Invasive Bladder Cancer With Peritoneal Invasion and Rectal Involvement Causing Rectal, Bilateral Ureteral, and Common Bile Duct Obstruction Without a Retroperitoneal Mass: A Case Report
Kazuto Imai, Norihiko Masuda, Tatsuya Hazama, Toshihide Hosomi, Keita Hanada, Takakazu Matsushita, Toshiya Akao

TL;DR
A case of invasive bladder cancer causing multiple obstructions is reported, highlighting unusual complications and treatment considerations.
Contribution
This case report highlights an unusual presentation of bladder cancer with rectal and biliary obstruction, emphasizing the importance of diagnostic and therapeutic strategies.
Findings
Bladder cancer can cause rectal, ureteral, and biliary obstructions without retroperitoneal mass.
Biliary drainage allowed initiation of systemic therapy in the presence of biliary obstruction.
Enfortumab vedotin use was avoided due to safety concerns in biliary obstruction.
Abstract
Bladder cancer (BC) is rarely associated with common bile duct (CBD) obstruction. We report a case of BC with peritoneal invasion and rectal involvement complicated by bilateral ureteral and biliary obstruction. A 77‐year‐old man presented with abdominal pain. Imaging revealed a bladder tumor with suspected muscle invasion, rectal obstruction, and bilateral hydronephrosis. Urothelial carcinoma was confirmed after transurethral resection of the bladder. Following the operation, the patient developed cholangitis with CBD obstruction, and in the absence of direct invasion or mass‐like lesions suggestive of malignant retroperitoneal fibrosis, retroperitoneal extension was considered a possible mechanism. Safety concerns regarding enfortumab vedotin in the setting of biliary obstruction led us to administer pembrolizumab monotherapy. BC may contribute to biliary obstruction through…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
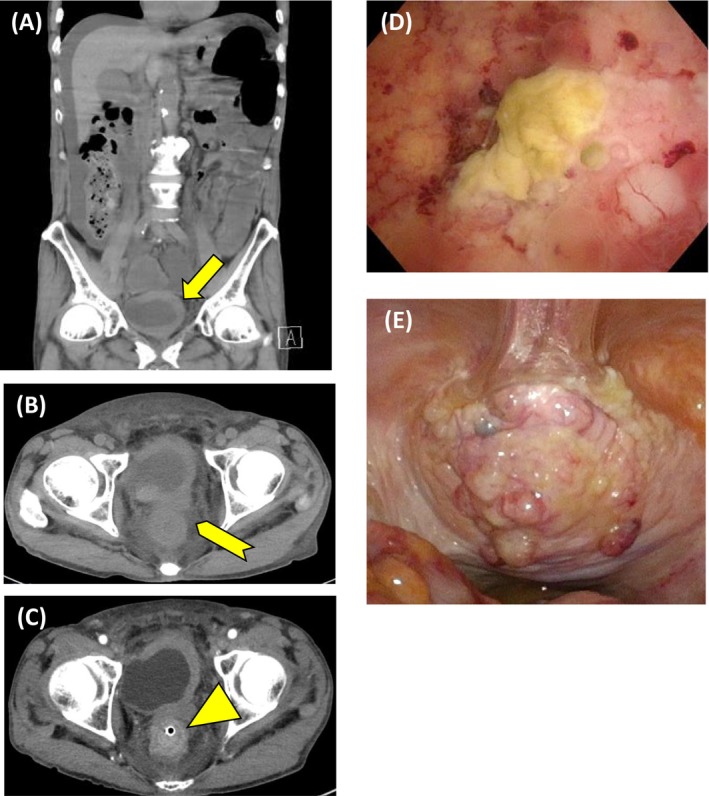 FIGURE 1
FIGURE 1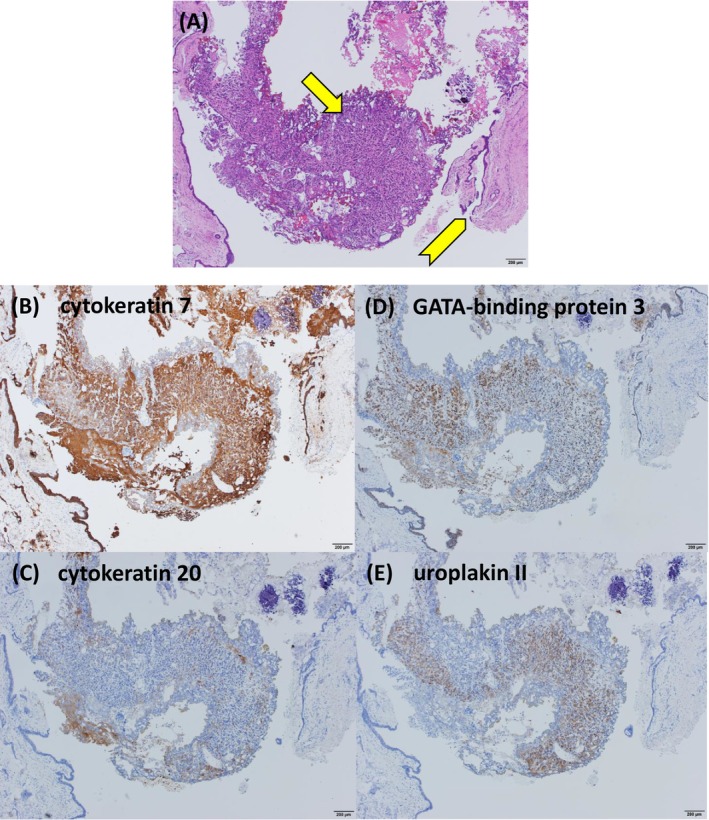 FIGURE 2
FIGURE 2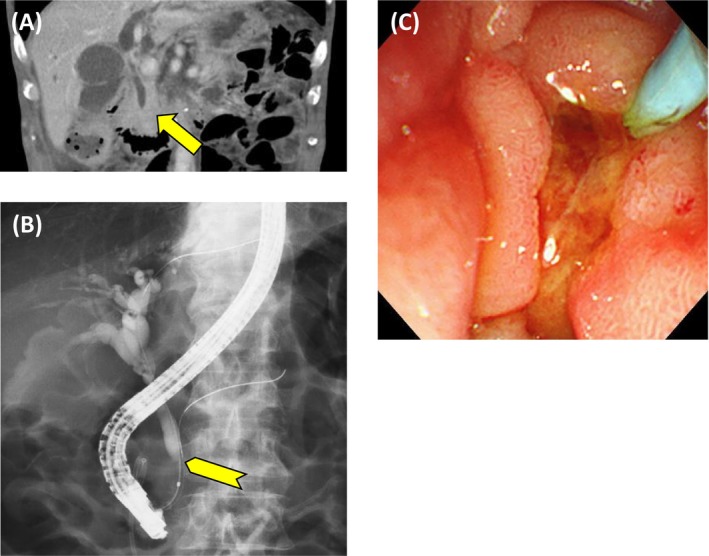 FIGURE 3
FIGURE 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Gallbladder and Bile Duct Disorders · Cholangiocarcinoma and Gallbladder Cancer Studies
Introduction
1
Bladder cancer (BC) typically progresses via direct invasion or lymphatic and hematogenous spread and has rarely been reported in association with common bile duct (CBD) obstruction. We report a case of BC with peritoneal invasion and rectal involvement complicated by bilateral ureteral and biliary obstruction.
Case Presentation
2
A 77‐year‐old man presented with abdominal pain. Abdominal computed tomography (CT) revealed a bladder tumor extending from the dome to the left lateral wall, with suspected muscle invasion and left hydronephrosis (Figure 1A), along with increased perirectal fat density, rectal wall thickening causing obstruction, and ascites (Figure 1B). No evidence of lymph node metastasis was observed. Because of the rectal obstruction, the patient was admitted and underwent colonoscopy followed by transanal decompression tube placement. Colonoscopy showed edematous mucosa at the site of rectal obstruction, and