Evaluation of the predictive value of scoring systems in diagnosis of acute appendicitis: a comparative prospective study
Ayman Shemes, Amr A. Elgharib, Ahmed Elghrieb, Mohamed Shetiwy, Mahmoud A. Aziz, Shady Elzeftawy

TL;DR
This study compares different scoring systems for diagnosing acute appendicitis and finds that the Adult Appendicitis Score (AAS) performs best.
Contribution
The study evaluates and compares the diagnostic accuracy of four scoring systems for acute appendicitis in a prospective clinical setting.
Findings
The AAS score showed the highest diagnostic accuracy with an AUC of 0.988.
AAS and AIR scores had high sensitivity and overall accuracy compared to other systems.
Alvarado score had lower accuracy with an AUC of 0.715.
Abstract
Acute Appendicitis stands as the leading cause of acute abdominal pain necessitating surgical intervention in the world. The initial clinical assessment of patients suspected of having acute appendicitis remains crucial. The aim is to quickly confirm or rule out the diagnosis to minimize delays, avoid unnecessary surgeries. The aim of our study is to evaluate the predictive value of multiple scoring systems for Diagnosis of acute appendicitis cases with correlation between scores prediction results and surgical interventions results. This a prospective study carried out in Mansoura university hospitals and Mansoura emergency hospital in the period between December 2024 and June 2025. Patients included in the study were admitted at emergency department of General Surgery at Mansoura University Hospital. The study was explained in details to the whole patients sharing in the study and a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
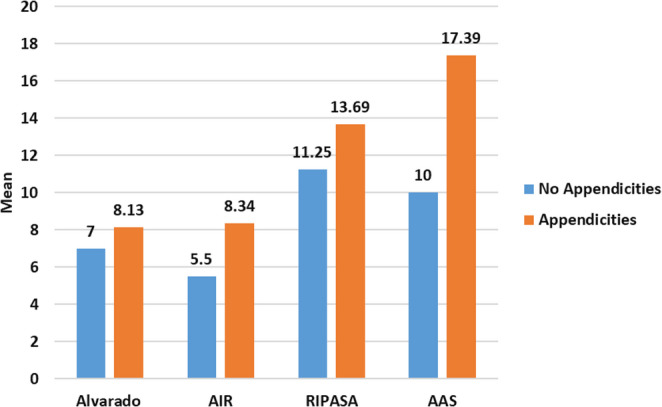 Figure 1
Figure 1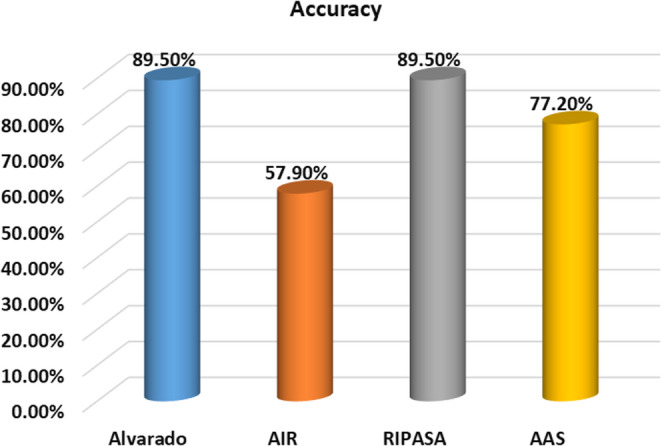 Figure 2
Figure 2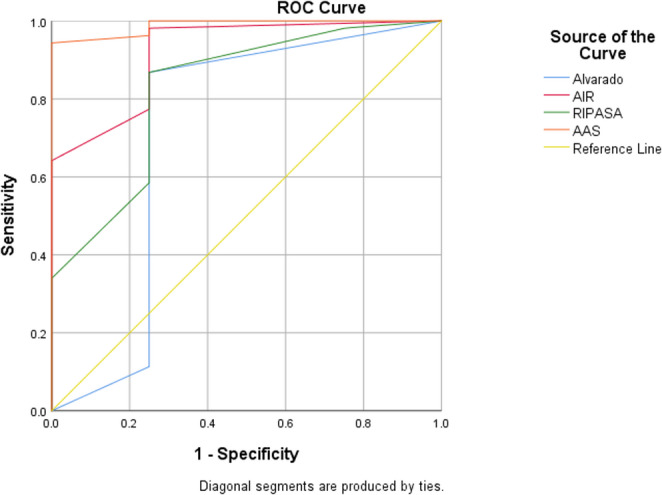 Figure 3
Figure 3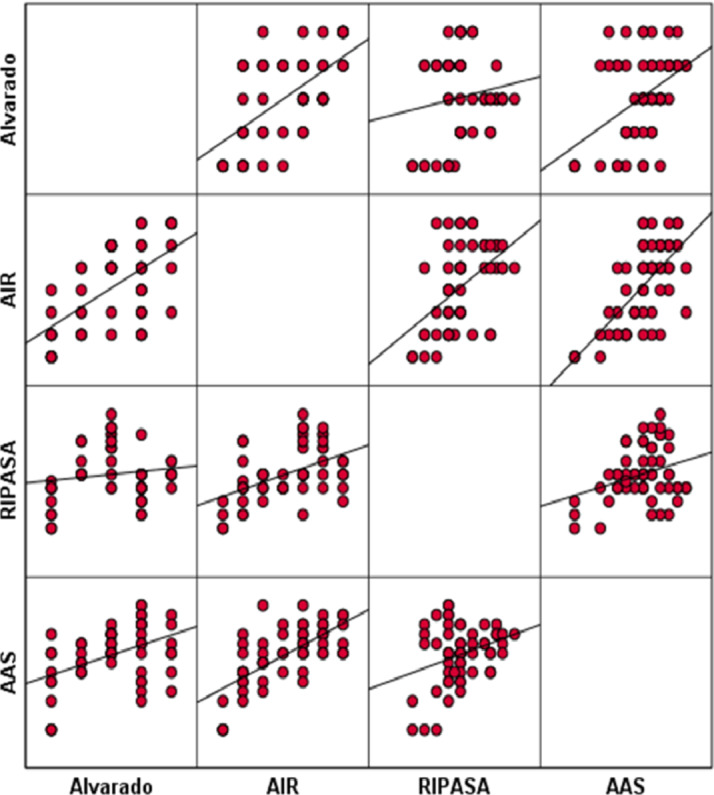 Figure 4
Figure 4- —Mansoura University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Sepsis Diagnosis and Treatment · Cardiac, Anesthesia and Surgical Outcomes
Introduction
