TREX1, a predator for treating MSI‐H tumors?
Elena Benidovskaya, Joséphine Deneft, Marc Van den Eynde

TL;DR
TREX1 helps MSI-H tumors avoid immune detection by degrading DNA, and blocking it could improve immunotherapy responses.
Contribution
The study identifies TREX1 as a novel target for enhancing immunotherapy in MSI-H tumors.
Findings
TREX1 degrades cytosolic DNA and suppresses the cGAS–STING–IFN-I pathway in MSI-H tumors.
Loss of TREX1 promotes immune cell infiltration and antitumor immunity.
Targeting TREX1 could overcome resistance to immune checkpoint blockade.
Abstract
Immunotherapy has revolutionized cancer treatment; yet, a subset of patients with microsatellite instability‐high (MSI‐H) tumors fails to respond to treatment despite their elevated tumor mutational burden and immunogenic potential. In a recent study, Xu et al. uncover a key mechanism of immune evasion in MSI‐H tumors mediated by the exonuclease TREX1, which degrades cytosolic DNA and suppresses activation of the cyclic GMP‐AMP synthase—stimulator of interferon genes (cGAS‐STING)—type I interferon pathway. Loss of TREX1 restores cytosolic DNA sensing, promotes CD8+ T and NK cell infiltration, and enhances antitumor immunity. These findings highlight TREX1 as a potential therapeutic target to overcome resistance to immune checkpoint blockade. Immunotherapy benefits many patients; yet, some with MSI‐H tumors remain unresponsive despite their high immunogenicity. Xu et al. reveal that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1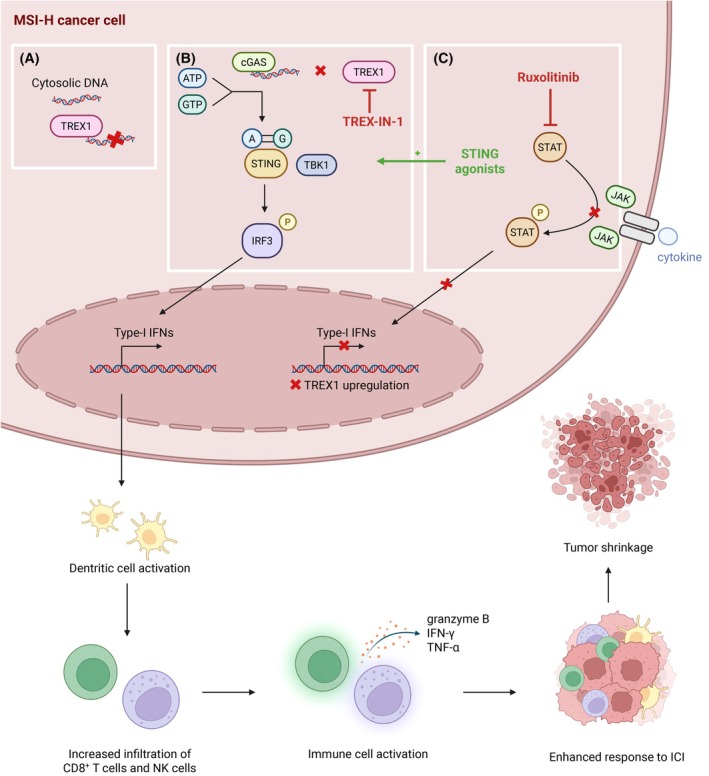 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
Topicsinterferon and immune responses · Ferroptosis and cancer prognosis · Cytokine Signaling Pathways and Interactions
In recent years, immunotherapy has emerged as a promising therapeutic strategy in oncology, offering durable clinical responses in several cancer types by harnessing the body's immune system to target cancer cells. Among these approaches, immune checkpoint inhibitors (ICI), targeting molecules such as programmed death protein 1 (PD‐1), programmed death‐ligand 1 (PD‐L1), or cytolytic T‐lymphocyte associated protein 4 (CTLA‐4), have shown remarkable efficacy in tumors with high levels of immune infiltration and genomic instability [1].