biopsy showed carcinoma with unclear mucosal architecture and differentiation, precluding identification of the primary site. Contrast‐enhanced CT on hospital day 3 revealed the development of right hydronephrosis, as well as rectal wall alternating hypo‐ and hyperenhancement, showing a malignant target sign (Figure 1C) [1]. Cystoscopy showed a patent right ureteral orifice and a partially necrotic mass predominantly involving the bladder dome (Figure 1D). Voided urine cytology was positive for malignancy. Serum carbohydrate antigen 125 (CA125), carbohydrate antigen 19–9 (CA19‐9), and Span‐1 levels were markedly elevated, whereas immunoglobulin G and immunoglobulin G4 levels were within normal range. Upper gastrointestinal endoscopy and abdominal ultrasonography revealed no evidence of gastric or pancreatic cancer. Urachal carcinoma, primary bladder adenocarcinoma, and urothelial carcinoma (UC) with glandular differentiation were considered in differential diagnosis. Transurethral resection of the bladder tumor (TUR‐BT), right ureteral stent placement, and laparoscopic sigmoid colostomy were performed on hospital day 6. Tumor invasion extending to the peritoneum was apparent (Figure 1E). No disseminated nodules were observed. Histopathological examination of the TUR‐BT specimen revealed solid and isolated invasive proliferation on a background of urothelium, with no variant histology identified (Figure 2A). No cystic components or glandular structures suggestive of urachal carcinoma or primary bladder adenocarcinoma were identified. Immunohistochemical staining showed positivity for cytokeratin 7, cytokeratin 20, GATA‐binding protein 3, and uroplakin II and negativity for caudal type homeobox 2, consistent with UC (Figure 2B–E). Cytology of ascites fluid and the rectal biopsy specimen demonstrated similar immunostaining patterns. Based on these findings, the patient was diagnosed with BC with peritoneal invasion, accompanied by malignant ascites and rectal involvement. Following the operation, the patient exhibited increased hepatobiliary enzyme levels, including aspartate aminotransferase, alanine aminotransferase, and gamma‐glutamyl transpeptidase (γ‐GTP), reaching a maximum of Common Terminology Criteria for Adverse Events (CTCAE) Grade 4. Contrast‐enhanced CT revealed obstructive cholangitis secondary to CBD obstruction, with no evidence of direct invasion or mass‐like lesions indicative of malignant retroperitoneal fibrosis. (Figure 3A). Endoscopic retrograde cholangiopancreatography demonstrated beak‐like narrowing of the bile duct, suggestive of external compression (Figure 3B), along with poor duodenal dilatation and edematous mucosa of the major duodenal papilla (Figure 3C). No endoscopic findings suggested cholangiocarcinoma, and bile duct cytology was negative. After biliary stenting, hepatobiliary enzyme abnormalities improved overall, with only γ‐GTP remaining mildly elevated at CTCAE Grade 2. The patient's Eastern Cooperative Oncology Group (ECOG) performance status (PS) was 1 at the initial presentation; however, it progressively deteriorated due to cancer progression and did not improve after biliary stenting. On postoperative day 44, at the time of initiation of systemic therapy, the ECOG PS had declined to 3, and the estimated glomerular filtration rate calculated using the Cockcroft–Gault formula was 24.4 mL/min. Based on these considerations, pembrolizumab monotherapy was initiated. Systemic therapy was ineffective, and the patient died of cancer on postoperative day 57.
