Efficacy and safety of a Venus A valve among Chinese patients undergoing transcatheter aortic valve replacement: a systematic review and single-arm meta-analysis
Zeyu Sun, Dongkai Shan, Jing Wang, Bo Jiang, Tao Chen, Yingqian Zhang, Tianwen Han, Weiran Wang, Jun Guo, Changfu Liu

TL;DR
This study evaluates the effectiveness and safety of the Venus A valve for heart valve replacement in Chinese patients, finding it generally safe with good results.
Contribution
The study provides a meta-analysis of the Venus A valve's performance in Chinese patients, offering insights into its efficacy and safety in this specific population.
Findings
The device success rate was 90%, with significant improvement in heart valve function.
At 30 days, all-cause mortality was 3%, and complications like stroke and bleeding were rare.
Despite a 12% need for a second valve, the Venus A valve showed low complication rates and good hemodynamic outcomes.
Abstract
The Venus A valve is a first-generation self-expanding valve used in China for transcatheter aortic valve replacement (TAVR). However, data on its efficacy and safety remain limited. The present study assessed the efficacy and safety of the Venus A valve in Chinese patients undergoing TAVR. A single-arm meta-analysis was performed, and relevant studies were systematically retrieved from PubMed, Embase, Web of Science, the Cochrane Library, ClinicalTrials.gov, and Google Scholar from inception until 1 June 2022. Domestic libraries were not searched due to data overlap. All study types evaluating the Venus A valve were considered for inclusion, except case reports or reviews. Non-English language studies or those without corresponding data were excluded. The Newcastle–Ottawa scale (NOS) was used to evaluate the included retrospective studies, and the methodological index for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
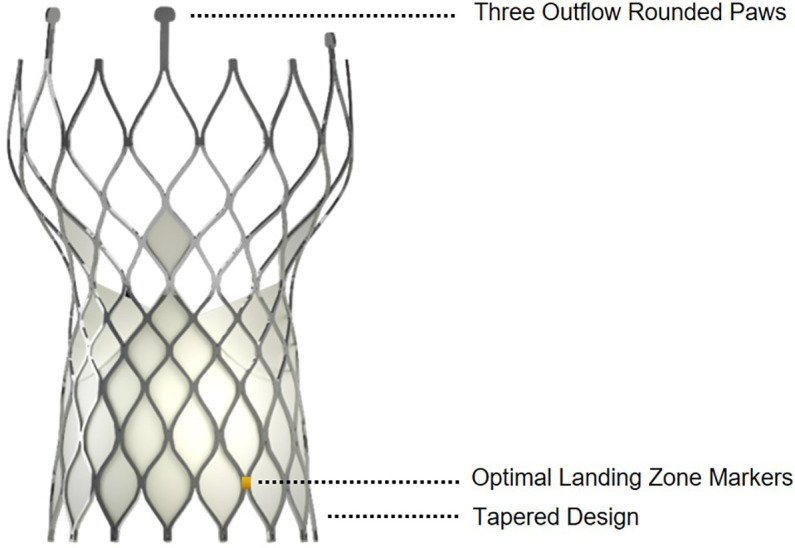 Figure 1
Figure 1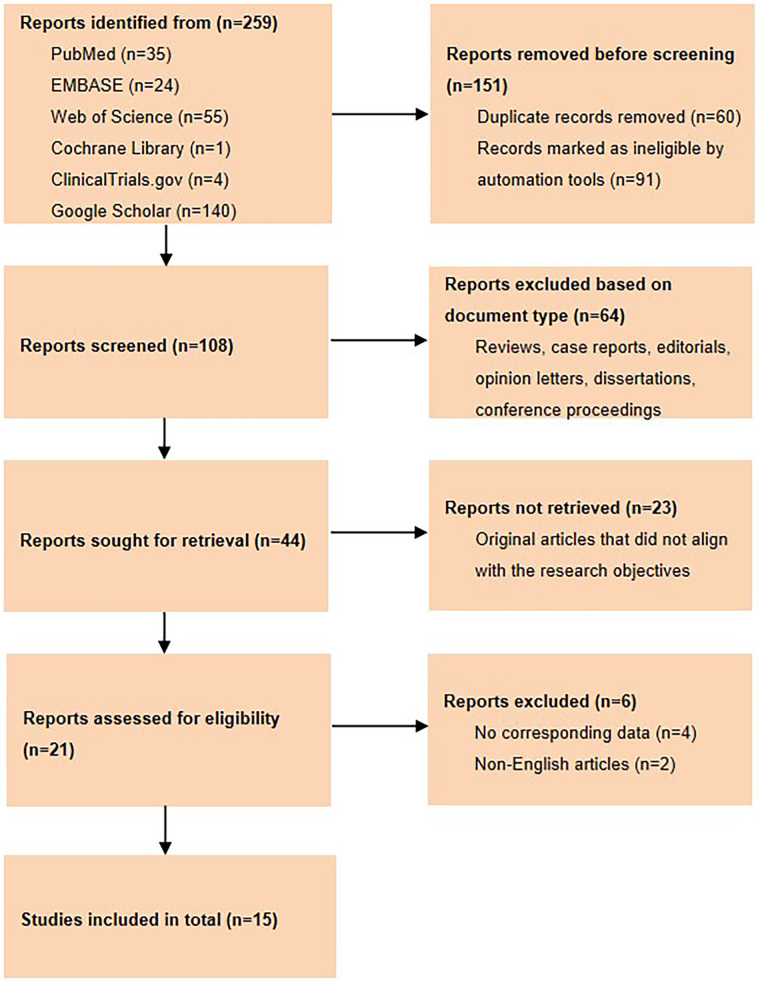 Figure 2
Figure 2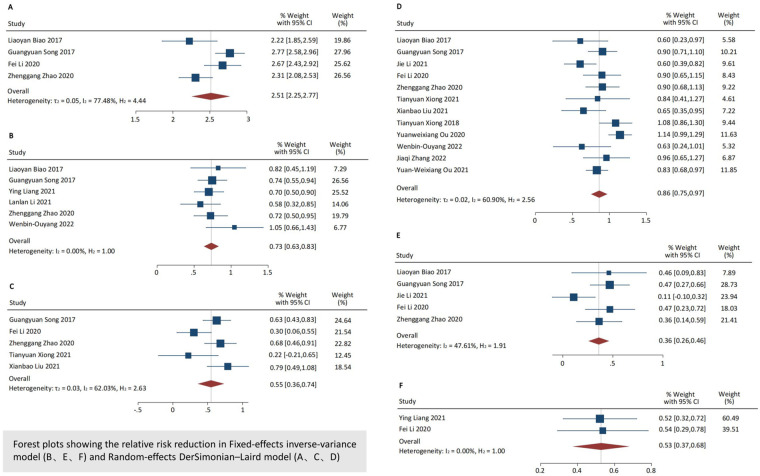 Figure 3
Figure 3| Study author | Year | Recruitment period | Follow-up time, months | Research patients | Patients who used Venus A | Average age, years | Gender, male | STS score, % | Study type |
|---|---|---|---|---|---|---|---|---|---|
| Liaoyan Biao | 2017 | 2012–2014 | 24 | 54 | 27 | 74.1 | 15 | 6.2 | Retrospective |
| Guangyuan Song | 2017 | 2012–2015 | 6 | 101 | 101 | 75.4 | 58 | 5.5 | Retrospective |
| Ying Liang | 2021 | 2012–2018 | 12 | 284 | 97 | TAVI: 76.6 | 175 | – | Retrospective |
| Jie Li | 2021 | 2016–2020 | 1 | 84 | 84 | Optimal position: 74.5 | 43 | – | Retrospective |
| Lanlan Li1 | 2021 | 2018–2019 | – | 53 | 53 | 68.1 | 42 | – | Retrospective |
