Recurrence of Pleomorphic Adenoma in the Submandibular Gland: A Case Report and Literature Review
Zhiqiong Li, Guiying Yuan, Ye Zhang, Junbin Huang, Fan Xu, Yuchao Xiong, Xuwen Zeng

TL;DR
This case report describes the recurrence of a rare tumor in the submandibular gland and highlights its imaging features to improve diagnosis.
Contribution
The paper is the first to comprehensively describe CT and MRI imaging features of recurrent pleomorphic adenoma in the submandibular gland.
Findings
The case provides detailed CT and MRI data for a recurrent pleomorphic adenoma in the submandibular gland.
The tumor recurred 5 years after initial resection and was confirmed by postoperative pathology.
Comprehensive imaging data helps avoid misdiagnosis of this rare tumor.
Abstract
Recurrent pleomorphic adenoma (PA) in the submandibular gland is a rare tumor that may be misdiagnosed as an inflammatory lesion. The imaging manifestations of the submandibular gland recurrent PA are unclear, with only three case reports reporting CT and MRI imaging, respectively. Our report is the first case report that comprehensively describes the imaging manifestations of recurrent PA in the submandibular gland. A 28-year-old woman had a right submandibular gland pleomorphic adenoma that recurred 5 years after resection and gradually grew larger. She had no special discomfort and was diagnosed with a recurrence of pleomorphic adenoma. The patient underwent CT and MRI examinations and tumor resection, and postoperative pathology showed tumor recurrence. This case report provides substantial and comprehensive CT and MRI data, which is conducive to the diagnosis of the recurrence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
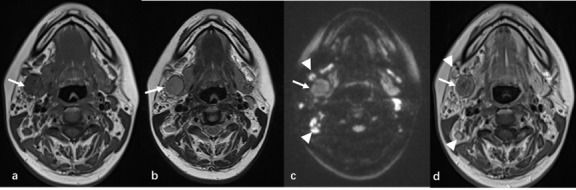 Figure 1
Figure 1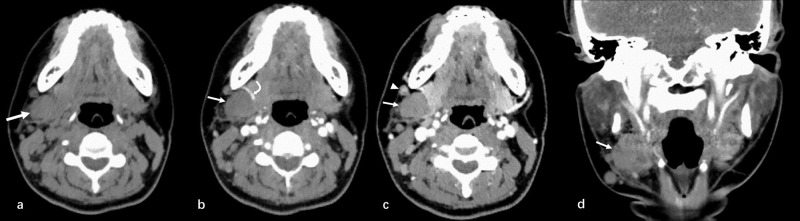 Figure 2
Figure 2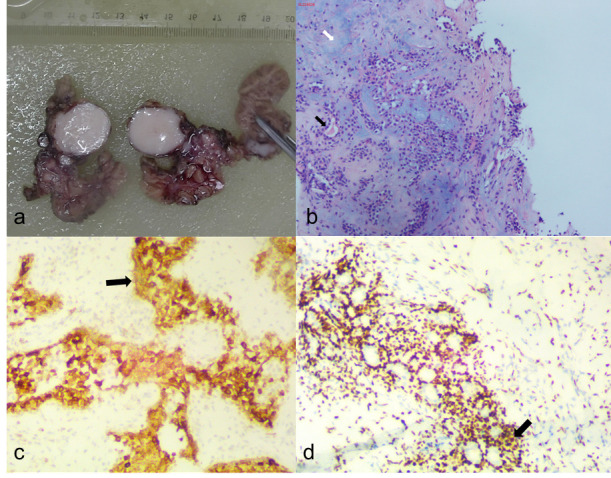 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Ear and Head Tumors · Oral and Maxillofacial Pathology
INTRODUCTION
1
Pleomorphic adenoma (PA) is the most prevalent benign salivary gland tumor, with a predilection for middle-aged females. It originates from the major salivary glands, although it may also arise from the minor salivary glands [1]. The parotid glands are the most frequently affected (85%), followed by the minor salivary (10%) and submandibular glands (5%). The recognition of PA is conceptualized by identifying three components: epithelial, myoepithelial, and mesenchymal. Epithelium in a loose fibrous stroma of myxoid, chondroid, or myxoid type shows different patterns in the histological manifestations of PA [2]. Although benign, these epithelial tumors have a tendency to relapse and become malignant if not completely resected, which can result in increased morbidity in these patients [1]. There are few imaging reports of recurrent PA in this site, and the imaging description is not detailed. Therefore, we report a case of recurrent PA in the right submandibular gland and review the literature, focusing on its imaging features, differential diagnosis, and possible factors for recurrence.