Acute Appendicitis stands as the leading cause of acute abdominal pain necessitating surgical intervention in the world [1]. The initial clinical assessment of patients suspected of having acute appendicitis remains crucial. The aim is to quickly confirm or rule out the diagnosis to minimize delays, avoid unnecessary surgeries (where the appendix is found to be normal), prevent appendiceal perforation, and reduce hospital costs [2]. Both confirming and excluding the diagnosis of Acute appendicitis are important for better and cost-effective management. Physical or laboratory findings can’t be used alone to predict or exclude a diagnosis of AA [3]. There are various clinical scoring systems combining physical findings and/or laboratory data have been adopted in regard to this issue such as the Alvarado score, Appendicitis Inflammatory Response score (AIR), The RIPASA (Raja Isteri Pengiran Anak Saleha Appendicitis) score and AAS (Adult Appendicitis Score) [4, 5].
Aim of the work
The aim of our study is to evaluate the predictive value of multiple scoring systems for Diagnosis of acute appendicitis cases with correlation between scores prediction results and surgical interventions results.
Patients and methods
This a prospective study carried out in Mansoura university hospitals and Mansoura emergency hospital in the period between December 2024 and June 2025. Patients included in the study were admitted at emergency department of General Surgery at Mansoura University Hospital. The study was explained in details to the whole patients sharing in the study and a written informed consent was taken from all the patients.
Sample size
Sample size calculation was based on Diagnostic Efficacy of different scores in differentang acute appendicities cases. Depending on sensitivity 89%, precision 0.10 and confidence level 95%, expected revalence of 66% then total sample size will be 57.
All patient presented with suspected acute appendicitis were subjected to four scores with comparing between them:
- Alvarado score.
- Appendicitis Inflammatory Response score (AIR).
- The RIPASA (Raja Isteri Pengiran Anak Saleha Appendicitis) score.
- AAS (Adult Appendicitis Score).
Inclusion criteria
- 1 – Patient age > 16 years with acute appendicitis
- 2 – All patients accepted to participate in the study.
Exclusion criteria
- 1- Patients whose age less than 16 years old.
- 2- patients presented with septic shock.
- 3- Patients who had a pre-operative abdominal CT scan for the diagnosis.
