underwent RVF repair by Musset's technique, 98% had a satisfactory functional result and 8.3% patients required iterative surgery. Such discrepancy could be explained by many reasons, including the number of previous interventions, the complexity of the fistulas, the etiology of the fistulas of if the intervention is done is one or two steps. In our study, 81.6% of the fistulas were obstetrical, whereas this etiology represented only 52.1% of the fistulas in the Soriano et al. study15 The study by Studniarek et al.23 found that obstetrical RVF repairs had lower success rates compared to malignant RVF (43.3% and 68.6%, respectively) and had a significantly increased risk of undergoing more than three procedures. This could be explained by the frequent association of anal sphincter injuries which can be easily overlooked.24 However, their preoperative detection may improve postoperative continence.25 Performing a rectal endoscopic ultrasound preoperatively is effective in identifying patients with concomitant anal sphincter defects (sensitivity and specificity of 100% for the external sphincter and 100% and 95.5% for the internal sphincter).26 In our study, only 17 patients out of the 38 patients benefited from this examination. Another fundamental element to explain such difference could be the prolonged follow‐up that we performed and the difference in criteria for success assessment.
Our success rate could also be explained by the choice of our criteria for success. Indeed, some patients can experience recurrence of incontinence but without a recurrence of the RVF. Factors such as menopause, aging of the sphincter, and decompensation of coping mechanisms can be responsible of delayed incontinence symptoms.27 The management of anal incontinence is complex and multifactorial and surgical repair is sometimes insufficient.
Even though incontinence symptoms persisted in the 11 patients that were recalled, they were all satisfied with their intervention and their quality of life. Indeed, concerning the satisfaction rates of our study, 10 patients described having a better life postoperatively since the procedure and all answered that they were happy with their surgery. Concerning the quality of life, it was improved postoperatively according to the Cleveland scale with a median score decreasing from 2.5 (1.5–3.75) to 0.5 (0–3.75) and there were no limitations due to physical health nor due to emotional problems according to the SF‐36 questionnaire with a median score of 100 (87.50–100) and 100 (66.65–100), respectively. The high satisfaction rate of our study could be explained by CHI Creteil's historical involvement in fistula repair and in vulvar and perineal surgeries, making it a reference center in the matter. Indeed, many patients have been operated on by Paniel et al., a leading expert in vulvar pathologies.28, 29 These results are consistent with the study of Leroy et al.13 who also recalled patients who had undergone a RVF repair by the Musset technique: three of the four patients were satisfied with their procedure, had a stable quality of life and an absence of physical and social repercussions even though a certain degree of incontinence persisted.
The sexual function score of patients having had a RVF repair was higher in our study compared to previous studies. In the study by El‐Gazzaz et al.,30 half of the patients that were recalled had regained their sexual activity postoperatively and 25.5% had dyspareunia.
The study by Studniarek et al.23 analyzed the success rate of up to 20 different surgical techniques in the repair of RVF, with an overall success rate of 37.3%. Among the procedures with the highest chance of success was 57.9% for the endorectal flap (22/38 patients), 55.2% for abdominal resections with and without proximal bypass (16/29) and 53.1% for the Musset technique (17/32). The choice of the Musset technique in RVF repairs could be based on the etiology of the fistula and could be well adapted to obstetrical fistulas since it allows a repair of the anal sphincter in the same operative time.