| Fei Li | 2020 | 2014–2017 | 1 | 163 | 63 | 76.1 | 35 | 8.3 | Retrospective |
| Zhengang Zhao | 2020 | 2017–2018 | 1 | 75 | 75 | 73.8 | 44 | 7.4 | Retrospective |
| Tianyuan Xiong | 2021 | – | – | 20 | 20 | 72.5 | 11 | – | Retrospective |
| Xianbao Liu | 2021 | – | – | 43 | 43 | BAV: 76.4 | 26 | – | Retrospective |
| Tianyuan Xiong | 2018 | 2012–2017 | – | 80 | 56 | 75.0 | 47 | – | Retrospective |
| Abdullah Hagar | 2020 | 2012–2017 | – | 256 | 145 | 74 | 145 | – | Retrospective |
| Yuanweixiang OU | 2020 | 2015–2017 | – | 165 | 165 | 74 | – | – | Single-arm |
| Wenbin Ouyang | 2022 | 2020–2021 | 12 | 178 | 97 | BEV: 72.4 | 99 | – | Retrospective |
| Zhangjia Qi | 2022 | 2019–2021 | 1 | 39 | 39 | 75 | 21 | – | Retrospective |
| Yuanweixiang OU | 2021 | 2015–2019 | 1 | 181 | 181 | Without HAVB: 72.8 | 103 | – | Retrospective |
| Study author | Year | Patients | PPI | BBB | PVD | CABG | MI | PCI | Stroke | AF | CKD | CLD | Hypertension | Diabetes | CAD | NYHA Class III/IV | Postprocedural AVmax, m/s |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Liaoyan Biao | 2017 | 54 | – | – | – | – | 2 | – | 7 | 12 | 6 | – | – | 10 | 18 | 50 | CoreValve: 2.5 ± 0.5 |
| Guangyuan Song | 2017 | 101 | 5 | 13 | 32 | 2 | 5 | 9 | 15 | 15 | – | 40 | 50 | 17 | – | 80 | 2.2 (2.0–2.6) |
| Ying Liang | 2021 | 284 | – | 20 | 52 | – | 22 | 28 | 100 | 39 | – | 37 | 109 | 52 | – | 23 | – |
| Jie Li | 2021 | 84 | 1 | – | 14 | – | – | 14 | 7 | 18 | – | 5 | 41 | 18 | 35 | 50 | – |
| Lanlan Li | 2021 | 53 | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Fei Li | 2020 | 163 | – | – | – | 5 | – | – | 26 | 29 | – | – | 94 | 44 | 61 | 141 | SAPIEN:2.25 ± 0.37 |
| Zhengang Zhao | 2020 | 75 | – | – | 35 | – | – | – | – | 14 | – | 41 | 32 | 7 | 33 | 70 | – |
| Tianyuan Xiong | 2021 | 20 | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Xianbao Liu | 2021 | 43 | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Tianyuan Xiong | 2018 | 80 | 21 | – | 36 | – | 3 | – | – | 28 | 9 | 43 | 42 | 13 | 29 | 77 | PPI:2.5 (2.2–2.8) |
| Abdullah Hagar | 2020 | 256 | – | – | 143 | – | 5 | – | 34 | 37 | 36 | 162 | 114 | 46 | 110 | 234 | 2.44 ± 1.1 |
| Yuanweixiang OU | 2020 | 165 | 48 | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Wenbin Ouyang | 2022 | 178 | 5 | – | 36 | 8 | – | 38 | 29 | 19 | – | 15 | 98 | 40 | 56 | – | – |
| Zhangjia Qi | 2022 | 39 | – | – | 12 | – | – | – | 13 | 9 | – | 3 | – | 13 | 23 | 14 | – |
| Yuanweixiang OU | 2021 | 181 | – | – | 72 | – | – | – | – | – | – | 84 | 70 | 35 | 67 | 158 | – |
| Variable | Results of meta-analysis |
| Adjusted results | Results of the Egger test, |
|---|---|---|---|---|
| Procedure details and adverse events during hospitalization | ||||