Gold-standard for diagnosing or excluding the condition
Histopathological examination of the surgical biopsy specimen of the appendix was used a gold-standard reference for either confirming or excluding acute appendicitis. (Table 1, 2, 3 and 4).Table 1. Alvarado score [6]CriteriaRangeInterpretation- Migratory right iliac fossa pain (1)- Anorexia (1)- Nausea and vomiting (1)- Right iliac fossa tenderness (2)- Rebound tenderness (1)- Elevated temperature (1)- Leukocytosis (2)- Shift to the left of neutrophils (1) 0–10 0–4: Low probability of appendicitis5–6: Possible appendicitis7–8: Probable Appendicitis9–10: Very probable appendicitisTable 2AIR score [7]CriteriaRangeInterpretation- Vomiting (1)- Right lower quadrant pain (1)- Rebound tenderness(light = 1, medium = 2,strong = 3)- Fever (1)- Polymorphonuclearleukocytes (< 70% = 0, 70-84% = 1, ≥ 85% = 2)- White blood cellcount (< 10 × 109/L = 0, 10-14.9 × 109/L = 1,≥ 15 × 109/L = 2)-Serum C-reactiveprotein (< 10 mg/dL = 0,10–49 mg/dL = 1, > 50mg/dL = 2) 0–12 0–4: Low probability ofappendicitis.5–8: Moderate probability9–12: High probabilityTable 3RIPASA score [8]CriteriaRangeInterpretation- Male (1)- Age < 40 years (1)- Migratory right iliac fossa pain (0.5)- Anorexia (1)- Nausea and vomiting (1)- Right iliac fossa pain (1)- Right iliac fossa tenderness (1)- Rebound tenderness (1)- Guarding (2)- Rovsing’s sign (2)- Fever (1)- Raised white blood cell count (1)- Negative urinalysis (1) 0–16.5.5 < 5: Low probability ofAppendicitis5–7: Low intermediate probability7.5–11.5: high intermedite probability> 12: High probability ofAppendicitisTable 4AAS score [9]AAS score CriteriaScoreInterpretation- Pain in RLQ (2) Adult Appendicitis Score (AAS): score ⩽10 low risk of appendicitis, score 11–15 intermediate risk of appendicitis,* and score* ⩾16 high risk of appendicitis
- Pain relocation (2)- RLQ tendernessWomen aged 16–49 years (1)All other patients (3)GuardingMild (2)Moderate or severe (4)- Blood leukocyte count (×109)⩾7.2 and < 10.9 (1)⩾10.9 and < 14.0 (2)⩾14.0 (3)- Proportion of neutrophils (%)⩾62 and < 75 (2)⩾75 and < 83 (3)⩾83 (4)CRP (mg/L), symptoms < 24 h⩾4 and < 11 (2)⩾11 and < 25 (3)⩾25 and < 83 (5)⩾83 (1)CRP (mg/L), symptoms > 24 h⩾12 and < 53 (2)⩾53 and < 152 (2)⩾152 (1)
Method
All the patients were subjected to full detailed history taking and proper general and local examinations.
- Abdominal ultrasound will be done to all patients before admission.
- Laboratory investigations (Complete blood Picture (CBC), C-Reactive protein, INR, urine analysis, Liver and kidney function test) will be done before admission.
- Pregnancy test in female cases presented with suspected acute appendicitis was done.
- Patient age and sex were recorded for all participants and incorporated into score calculation where applicable (e.g., RIPASA and AAS). As demographic variables were not evaluated as independent outcome predictors, a separate demographic summary table was not included.
All patient presented with suspected acute appendicitis were subjected to four scores with comparing between them:
- Alvarado score.
- Appendicitis Inflammatory Response score (AIR).
- The RIPASA (Raja Isteri Pengiran Anak Saleha Appendicitis) score.
- AAS (Adult Appendicitis Score).
The Alvarado, Appendicitis Inflammatory Response (AIR), RIPASA, and Adult Appendicitis Score (AAS) were selected for evaluation due to their widespread clinical use, ease of bedside application, and reliance on routinely available clinical and laboratory parameters.
Statistical analysis and data interpretation
Data analysis was performed by SPSS software, version 26 (SPSS Inc., PASW statistics for windows version 26. Chicago: SPSS Inc.). Quantitative data were described using mean ± Standard deviation for normally distributed data after testing normality using Kolmogrov-Smirnov test. Significance of the obtained results was judged at the (0.05) level.
- McNemar test & Marginal Homogenity test (Stewart Maxwell) was used to Student t test was used to compare 2 independent groups for normally distributed data.
- The Spearman’s rank-order correlation is used to determine the strength and direction of a linear relationship between two non-normally distributed continuous variables and/or ordinal variables.
- Receiver operating characteristics curve (ROC curve) was used to calculate validity (sensitivity & specificity) of continuous variables with calculation of best cut off point.Predictive values and accuracy are assessed using cross tabulation.