CASE REPORT
2
A 28-year-old woman was admitted to the hospital with a diagnosis of a right submandibular mass that had re-swelled 5 years after the initial surgical removal of the tumor. The patient had undergone a resection of the right submandibular mass at another hospital 10 years prior. The postoperative pathological result of this case was considered to be a mixed tumor. Five years ago, the tumor recurred for no apparent reason, approximately the size of a soybean. Thereafter, the tumor gradually increased in size, and the B-ultrasound demonstrated that the right submandibular gland was occupied by solid nodules, prompting the consideration of a mixed tumor.
A specialist physical examination revealed a localized submandibular bulge on the right side, a surgical scar of approximately 2 cm on the surface, and a palpable oval mass of 3.0×2.0 cm. It was firm, non-tender, with clear margins, an acceptable range of motion, and no surface damage, ulceration, or pus. Multiple lymph nodes were palpated in areas II and III on the right side of the neck, which had clear margins and no tenderness, with a maximum size of approximately 1.0 × 1.0 cm.
The patient underwent magnetic resonance imaging (MRI) on the first day of admission. There were multiple round nodules in the posterior and inferior regions of the right submandibular gland. T1-weighted images showed an intermediate or slightly low signal and T2-weighted images exhibited a slightly high signal. The largest was approximately 1.8×2.2×2.8 cm in size. The signal was slightly heterogeneous. Diffusion-weighted imaging (DWI) demonstrated a high signal, and apparent diffusion coefficient (ADC) mapping showed a slightly high signal. The contrast-enhanced scans exhibited non-uniform enhancement. The unenhanced necrotic area was seen in the center of the nodules, and a capsule sign appeared around it. A number of enlarged lymph nodes were observed on the right side of the neck, with notable enhancement. The largest of these was approximately 1.0 cm in size (Fig. 1). Based on the MR imaging features, a recurrence of a PA of the right submandibular gland was suspected.
On the second day, a non-contrast computed tomography (CT) of the neck and a contrast-enhanced CT of the neck were performed. Multiple round, low-density nodules were observed in the posterior and inferior regions of the right submandibular gland, some of which were clustered. The largest was about 2.3 ×1.8 cm in size. Some of the nodules exhibited clear borders, while others displayed unclear borders with the right submandibular gland. The enhancement was of a relatively mild to moderate degree and exhibited slight unevenness. The adjacent cervical fascia was slightly thickened. Multiple scattered enlarged lymph nodes were seen on the right side of the neck, ranging from approximately 0.3 to 1.1 cm in diameter. The enhancement was not homogeneous (Fig. 2). Based on the CT imaging characteristics, tumor recurrence was considered.
On day 2, a puncture biopsy of the right submandibular gland tumor was performed. The result was a PA of the right submandibular gland. The patient underwent “right submandibular gland and mass resection, cervical lymph nodes resection and arbitrary skin flap arthroplasty” in our hospital. The greyish-red submandibular gland tissue was sent for examination, and through the incision, multiple greyish-white solid nodules with tough, clear borders and maximum diameters of 0.5 cm-2.5 cm were seen (Fig. 3).
Under the microscope, multiple nodules were seen, with nodules of different sizes and fibrous capsules. They were composed of epithelium, myoepithelial-like cells, mucus, and bone-like matrix (Fig. 3). The cells were arranged in glandular or sheet-like shapes, and some epithelial cells were actively proliferating. Some epithelial proliferation was active with mild to moderate atypical hyperplasia. In some regions, fibrous tissue hyperplasia and hyaline degeneration involved surrounding adipose tissue and muscle fibers. In some of the lymph nodes sent for examination, residual lymphoid tissue was found around the tumor, and it was highly suspected that the tumor involved the lymph nodes. Immunohistochemical analysis revealed P63 (+), S100 (+), GFAP (-), CK (Pan) (+), BCL-2 (+), SMA (-/+), P53 (about 20%+), and Ki-67 (about 5%+). The pathological diagnosis of the right submandibular gland tumor was a PA (recurrent, multifocal distribution). This PA was accompanied by mild to moderate atypical hyperplasia and had malignant potential with the possibility of malignant transformation and metastasis.