| Device/procedure success | 2.51 (95% CI: 2.25–2.77) | 77.48% | 0.90 (95% CI: 0.81–0.96) | 0.207 |
| Pre-dilation | 2.52 (95% CI: 2.06–2.9) | 85.76% | 0.90 (95% CI: 0.73–0.99) | 0.117 |
| Post-dilation | 1.22 (95% CI: 0.79–1.66) | 83.81% | 0.28 (95% CI: 0.15–0.54) | 0.095 |
| Conversion to SAVR | 0.30 (95% CI: 0.11–0.50) | 44.77% | 0.02 (95% CI: 0.00–0.06) | 0.802 |
| Need a second valve | 0.73 (95% CI: 0.63–0.83) | 0.00% | 0.12 (95% CI: 0.06–0.19) | 0.221 |
| PVL ≥ moderate | 0.55 (95% CI: 0.36–0.74) | 62.03% | 0.07 (95% CI: 0.03–0.13) | 0.297 |
| Adverse events at the 30-day follow-up evaluation | ||||
| Major vascular complication | 0.40 (95% CI: 0.25–0.54) | 0.00% | 0.03 (95% CI: 0.01–0.07) | 0.740 |
| Major bleeding | 0.64 (95% CI: 0.49–0.80) | 0.00% | 0.09 (95% CI: 0.05–0.15) | 0.977 |
| Stroke | 0.16 (95% CI: 0.04–0.28) | 0.00% | 0.00 (95% CI: 0.00–0.02) | 0.784 |
| AKI | 0.36 (95% CI: 0.21–0.50) | 0.00% | 0.03 (95% CI: 0.01–0.06) | 0.658 |
| New-onset AF | 0.74 (95% CI: 0.50–0.98) | 42.11% | 0.13 (95% CI: 0.06–0.22) | 0.188 |
| New PPI | 0.86 (95% CI: 0.75–0.97) | 60.90% | 0.17 (95% CI: 0.13–0.21) | 0.182 |
| All-cause mortality | 0.36 (95% CI: 0.26–0.46) | 47.61% | 0.03 (95% CI: 0.01–0.05) | 0.631 |
| Adverse events at the 1-year follow-up evaluation | ||||
| All-cause mortality | 0.53 (95% CI: 0.37–0.68) | 0.00% | 0.07 (95% CI: 0.03–0.11) | 0.923 |
| Adverse events of BAV at the 30-day follow-up evaluation | ||||
| New PPI | 0.83 (95% CI: 0.62–1.04) | 0.00% | 0.16 (95% CI: 0.09–0.25) | 0.678 |
| All-cause mortality | 0.58 (95% CI: 0.33–0.83) | 0.00% | 0.08(95% CI: 0.03–0.16) | 0.811 |
| Variable | Results of meta-analysis |
| Results of the Egger test, |
|---|---|---|---|
| Baseline | |||
| PGmean, mmHg | 58.52 (95% CI: 47.24–69.79) | 90.42% | 0.005 |
| Vmax, m/s | 4.86 (95% CI: 4.72–5.00) | 0.00% | 0.645 |
| LVEF, % | 56.88 (95% CI: 54.33–59.44) | 11.79% | 0.183 |
| During hospitalization | |||
| PGmean, mmHg | 10.85 (95% CI: 9.54–12.17) | 0.00% | 0.960 |
| Vmax, m/s | 2.23 (95% CI: 2.04–2.44) | 69.69% | 0.827 |
| LVEF, % | 58.76 (95% CI: 56.34–61.17) | 0.00% | 0.776 |
| At the 30-day follow-up evaluation | |||
| PGmean, mmHg | |||
| Vmax, m/s | 2.25 (95% CI: 2.15–2.35) | 0.00% | 0.365 |
| LVEF, % | 59.93 (95% CI: 57.72–62.13) | 15.60% | 0.276 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Congenital Heart Disease Studies · Aortic Disease and Treatment Approaches
Introduction
Background