Results
In this study, four clinical scoring systems: Alvarado, AIR, RIPASA, and AAS, were evaluated for their diagnostic accuracy in cases of suspected acute appendicitis. Receiver operating characteristic (ROC) curve analysis demonstrated significant differences in the diagnostic performance of the evaluated scoring systems for acute appendicitis. The Appendicitis Assessment Score (AAS) showed the highest discriminatory ability with an area under the curve (AUC) of 0.988 (95% CI: 0.961–1.0, p = 0.001), followed by the Appendicitis Inflammatory Response (AIR) score (AUC = 0.920, 95% CI: 0.790–1.0, p = 0.005) and the RIPASA score (AUC = 0.825, 95% CI: 0.605–1.0, p = 0.03). The Alvarado score demonstrated lower diagnostic performance (AUC = 0.715, 95% CI: 0.337–1.0, p = 0.155). At the optimal cutoff values (≥ 14 for AAS, ≥ 6 for AIR, ≥ 12 for RIPASA, and ≥ 7 for Alvarado), AAS achieved a sensitivity of 94.3% and a specificity of 100%, while AIR demonstrated the highest sensitivity (98.1%) with a specificity of 75.0%. Both RIPASA and Alvarado scores showed sensitivities of 86.8% and specificities of 75.0%. Positive predictive values were high across all scoring systems (97.9–100%), whereas negative predictive values ranged from 30.0% to 75.0%. Overall diagnostic accuracy was highest for AIR (96.5%) and AAS (94.7%), confirming their superior performance compared with RIPASA (94.7%) and Alvarado (85.9%) in the studied cohort.
In details, Table (5) and Fig. (1) present a comparative analysis of mean scores for the Alvarado, AIR, RIPASA, and AAS systems among patients with and without confirmed diagnosis of acute appendicitis. The data show that mean scores were consistently higher in patients with appendicitis across all scoring systems, with AIR, RIPASA, and AAS demonstrating statistically significant differences (p = 0.002, p = 0.017, and p = 0.001, respectively), indicating their superior discriminatory ability. Alvarado showed a non-significant trend toward higher scores in appendicitis cases (p = 0.09).Table 5. Comparison of different studied scores in determining cases with acute appendicitis in the present studyAppendicitisp value-VE(N = 4)+VE(N = 53)Alvarado7 ± 28.13 ± 1.21t = 1.72p = 0.09AIR5.50 ± 1.08.34 ± 1.74t = 3.20p = 0.002RIPASA11.25 ± 1.7113.69 ± 1.92t = 2.47p* = 0.017AAS10 ± 2.017.39 ± 2.44t = 5.91p* = 0.001*t = Student t test, *statistically significant, data expressed as mean ± SDFig. 1Comparison of different studied scores in determining cases with acute appendicitis in the present study
Table (6) and Fig. (2) illustrate the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of each scoring system according to reference cutoff values from published literature. All scoring systems demonstrated perfect specificity and PPV (100%), reflecting a strong ability to correctly identify true cases when positive. However, this inflated specificity can be attributed to the limited sample size which presents a major limitation that prevents definitive conclusions. Sensitivity varied, with Alvarado and RIPASA showing higher sensitivity (88.7%) compared to AAS (75.5%) and AIR (54.7%). However, all systems showed low NPV, indicating limited reliability in ruling out appendicitis when scores are low. These findings emphasize that while the studied scores effectively confirm the diagnosis of appendicitis, they are less reliable to exclude the diagnosis.Table 6. Comparison of studied scores according to reference values published in differentiating cases with acute appendicitis [10–12]SensitivitySpecificityPPVNPVAccuracyAlvarado88.7%100%100%40%89.5%AIR54.7%100%100%14.3%57.9%RIPASA88.7%100%100%40%89.5%AAS75.5%100%100%23.5%77.2%PPV: Positive predictive value NPV: Negative predictive valueFig. 2Comparison of studied scores according to reference values published in differentiating cases with acute appendicitis [10–12]
Table (7) and Fig. (3) display the ROC curve analysis results of the current study, showing the area under the curve (AUC), optimal cutoff points, sensitivity, specificity, PPV, NPV, and accuracy for each scoring system in diagnosing acute appendicitis. The AAS demonstrated the highest AUC (0.988, p = 0.001), indicating excellent diagnostic performance, followed by AIR (AUC = 0.920, p = 0.005) and RIPASA (AUC = 0.825, p = 0.03). Alvarado exhibited a lower AUC (0.715, p = 0.155), suggesting comparatively lower discriminatory power. These findings confirm that AAS and AIR scores provide superior diagnostic accuracy and reliability in identifying cases of acute appendicitis, with AAS particularly excelling in clinical performance.Table 7ROC curve of studied scores in differentiating cases with appendicitis in the present studyAUC(95%CI)P valueCut off pointSensitivitySpecificityPPVNPVAccuracyAlvarado0.715(0.337–1.0.337.0)0.155≥ 786.8%75.0%97.9%30%85.9%AIR0.920(0.790–1.0.790.0)0.005*≥ 698.1%75.0%98.1%75.0%96.5%RIPASA0.825(0.605–1.0.605.0)0.03*≥ 1286.8%75.0%97.9%30.0%94.7%AAS0.988(0.961–1.0.961.0)0.001*≥ 1494.3%100.0%100.0%57.1%94.7%PPV: Positive predictive value NPV: Negative predictive valueFig. 3ROC curve of studied scores in differentiating cases with appendicitis in the present study