In the present study, some limitations are worth underlining. First, the long delay between evaluation and the time of surgery could have induced a risk of bias including recall bias with patients over‐evaluating their discomfort prior to surgery. However, a large period of inclusion was required due to the rarity of the procedure and to achieve long follow‐up. The monocentric inclusion in our tertiary referral center induces a risk of selection bias as more severe patients were referred for management, thus underestimating the benefit of this surgical technique. Indeed, in our cohort, 12 patients had undergone an attempt of RVF repair prior to the index surgery. Second, the limited number of patients, due to the rarity of this condition in occidental countries, did not permit a comparison between the incontinent and continent patients. Furthermore, 27 patients were lost to follow‐up which could be explained by the traumatic experience for these patients of having a RVF. During the visit, a patient described how traumatic this experience had been for her and how difficult it was to discuss her illness. Third, the scores used could bias the evaluation of the surgical impact. The scores used are usually based on symptoms preceding 4 weeks from the moment the patient took the test. The results of the SF‐36 and WHOQOL‐Bref scores were strongly biased with decreased results in a patient who had recently had a fetal death in utero before the study. Life events can therefore modify the scoring and are more representative of quality of life and mental health in general than post‐RVF treatment. Similarly concerning the FSFI score: two of the recalled patients had not had recent sexual relations and were therefore unable to answer all the questions. Eventually, the different questionnaires were not available prior surgery to definitely assess the state of all patients at the time they required/decided to undergo surgery.
CONCLUSION
5
The Musset technique provides good functional results with a success rate of 51.6% and a reduction in the intensity of incontinence symptoms. There were excellent satisfaction rates and an improved quality‐of‐life postoperatively. However, this repair technique is associated with a high rate of complications and reinterventions, resulting in long‐term care which should be done in referral centers in order to optimize the chances of success.
AUTHOR CONTRIBUTIONS
Planning the study—Organization—Study administration: BH, YD, GC, CT. Data collection and analysis: JB, EL, BH, CT, YD. Drafting first version of the manuscript: JB, EL, YD. Revising manuscript for critical intellectual content: all authors.
CONFLICT OF INTEREST STATEMENT
The authors declare that they do not have any conflicts of interest.
Supporting information
Appendix S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adler AJ , Ronsmans C , Calvert C , Filippi V . Estimating the prevalence of obstetric fistula: a systematic review and meta‐analysis. BMC Pregnancy Childbirth. 2013;13(1):246.24373152 10.1186/1471-2393-13-246PMC 3937166 · doi ↗ · pubmed ↗
- 2Champagne BJ , Mc Gee MF . Rectovaginal Fistula. Surg Clin North Am. 2010;90(1):69‐82.20109633 10.1016/j.suc.2009.09.003 · doi ↗ · pubmed ↗
- 3Goldaber KG , Wendel PJ , Mc Intire DD , Wendel GD . Postpartum perineal morbidity after fourth‐degree perineal repair. Am J Obstet Gynecol. 1993;168(2):489‐493.8438915 10.1016/0002-9378(93)90478-2 · doi ↗ · pubmed ↗
- 4Cowgill KD , Bishop J , Norgaard AK , Rubens CE , Gravett MG . Obstetric fistula in low‐resource countries: an under‐valued and under‐studied problem—systematic review of its incidence, prevalence, and association with stillbirth. BMC Pregnancy Childbirth. 2015;15(1):193.26306705 10.1186/s 12884-015-0592-2PMC 4550077 · doi ↗ · pubmed ↗
- 5Murray CJL , Lopez AD , Organization WH . Health Dimensions of Sex and Reproduction: the Global Burden of Sexually Transmitted Diseases, HIV, Maternal Conditions, Perinatal Disorders, and Congenital Anomalies. Boston: Harvard School of Public Health; 1998. Accessed Jul 6, 2021. https://apps.who.int/iris/handle/10665/42161
- 6Bacon C , United Nations Population Fund , Engender Health (Firm) . Obstetric fistula needs assessment report: findings from nine African countries. UNFPA: Engender Health; 2003.
- 7United Nations Population Fund . Second Meeting of the Working Group for the Prevention and Treatment of Obstetric Fistula. Accessed May 4, 2022. https://www.unfpa.org/publications/second‐meeting‐working‐group‐prevention‐and‐treatment‐obstetric‐fistula
- 8Hannaway CD , Hull TL . Current considerations in the management of rectovaginal fistula from Crohn's disease. Color Dis. 2008;10(8):747‐755.10.1111/j.1463-1318.2008.01552.x 18462243 · doi ↗ · pubmed ↗