Patients with high microsatellite instability (MSI‐H) tumors demonstrate significantly improved responses to immunotherapy and overall survival compared to patients with microsatellite‐stable (MSS) tumors [2]. This improved sensitivity is largely attributed to the elevated tumor mutational burden (TMB) characteristic of MSI‐H tumors, which leads to the generation of numerous neoantigens capable of eliciting robust antitumor immune responses [3].
However, despite their immunogenic potential, a subset of MSI‐H patients fails to benefit from immunotherapy. The mechanisms underlying this resistance remain poorly understood, suggesting that factors beyond TMB, such as the composition and functional state of tumor‐infiltrating and circulating immune cells, may play critical roles in modulating treatment efficacy. Understanding these immune determinants is essential to identify biomarkers predictive of response and to optimize patient selection for immunotherapy [4].
To overcome this limitation, various strategies are currently being explored to enhance the immunogenicity of these tumors and improve patient outcomes. These include combination approaches integrating immunotherapy with chemotherapy, radiotherapy, targeted agents, or novel immunomodulatory treatments aimed at reshaping the tumor microenvironment [5, 6, 7].
In this context, Xu et al. investigated the mechanisms by which MSI‐H tumors might evade immune surveillance [8]. They proposed that three‐prime repair exonuclease 1 (TREX1) could play a key role by degrading cytosolic DNA, which accumulates in tumors with genomic instability, thereby preventing activation of the cGAS‐STING pathway and the subsequent adaptive antitumor immune response. Consistently, they demonstrated that MSI‐H tumors exhibit elevated intrinsic TREX1 expression. Loss of TREX1 in those tumors results in tumor‐intrinsic type I interferon (IFN‐I) activation, increased infiltration of CD8^+^ T and natural killer (NK) cells in a dendritic cell (DC)‐dependent manner, and consequent tumor regression (Fig. 1). Conversely, IFN‐I treatment induces TREX1 expression, forming a negative feedback loop that dampens cGAS‐STING pathway activation. This tumor‐intrinsic mechanism ultimately contributes to immune evasion in MSI‐H tumors. Notably, this regulation can be reversed by ruxolitinib, which downregulates TREX1 through JAK/STAT pathway inhibition. They also demonstrated that the infiltrating CD8^+^ T cells displayed activation markers such as CD69, CD44, and CD28, together with reduced expression of exhaustion markers PD‐1 and T‐cell immunoglobulin and mucin‐domain containing‐3. Moreover, these tumor‐infiltrating T cells exhibited increased levels of granzyme B, IFN‐γ, TNF‐α, and IL‐2–STAT5 signaling, consistent with a robust cytotoxic and activated phenotype.
The results of this study suggest new therapeutic avenues for the treatment of MSI‐H tumors. TREX1 inhibition could be combined with existing immunotherapies to enhance patient responses and improve survival. The authors demonstrated that TREX1‐IN‐1 (specific inhibitor) suppresses tumor growth in MLH1‐deficient tumors by stimulating CD8^+^ T cell–mediated antitumor immunity. This study adds to a growing body of work exploring TREX1 as a potential modulator of immunotherapy and chemotherapy efficacy by enhancing T‐cell infiltration in cold tumors [9, 10, 11].
Although promising, TREX1‐IN‐1 has not yet been validated clinically. Ruxolitinib, a clinically approved JAK1/2 inhibitor for the treatment of myeloproliferative syndromes, to inhibit IFN‐I signaling and thereby prevent TREX1 upregulation in an MLH1‐dependent manner, could be used. The combination of nivolumab and ruxolitinib in 19 patients with Hodgkin lymphoma showed promising results with a best overall response rate of 53%, a lower infiltration in myeloid suppressive cells inside the tumor and an increase of activated T‐cell infiltration [12]. However, its benefit in solid tumors remains to be established. Xu et al. explored the possibility of modulating TREX1 expression through JAK/STAT pathway inhibition (e.g., with ruxolitinib) but they emphasized that IFN signaling remains essential for immune‐mediated tumor rejection in MSI‐H/dMMR tumors. Thus, while JAK inhibitors may have complex immunomodulatory effects in certain contexts, their use in MSI‐H tumors warrants cautious evaluation. Other strategies targeting different components of the cGAS–STING pathway, such as the development of STING agonists or modulators of downstream signaling molecules, are also being investigated in preclinical and clinical settings, further supporting the therapeutic potential of this pathway in cancer immunotherapy (Fig. 1). Yet, clinical responses have so far been modest, highlighting the need for improved delivery systems or combination strategies to fully exploit the therapeutic potential of this pathway [13, 14].