Since the introduction of transcatheter aortic valve replacement (TAVR) into global clinical practice over 20 years ago, a vast portfolio of high-quality clinical data has confirmed the efficacy and safety of TAVR across the entire surgical risk spectrum (1–3). Although TAVR development has been relatively recent in China, a rapid and comprehensive development phase began in 2017 with the approval of two domestic valves (2). The Venus A valve (Venus Medtech, Hangzhou, China) is a first-generation domestic self-expanding valve (SEV) approved by the China Food and Drug Administration. By 2015, the TAVR clinical trial involving the Venus A valve was completed in China (ClinicalTrials.gov identifier: NCT01683474), and investigators demonstrated promising results in the treatment of patients with bicuspid or tricuspid aortic valve (TAV) stenosis who were deemed unsuitable for surgery (4). The TAVR clinical trial (4) assessed the clinical profile and outcomes of TAVR in patients with severe symptomatic aortic stenosis (AS). The preliminary results implied that treatment of AS with the Venus A valve is effective.
Rationale and knowledge gap
The Venus A valve is a self-expanding frame manufactured by suturing valve leaflets and a skirt made from a single layer of porcine pericardium into a tri-leaflet configuration (4). The first-generation SEV developed in the United States was the CoreValve transcatheter bioprosthesis (Medtronic, MN, USA) (5). The Venus A valve, like the CoreValve, has a supra-annular design with the functioning prosthetic leaflets located above the native annulus when properly deployed (4). However, the Venus A valve device differs from other valves in several respects. Specifically, there are three rounded paws rather than two at the outflow end for coaxial loading, radiopaque markers of 0.5 cells above the inflow end indicate the optimal landing zone, and the inflow end is tapered to protect the conduction tissue (Figure 1). To date, there has been limited data describing the procedural, clinical, and valve performance outcomes of the Venus A valve, the first-generation domestic SEV for TAVR in China.
Illustration of the Venus A valve.
Objective
The present meta-analysis analyzed and evaluated the efficacy and safety of the Venus A valve in Chinese patients. We present this article in accordance with the PRISMA reporting checklist.
Methods
Search strategy, study selection, and data extraction
A systematic search was performed to retrieve relevant literature from PubMed, Embase, Web of Science, the Cochrane Library, ClinicalTrials.gov, and Google Scholar from inception until 1 June 2022. Domestic libraries were not searched due to data overlap. The search code was as follows: (“Transcatheter Aortic Valve Implantation [TAVI]” OR “Transcatheter Aortic Valve Replacement [TAVR]” OR “Percutaneous Aortic Valve” OR “Transcatheter Aortic Valve”) AND “Venus A.”