DISCUSSION
3
PA is the most common benign tumor of the submandibular gland. The preferred treatment for PA of the submandibular gland is “complete” resection of the tumor and the affected submandibular gland. The good postoperative oncologic outcome of PA of the submandibular gland contrasts with the well-known great risk of recurrence of PA of the parotid gland. Recurrence of PA in the submandibular gland is rare, and Mantsopoulos [3, 4] reported a total of 147 cases of PA in the submandibular gland, none of which recurred. Due to its rarity, imaging manifestations have not been systematically reported.
To the best of our knowledge, only 15 cases of pathologically confirmed recurrent PA in the submandibular gland have been reported in the English literature [5-9], and only 3 of them mentioned the imaging manifestations of recurrent PA in the submandibular gland. Grabovac [6] and Yasumoto [9] reported only the CT manifestations of recurrent PA in the submandibular gland, and İnan [7] reported only the MRI manifestations of recurrent PA. Our report is the first case report that comprehensively describes the imaging manifestations of recurrent PA in the submandibular gland.
Most reported primary PA tumors are solitary masses [10], but recurrent PA tumors often present as multiple nodules, whether they occur in the parotid gland or submandibular gland. Phillips et al. [9a] reported 126 patients with recurrent parotid PA, of whom 85 (67.4%) presented with multinodular lesions. Two previously reported [6, 7] cases of recurrent PA occurring in the submandibular gland also showed multi-nodularity, and the imaging of the present case was consistent with the previous reports, showing a multinodular lesion. Recurrent PA of the parotid gland presenting as multinodular is thought to be associated with pseudocapsular rupture and inadvertent tumor spillage. Therefore, it is suggested that recurrent submandibular PA presenting as multinodular may be similarly associated with pseudocapsular rupture and inadvertent tumor spillage [11]. In addition, the possibility of recurrence in the glandular and ductal tissue surrounding the submandibular gland cannot be ruled out.
Primary PA has well-defined borders, and lesions are usually lobulated [10]. Yasumoto et al. [9] stated that recurrent PAs, like most primary tumors, have clear contours and smooth margins. However, in this case, most borders of the tumor were clear, and a small portion of the borders were unclear. Therefore, the pathology suggested that this case was accompanied by mild to moderate atypical hyperplasia with some malignant potential. Therefore, when the borders of recurrent PA are unclear, one should be alert to the possibility of malignancy. The recurrent PA, in this case, showed a slightly higher signal on T2-weighted images, which was not consistent with the apparent high signal on T2 shown in the images provided in the case report by İnan et al. [7]. This may be due to different tissue subtypes. Histopathologically, PA can be classified into three types: mucinous (or stroma-rich), cellular, and classic [3]. Among recurrent PA, the myxoid subtype has been shown to be the most prevalent, with myxoid material showing a markedly high signal on T2WI, whereas the other types, with a lower proportion of myxoid material, may show a slightly higher signal on T2WI.
An enhancement pattern was recorded only in 1 case of recurrent PA in the submandibular gland after intravenous contrast injection, which showed inhomogeneous enhancement [7]. The pattern of enhancement in our reported case was a partial inhomogeneous enhancement, as reported in previous reports. This pattern supported our pathologic findings. The pathologic findings showed fibrosis and necrosis in some of the lesions. This was also consistent with the previously reported pathologic findings of recurrent PA multi-nodularity in the parotid gland, i.e., the enhancement patterns showed a variety of findings ranging from solid, homogeneous, and heterogeneous to marginal enhancement (cystic pattern) [11].