Abdominal CT revealed a bladder tumor extending from the dome to the left lateral wall, with suspected muscle invasion and left hydronephrosis (A, arrow), along with increased perirectal fat density, rectal wall thickening causing obstruction, and ascites (B, arrowhead). Contrast‐enhanced CT on hospital day 3 revealed the rectal wall alternating hypo‐ and hyperenhancement (C, triangle). Cystoscopy showed a partially necrotic mass predominantly involving the bladder dome (D). Tumor invasion extending to the peritoneum was apparent (E).
Histopathological examination of the TUR‐BT specimen revealed solid and isolated invasive proliferation (arrow) on a background of urothelium (arrowhead), with no variant histology identified (A). Immunohistochemical staining was positive for cytokeratin 7, cytokeratin 20, GATA‐binding protein 3, and uroplakin II, sequentially in that order (B–E).
Contrast‐enhanced imaging revealed obstructive cholangitis secondary to CBD obstruction, with no evidence of direct invasion or mass‐like lesions indicative of malignant retroperitoneal fibrosis (A, arrow). Endoscopic retrograde cholangiopancreatography demonstrated beak‐like narrowing of the bile duct, suggestive of external compression (B, arrowhead), along with poor duodenal dilatation and edematous mucosa of the major duodenal papilla (C).
Discussion
3
BC typically progresses via direct invasion or lymphatic and hematogenous spread, commonly affecting the lymph nodes, lungs, and peritoneum [2, 3]. Progression along the cavity or membranous structures surrounding the bladder, rectum, or retroperitoneum without formation of a discrete mass is rare [4]. In our case, the left ureter was obstructed, likely owing to direct invasion. Although imaging did not demonstrate obvious involvement of the rectum, right ureter, or CBD, histology confirmed UC in the rectum, and extrinsic tumor compression was suspected in the right ureter and CBD. On contrast‐enhanced CT, bladder and rectal wall thickening with alternating rectal wall enhancement suggests malignant rectal involvement [1]. In our patient, malignant retroperitoneal fibrosis as the cause of CBD obstruction could not be excluded; however, no typical retroperitoneal mass was observed. Alternatively, biliary obstruction may have resulted from retroperitoneal extension of BC along the retromesenteric plane, which surrounds the CBD and extends to the pelvis [5]. In this case, endoscopic drainage was performed for biliary obstruction. However, although malignant ascites was present, there was no definitive evidence of peritoneal dissemination; therefore, drainage by surgical bypass may also be considered depending on the clinical context.