In the present study, the following inclusion criteria were used: (1) All study types except case reports or reviews were considered for inclusion (e.g., cross-sectional studies and cohort studies); (2) patients undergoing TAVR with the Venus A valve were included in the study; and (3) the study reported the procedural, clinical, and valve performance results of the Venus A valve. The following studies were excluded: (1) duplicate studies; (2) studies containing other valves, the data of which could not be extracted separately; and (3) non-English language studies or no corresponding data. Two investigators (CL and DS) independently assessed the quality of articles and extracted relevant data. Any disagreements in quality assessment were resolved through consultation with a third investigator (JG).
Outcomes of interest
Efficacy outcome measures include the device/procedure success rate, the mean transvalvular gradient (PGmean), peak jet velocity (Vmax), and left ventricle ejection fraction (LVEF) at baseline, during hospitalization, and at the follow-up evaluation.
Safety outcomes of the Venus A valve included pre-dilation, post-dilation, conversion to surgical aortic valve replacement (SAVR), the need for a second valve, moderate or severe paravalvular leakage (PVL), and adverse events. Adverse events at the 30-day follow-up evaluation included life-threatening or disabling bleeding, major vascular complications, new permanent pacemaker implantation (PPI), acute kidney injury (AKI), new-onset atrial fibrillation (AF), stroke, and all-cause mortality. In addition, adverse events at the 1-year follow-up evaluation included all-cause mortality. Furthermore, the safety of the Venus A valve for a bicuspid aortic valve (BAV) was preliminarily examined.
The Valve Academic Research Consortium 3 (VARC-3) was used to define TAVR-specific outcomes (6), while study-specific definitions remained in the corresponding articles. The success of the device/procedure was defined as the absence of surgical mortality, accurate placement of a singular artificial valve in the appropriate anatomic position, and achieving the anticipated effect. Type 3 (life-threatening) bleeding was defined as overt bleeding occurring in a critical organ, causing hypovolemic shock or severe hypotension, or necessitating reoperation, surgical exploration, or re-intervention to achieve hemostasis. Type 4 (leading to death) bleeding was defined as any overt bleeding event that directly resulted in mortality. Major vascular complications are defined as the occurrence of aortic dissection/rupture, vascular injury, distal embolization, unplanned endovascular/surgical intervention, or closure device failure, provided that any of these events result in death, VARC type ≥2 bleeding, limb/visceral ischemia, irreversible neurologic impairment, amputation, or irreversible end-organ damage.
Quality of assessment
The Newcastle–Ottawa scale (NOS) was used to evaluate the included retrospective studies (7). The methodological index for non-randomized studies (MINORS) was used to assess the included non-randomized study (single-arm study) (8).
Statistical analysis
The single-arm meta-analysis was conducted using Stata statistical software (version 17.0). The original data from the literature were transformed using the double arcsine method to conform to the normal distribution before analysis using Stata. The initial meta-analysis conclusion was then restored using the following formula to make a final conclusion: P = [sin (tp/2)]^2^. The I^2^ value was used to assess heterogeneity. The random-effects model was used to calculate the combined proportion and 95% confidence interval (CI) when I^2^ was >50%; otherwise, a fixed-effect model was used. Publication bias was assessed using the Egger test, with P < 0.05 indicating potential bias.
Results
Search results
A comprehensive search yielded a total of 259 articles, of which 151 were excluded due to duplication or automation exclusion. Additionally, 64 articles did not meet the specified inclusion criteria, 23 articles had inconsistent objectives, and 6 articles had no corresponding data or were non-English language articles and were excluded. Therefore, a total of 15 articles were deemed suitable for inclusion in the present meta-analysis, encompassing data from 1,144 Chinese patients. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram depicts the study flow (Figure 2).
Flow chart of the study selection process.
Pooled results of procedure details and adverse events within hospitalization and at follow up. Forest plots showing the relative risk reduction in Fixed-effects inverse-variance model (B, E, F) and Random-effects DerSimonian-Laird model (A, C, D); (A) device/procedure success during hospitalization, (B) need a second valve during hospitalization, (C) PVL ≥ moderate at 30-day follow-up evaluation, (D) new PPI at 30-day follow-up evaluation, (E) all-cause mortality at 30-day follow-up evaluation, (F) All-cause mortality at 1-year follow-up evaluation.