Nodular lesions in the submandibular gland region are increasingly being detected in radiologic practice due to the increasing number of routine images. Recurrent PA is a type of nodule, but diagnostic imaging is challenging due to its rarity and lack of definitive imaging features. The differential diagnosis of recurrent PA includes lymphoepithelial carcinoma of the submandibular gland [12], adenoid cystic carcinoma [13], lymph node tuberculosis [14], and lymphoma [15]. The diagnosis of lymphoepithelial carcinoma of the submandibular gland and adenoid cystic carcinoma is prioritized if most of the nodal borders are indistinct. If most of the nodules show uneven peripheral enhancement and there is a history of tuberculosis, lymph node tuberculosis may be a priority. If multiple nodules in the submandibular gland region exhibit uniform density or signal and are associated with a history of Sjögren's syndrome, lymphoma may be prioritized [15].
Radiotherapy for the recurrence of pleomorphic adenomas has become a topic of consideration for scholars. Witt et al. summarized local tumor control after postoperative radiotherapy. Radiotherapy seems to improve the treatment outcomes of patients with multinodular tumors with multiple recurrences [16]. However, conclusions about the indications for radiotherapy are difficult to summarize. The side effects of radiotherapy and whether radiotherapy will induce the growth of other nodules in the future should also be considered. K. Aro et al. speculated that more extensive utilization of postoperative radiotherapy may delay further recurrences and suggested that postoperative radiotherapy appears to be necessary for patients with multifocal recurrent disease [17]. However, radiotherapy was not performed in our case.
CONCLUSION
In conclusion, if the lesions in the submandibular gland area are multinodular and the pattern of enhancement varies from one nodule to another, recurrent PA should be included in the differential diagnosis. It is advisable to conduct a thorough history and physical examination to ascertain the patient's medical history and to elicit any pertinent information that may assist in making an accurate diagnosis.
AUTHORS’ CONTRIBUTION
The authors confirm their contribution to the paper as follows: study conception and design: ZQL, YCX, and XWZ; data collection: GYY, YZ, and JBH; analysis and interpretation of results: ZQL, GYY, and FX; draft manuscript: ZQL.
All authors reviewed the results and approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kalwaniya D.S. Meena R. Kumar D. A review of the current literature on pleomorphic adenoma.Cureus.2023157 e 4231110.7759/cureus.4231137614271 PMC 10442517 · doi ↗ · pubmed ↗
- 2Matsumiya-Matsumoto Y. Morita Y.A.-O. Uzawa N. Pleomorphic adenoma of the salivary glands and epithelial-mesenchymal transition.J. Clin. Med.20221114421010.3390/jcm 1114421035887973 PMC 9324325 · doi ↗ · pubmed ↗
- 3Mantsopoulos K. Goncalves M. Koch M. Submandibular gland pleomorphic adenoma: Histopathological capsular characteristics and correlation with the surgical outcome.Ann. Diagn. Pathol.20183416616910.1016/j.anndiagpath.2018.04.00229689463 · doi ↗ · pubmed ↗
- 4Mantsopoulos K.A.-O. Goncalves M. Schapher M. Long-term oncologic and functional outcome in pleomorphic adenomas of the submandibular gland.Laryngos. Investig. Otolaryngol.20172636937210.1002/lio 2.11329299510 PMC 5743162 · doi ↗ · pubmed ↗
- 5Alzumaili B. Xu B. Saliba M. Clinicopathologic characteristics and prognostic factors of primary and recurrent pleomorphic adenoma: a single institution retrospective study of 705 cases.Am. J. Surg. Pathol.46685486210.1097/PAS.000000000000183734772841 PMC 9106806 · doi ↗ · pubmed ↗
- 6Grabovac S. GrabovacĐ. PuharićZ. Relapse of pleomorphic adenoma from childhood to adulthood: Case report.Acta. Clin. Croat.201756481281610.20471/acc.2017.56.04.3329590741 · doi ↗ · pubmed ↗
- 7İnan S. Aydın E. Babakurban S.T. Recurrent pleomorphic adenoma of the submandibular gland.Turk. Arch. Otorhinolaryngol.2016541434610.5152/tao.2016.128129392015 PMC 5782975 · doi ↗ · pubmed ↗
- 8Jackson S.R. Roland N.J. Clarke R.W. Jones A.S. Recurrent pleomorphic adenoma.J. Laryngol. Otol.1993107654654910.1017/S 00222151001236678393908 · doi ↗ · pubmed ↗