This study sheds light on the mechanisms underlying immune escape in MSI‐H tumors, highlighting the pivotal role of TREX1 in regulating the cGAS–STING pathway. These findings open new therapeutic perspectives aimed at modulating immune responses in MSI‐H cancers refractory to current immunotherapy approaches.
Nonetheless, MSI‐H tumors account for a minority of cancer cases, with most patients presenting MSS tumors. These tumors are characterized by a low TMB but display chromosomal instability, which has also been associated with the accumulation of genomic DNA in the cytosol. Therefore, collective efforts should be focused on elucidating the role of TREX1 and of the cGAS–STING pathway in this tumor subtype, which is crucial to extend the potential therapeutic benefit of immune checkpoint inhibitors to the larger group of patients who remain resistant to current immunotherapy strategies [15].
Conflict of interest
The authors declare no conflict of interest.
Author contributions
EB, JD, and MVdE have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zugazagoitia J , Guedes C , Ponce S , Ferrer I , Molina‐Pinelo S , Paz‐Ares L . Current challenges in cancer treatment. Clin Ther. 2016;38:1551–1566.27158009 10.1016/j.clinthera.2016.03.026 · doi ↗ · pubmed ↗
- 2Le DT , Durham JN , Smith KN , Wang H , Bartlett BR , Aulakh LK , et al. Mismatch repair deficiency predicts response of solid tumors to PD‐1 blockade. Science. 2017;357:409–413.28596308 10.1126/science.aan 6733 PMC 5576142 · doi ↗ · pubmed ↗
- 3Germano G , Lamba S , Rospo G , Barault L , Magrì A , Maione F , et al. Inactivation of DNA repair triggers neoantigen generation and impairs tumour growth. Nature. 2017;552:116–120.29186113 10.1038/nature 24673 · doi ↗ · pubmed ↗
- 4Bruni D , Angell HK , Galon J . The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat Rev Cancer. 2020;20:662–680.32753728 10.1038/s 41568-020-0285-7 · doi ↗ · pubmed ↗
- 5Huyghe N , Benidovskaya E , Masoodi T , Sinapi I , De Cuyper A , Vempalli F , et al. Impact of the tumor immune contexture in microsatellite‐stable metastatic colorectal cancer treated with avelumab, cetuximab, and irinotecan. Cell Rep Med. 2025;6:102201.40562041 10.1016/j.xcrm.2025.102201 PMC 12281371 · doi ↗ · pubmed ↗
- 6Raimondi A , Lonardi S , Murgioni S , Cardellino GG , Tamberi S , Strippoli A , et al. Tremelimumab and durvalumab as neoadjuvant or non‐operative management strategy of patients with microsatellite instability‐high resectable gastric or gastroesophageal junction adenocarcinoma: the INFINITY study by GONO. Ann Oncol. 2025;36:285–296.39637944 10.1016/j.annonc.2024.11.016 · doi ↗ · pubmed ↗
- 7Weichselbaum RR , Liang H , Deng L , Fu Y‐X . Radiotherapy and immunotherapy: a beneficial liaison? Nat Rev Cancer. 2017;14:365–379.10.1038/nrclinonc.2016.21128094262 · doi ↗ · pubmed ↗
- 8Xu Y , Zhou Z , Chen W , du F , Huang S , Qi J , et al. Tumors with microsatellite instability upregulate TREX 1 to escape antitumor immunity. J Exp Med. 2025;222:e 20250265.41055714 10.1084/jem.20250265 · doi ↗ · pubmed ↗