Details of all studies and quality assessment
All 15 eligible studies were conducted in China, including 14 retrospective studies and 1 single-arm study. Supplementary Table S1 presents the quality assessment results of the included studies. Supplementary Tables S2 and S3 present the echocardiographic characteristics and outcome indicators of the included studies, respectively. All retrospective studies had quality assessment scores ≥7. The MINORS index of the single-arm study was 10. Basic information from the studies is detailed in Table 1.
Baseline characteristics of patients
The baseline characteristics of patients are presented in part in Tables 1 and 2. The patients in the extractable data were nearly 70 years of age, and 61.2% were males. A 5%–10% score on the Society of Thoracic Surgeons (STS) risk calculator indicated intermediate risk. Overall, 75% of patients were in the New York Heart Association (NYHA) functional class ≥III. The overall patient disease spectrum is listed in Table 2.
Efficacy outcomes
The device/procedure success rate was 90% (95% CI: 0.81–0.96, I^2^ = 77.48%; Table 3). Three studies reported PGmean and Vmax improvement (4, 9, 10). The PGmean was 58.52 mmHg (95% CI: 47.24–69.79, I^2^ = 90.42%) and the Vmax was 4.86 m/s (95% CI: 4.72–5.00, I^2^ = 0.00%) prior to TAVR. The PGmean decreased to 10.85 mmHg (95% CI: 9.54–12.17, I^2^ = 0.00%) and the Vmax decreased to 2.23 m/s (95% CI: 2.04–2.44, I^2^ = 69.69%) during hospitalization (Table 4).
Safety outcomes
Eight studies have investigated the TAVR procedure details with the Venus A valve (4, 9–15). The incidence of pre- and post-dilation was 90% (95% CI: 0.73–0.99, I^2^ = 85.76%) and 28% (95% CI: 0.15–0.54, I^2^ = 83.81%), respectively. The conversion to SAVR rate was 2% (95% CI: 0.00–0.06, I^2^ = 44.77%), and the requirement for a second valve accounted for 12% of cases (95% CI: 0.06–0.19, I^2^ = 0.00%). During hospitalization, 7% of patients (95% CI: 0.03–0.13, I^2^ = 62.03%) had moderate or severe PVL (Table 3).
Fourteen studies reported adverse outcomes (Figure 3; Table 3) (4, 9, 10, 15–23). At the 30-day follow-up evaluation, 3% of the patients (95% CI: 0.01–0.07, I^2^ = 0.00%) had a major vascular complication, and 9% (95% CI: 0.05–0.15, I^2^ = 0.00%) had major bleeding. No strokes were reported (95% CI: 0.00–0.02, I^2^ = 0.00%). The incidence of AKI and new-onset AF was 3% (95% CI: 0.01–0.06, I^2^ = 0.00%) and 13% (95% CI: 0.06–0.22, I^2^ = 42.11%), respectively. The incidence of new PPI was 17% (95% CI: 0.13–0.21, I^2^ = 60.90%). The 30-day all-cause mortality rate was 3% (95% CI: 0.01–0.05, I^2^ = 47.61%). At the 1-year follow-up evaluation, the all-cause mortality rate increased to 7% (95% CI: 0.03–0.11, I^2^ = 0.00%).
Three studies reported adverse outcomes of the Venus A valve for BAV (4, 16, 18). The incidence of new PPI was 16% (95% CI: 0.09–0.25, I^2^ = 0.00%), and the all-cause mortality rate was 8% (95% CI: 0.03–0.16, I^2^ = 0.00%) at the 30-day follow-up evaluation (Table 3).
Publication bias
The present study used Egger's test to detect publication bias. There was no significant publication bias in the assessment indicators (P > 0.05; Tables 3, 4) except for the PGmean at baseline (P = 0.005).
Discussion
Key findings
The present study evaluated the efficacy and safety of the first-generation domestic SEV (the Venus A valve) that is used for TAVR in China. The device/procedure success rate of TAVR using the Venus A valve was relatively high. Patients experience significant PGmean and Vmax hemodynamic improvements. Importantly, using the Venus A valve for TAVR did not significantly increase the complication and adverse event rates.
Strengths and comparison with similar research
Previous studies reported that the 30-day follow-up evaluation major vascular complication, life-threatening or disabling bleeding, stroke, AKI, and new-onset AF rates with the CoreValve were 8.2%, 12.7%, 2.3%, 1.7%, and 12.9%, respectively (23–25). In the present study, the incidence of major vascular complications (3%), major bleeding (9%), stroke (0%), AKI (3%), and new-onset AF (13%) was basically consistent with previous studies at the 30-day follow-up evaluation (24, 25). These data revealed that the Venus A valve is a suitable choice for Chinese patients undergoing TAVR.