Tumor markers associated with adenocarcinoma, such as CA125 and CA19‐9, are frequently elevated in urachal carcinoma [6]. In our case, histopathological and immunohistochemical findings supported the diagnosis of UC [7]; however, because radical cystectomy was not performed and the evaluation was limited to TUR‐BT specimens, the possibility that urachal carcinoma or adenocarcinoma components were not detected cannot be excluded.
Both the 2025 European Association of Urology and National Comprehensive Cancer Network guidelines recommend enfortumab vedotin plus pembrolizumab (EVP) as first‐line therapy for unresectable UC [8, 9]. In our case, although the patient was considered platinum‐unfit due to impaired renal function and an ECOG PS of 3, the KEYNOTE‐A39 trial exclusion criteria were not met; therefore, EVP was initially considered [10]. Enfortumab vedotin (EV) is a Nectin‐4–targeting antibody–drug conjugate containing monomethyl auristatin E (MMAE). MMAE is metabolized in the liver and is excreted via the bile [11, 12]. A case of Stevens–Johnson syndrome after EV treatment in a patient with liver cirrhosis has been reported, and patients with mild hepatic impairment show moderately increased exposure to free MMAE; however, a clear association between hepatic dysfunction and the effects of EV has not been established [13, 14]. In our patient, safety concerns regarding EV in the setting of biliary obstruction led us to administer pembrolizumab monotherapy.
This case demonstrates a rare progression pattern of UC, emphasizing the need to consider atypical modes of tumor spread in advanced disease. Furthermore, biliary drainage enabled the initiation of systemic therapy, highlighting the importance of appropriate supportive intervention in such complex cases.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. J. Gollub , M. B. Schwartz , and J. Shia , “Scirrhous Metastases to the Gastrointestinal Tract at CT: The Malignant Target Sign,” AJR 192 (2009): 936–940.19304697 10.2214/AJR.08.1152 PMC 3712505 · doi ↗ · pubmed ↗
- 2S. Liu , X. Chen , and T. Lin , “Lymphatic Metastasis of Bladder Cancer: Molecular Mechanisms, Diagnosis and Targeted Therapy,” Cancer Letters 505 (2021): 13–23.33610730 10.1016/j.canlet.2021.02.010 · doi ↗ · pubmed ↗
- 3A. Wallmeroth , U. Wagner , H. Moch , et al., “Patterns of Metastasis in Muscle‐Invasive Bladder Cancer (p T 2‐4): Au Autopsy Study on 367 Patients,” Urologia Internationalis 62 (1996): 69–75.10.1159/00003036110461106 · doi ↗ · pubmed ↗
- 4K. Tokunaga , A. Furuta , S. Arizono , et al., “Duodenal Obstruction Induced by Retroperitoneal Progression of Bladder Cancer: A Report of Two Cases,” Abdom Radiol (NY) 44 (2019): 1223–1229.30600382 10.1007/s 00261-018-1874-8 · doi ↗ · pubmed ↗
- 5T. Tirkes , K. Sandrasegaran , A. A. Patel , et al., “Peritoneal and Retroperitoneal Anatomy and Its Relevance for Cross‐Sectional Imaging,” Radiographics 32 (2012): 437–451.22411941 10.1148/rg.322115032 · doi ↗ · pubmed ↗
- 6L. E. Stokkel , H. H. van de Rossum , M. W. Kamp , et al., “Clinical Value of Preoperative Serum Tumor Markers CEA, CA 19‐9, CA 125, and CA 15‐3 in Surgically Treated Urachal Cancer,” Urologic Oncology 41 (2023): 326.e 17‐24.10.1016/j.urolonc.2023.01.01836813613 · doi ↗ · pubmed ↗
- 7R. Kumar , S. Harilal , M. A. Abdelgawad , M. M. Ghoneim , A. Kumar , and B. Mathew , “Urachal Carcinoma: The Journey So Far and the Road Ahead,” Pathology, Research and Practice 243 (2023): 154379.36821941 10.1016/j.prp.2023.154379 · doi ↗ · pubmed ↗
- 8“European Association of Urology: Guideline on Muscle‐Invasive and Metastatic Bladder Cancer,” https://uroweb.org/guidelines/muscle‐invasive‐and‐metastatic‐bladder‐cancer.