At the 30-day and 1-year follow-up evaluations, the all-cause mortality rates were 3% and 7%, respectively. Popma et al. (24) reported that the all-cause mortality rates at the 30-day and 1-year follow-up evaluations in patients with severe AS at extreme risk for surgery who received the CoreValve were 8.4% and 24.3%, respectively. In addition, Adams et al. (26) reported that the all-cause mortality rate at the 1-year follow-up evaluation in patients with severe AS who received the CoreValve at increased risk for surgery was 14.2%. The SURTAVI study (25), which used the CoreValve or Evolut R (Medtronic), demonstrated that the all-cause mortality rates at the 30-day and 1-year follow-up evaluations in patients with severe AS at intermediate risk for surgery were 2.8% and 8.1%, respectively. Therefore, the all-cause mortality rate at 30-day and 1-year follow-up in the present study was comparable to the SURTAVI study (25) but lower than the rates reported by Popma et al. (24) and Adams et al. (26). These promising results may be attributed to the near 50% prevalence of BAV in the Chinese population presenting for TAVR, which exceeds the 2%–10% overall prevalence reported in Western TAVR series (27). Patients with BAVs are younger on average than patients with TAVs (28). The potential impact of this finding is that patients referred for TAVR in China are much younger, with a mean age of 74 years. Nevertheless, the mean age of patients in European and US TAVR registries is >80 years (29). Therefore, from a safety perspective, TAVR using the Venus A valve may demonstrate equal safety to the CoreValve.
In the present study, the incidence of moderate or severe PVL during hospitalization was 7%, which was less than reported by Popma et al. (24) (10.7%). Balloon pre-dilation is a routine procedure; whether or not post-dilation is performed depends on valve performance and paravalvular regurgitation. Pre- and post-dilation facilitates delivery of the transcatheter valve and expansion of the nitinol prosthesis frame to achieve the desired hemodynamics and minimize PVL (30). The incidence of pre- and post-dilation in the current study was 90% and 28%, respectively, which are comparable to the Popma et al. (24) results. The post-dilation rate was nearly the same as the CoreValve but a lower PVL rate than the CoreValve occurred, which demonstrates that the Venus A valve exhibits comparable efficacy to the CoreValve. However, a head-to-head comparison is warranted to confirm this speculation.
The need for a second valve accounted for 12% of all cases, which was higher than reported by Popma et al. (24) (3.5%) and the Italian CoreValve Registry (3.6%) (31). The increased requirement for a second valve could be due to the following reasons: (1) TAVR was introduced relatively late in China, and the TAVR procedure requires extensive learning that was obtained from the experiences reported by other countries (32), and most cases occurred between 2012 and 2018, indicating that early TAVR procedures in China were performed with limited experience. Nevertheless, there has been a downward trend in the incidence of requiring a second valve (10, 33). (2) The relatively higher incidence of BAV was an influencing factor because prosthetic valve function could theoretically be jeopardized by pre-existing abnormal cusp fusion, heavily calcified leaflets, and an asymmetric BAV raphe (34). A higher valve-in-valve (VIV) bailout procedure was reported in the BAV cohort compared with the TAV group by De Biase et al. (35) (11% vs. 3%). 3) There were no retrievable or repositionable functions on the first-generation valves. Therefore, the valve expansion accuracy in the early phase was lower than that of the current valve prosthesis implantations. A meta-analysis revealed that the Medtronic second-generation Evolut R valve had a lower incidence of incorrect prosthetic positioning or unintended prosthetic performances than the CoreValve (3.5% vs. 5.2%) (36). It should be noted that despite the increased frequency of the VIV procedure, the clinical and echocardiographic endpoints compared favorably to those of patients undergoing the standard procedure (31).
Compared with surgery, TAVR with a self-expanding supra-annular bioprosthesis is associated with a lower incidence of disabling stroke, AKI, bleeding events, and new-onset AF, but a higher incidence of aortic regurgitation and permanent pacemaker use (37). The incidence of new PPI was 17%, which was lower than reported by Popma et al. (24) (21.6%) and the SURTAVI study (25.9%) (25), but comparable to Adams et al. (26) (19.8%) and Popma et al. (37) (17.4%). Conduction abnormalities are common after TAVR and may result in PPI (38), which is a main complication of TAVR that includes adverse effects involving left ventricular function, heart failure, and late mortality among low-risk patients with a potential for increased longevity (39). The anatomic proximity of the atrioventricular conduction system to the aortic valvular complex contributes to cardiac conduction disturbances (38). Conduction disturbances can develop due to direct physical damage or compression, such as injuries from wire manipulation or balloon aortic valvuloplasty, or compression by the valve frame, which causes ischemic damage to the conduction system cells or interstitial edema (40, 41). The shape and height of the frame may be key factors underlying this abnormality (42). We attribute this finding to the tapered design (Figure 1) at the inflow end to protect conduction tissue. Therefore, the incidence of new PPI was lower for the Venus A valve than in previous studies.
Previous guidelines and an expert consensus have identified BAV as a relative contraindication to TAVR (32). The present study generated a few preliminary results because the number of studies that have focused on BAV is limited, and few data could be extracted. Himbert et al. (43) showed that the 30-day combined safety endpoint rate in high-risk patients with stenotic BAV using the CoreValve was 93% with a PPI required in 40% of the patients. Because of the small sample size, the previous research only indicated that the Venus A valve is feasible for BAV, and the new PPI and all-cause mortality rates were not discussed in detail. Therefore, the safety and effectiveness of BAV should be investigated with a large sample size in a randomized controlled trial.
Study limitations
The present study had several limitations. First, high heterogeneity existed in more than one-half of the outcomes. However, the complete data were rarely accessed for subgroup analysis to reduce heterogeneity. Second, there may have been differences in postoperative efficacy between the Venus A valve and the CoreValve due to the different application times and the main adaptation population. Moreover, because single-arm trials lack control groups, comparisons between the Venus A valve and the CoreValve were based on data from the population with a discrepant baseline. Therefore, it is essential to design a prospective study to explore the clinical effects of the two types of valves. Third, BAV vs. TAV could not be analyzed due to the lack of original data. Therefore, outcomes for BAV intervention were preliminary findings awaiting further verification. Finally, due to the short-term follow-up of the included studies, the long-term prognosis of the Venus A valve has not been established. Future evaluation of the long-term prognosis of this valve will be beneficial for further improving valve equipment and enhancing implantation techniques.
Conclusions
In conclusion, this single-arm meta-analysis demonstrated that the Venus A valve is feasible for Chinese patients undergoing TAVR despite its relatively high requirement for a second valve. Moreover, preliminary findings indicated that TAVR with the Venus A valve may be suitable for Chinese patients with BAV.
Implications and actions needed
The Venus A valve effectiveness was demonstrated by the high device/procedure success rate and immediate hemodynamic improvement. The low incidence of complications confirmed the safety of the Venus A valve. Venus A valve may be worth promoting in the application of Chinese patients. However, it is essential to design a prospective study to explore the clinical effects of two or more types of valves with subgroup analysis. Future evaluation of the long-term prognosis of this valve will be beneficial for further improving valve equipment and enhancing implantation techniques.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Han Y. Current clinical data and experience of TAVR in China. Eur Heart J. (2022) 43(22):2087–8. 10.1093/eurheartj/ehab 82134977927 · doi ↗ · pubmed ↗
- 2Ge J-B. Chinese Expert consensus on transcatheter aortic valve replacement (2020 update). Cardiology Plus. (2020) 5(2):71–80. (2020). 10.4103/cp.cp_11_20 · doi ↗
- 3Tarantini G Dvir D Tang GHL. Transcatheter aortic valve implantation in degenerated surgical aortic valves. Euro Intervention. (2021) 17(9):709–19. 10.4244/EIJ-D-21-0015734665140 PMC 9725043 · doi ↗ · pubmed ↗
- 4Liao YB Zhao ZG Wei X Xu YN Zuo ZL Li YJ Transcatheter aortic valve implantation with the self-expandable Venus A-valve and Core Valve devices: preliminary experiences in China. Catheter Cardiovasc Interv. (2017) 89(S 1):528–33. 10.1002/ccd.2691228318133 · doi ↗ · pubmed ↗
- 5Forrest JK Kaple RK Tang GHL Yakubov SJ Nazif TM Williams MR Three generations of self-expanding transcatheter aortic valves: a report from the STS/ACC TVT registry. JACC Cardiovasc Interv. (2020) 13(2):170–9. 10.1016/j.jcin.2019.08.03531973793 · doi ↗ · pubmed ↗
- 6Généreux P Piazza N Alu MC Nazif T Hahn RT Pibarot P Valve academic research consortium 3: updated endpoint definitions for aortic valve clinical research. J Am Coll Cardiol. (2021) 77(21):2717–46. 10.1016/j.jacc.2021.02.03833888385 · doi ↗ · pubmed ↗
- 7Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25(9):603–5. 10.1007/s 10654-010-9491-z 20652370 · doi ↗ · pubmed ↗
- 8Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. (2003) 73(9):712–6. 10.1046/j.1445-2197.2003.02748.x 12956787 · doi ↗ · pubmed ↗