Table (8) and Fig. (4) show the correlation matrix and scatter plots illustrating the relationships between the different scoring systems in diagnosing appendicitis. Significant positive correlations were observed, particularly between AAS and AIR (r = 0.683, p < 0.05), indicating a strong association in their scoring patterns among cases studied. Alvarado showed moderate correlations with AIR (r = 0.605, p < 0.05) and AAS (r = 0.441, p < 0.05), while RIPASA demonstrated lower but still significant correlations with AIR (r = 0.488, p < 0.05) and AAS (r = 0.309, p < 0.05). These correlations support the concurrent validity of these scoring systems and suggest that while the scores align in trends, AAS and AIR may provide complementary value in the clinical assessment of suspected appendicitis. While most scoring systems demonstrated significant positive correlations, particularly between AAS and AIR. RIPASA showed a weak and non-significant correlation with Alvarado, indicating partial rather than complete alignment among the evaluated scores. Table 8. Correlation matrix between different scores for differentiating appendicitisAlvaradoAIRRIPASAAASAlvarado1AIR0.6051RIPASA0.1450.4881AAS0.4410.6830.309*1.0Data assessed by correlation coefficient, *statistically significantFig. 4Scatter diagram showing correlation between different scores for differentiating appendicitis
Discussion
Acute appendicitis (AA), the inflammation of the appendix, remains one of the most common causes of acute abdominal pain presenting to emergency departments (EDs), with a lifetime incidence of approximately 7% in the general population [13]. Despite its frequency, the diagnosis of AA continues to pose a clinical challenge due to atypical presentations, particularly among young adults, elderly patients, and females. Gynecological and urogenital conditions may mimic appendicitis, leading to diagnostic uncertainty and potential delays in management [14]. To improve diagnostic accuracy and reduce negative appendectomy rates, several clinical scoring systems have been developed. Among these, the Alvarado score- based on clinical symptoms, physical findings, and laboratory parameters- has been the most widely used. However, previous studies have demonstrated reduced diagnostic accuracy of the Alvarado score, particularly in Eastern populations [15]. The Acute Inflammatory Response (AIR) score was introduced to enhance diagnostic discrimination by incorporating C-reactive protein (CRP) and detailed inflammatory markers alongside clinical criteria [16]. More recently, the Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score was developed, integrating 14 clinical and laboratory parameters, and has been shown to outperform the Alvarado score in several Asian populations with different ethnic and dietary characteristics [17]. In addition, the Adult Appendicitis Score (AAS) has emerged as a comprehensive scoring system designed to improve risk stratification and clinical decision-making. Accordingly, the present study aimed to evaluate and compare the diagnostic performance of multiple appendicitis scoring systems and to assess the correlation between score predictions and surgical outcomes.
The study included 57 patients presenting with suspected acute appendicitis to the Emergency Department of General Surgery at Mansoura University Hospital. Histopathological examination confirmed acute appendicitis in 53 patients, while 4 cases were normal, yielding a negative appendectomy rate of 7%. Comparative analysis revealed that mean scores for all evaluated systems were higher in patients with confirmed appendicitis. Statistically significant differences were observed for AIR, RIPASA, and AAS scores (p = 0.002, p = 0.017, and p = 0.001, respectively), highlighting their superior discriminatory ability, whereas the Alvarado score demonstrated only a non-significant trend (p = 0.09). The diagnostic performance of the scoring systems in the present study was variable rather than uniformly perfect. At the optimal cutoff points derived from ROC analysis, AIR demonstrated the highest sensitivity (98.1%) with a specificity of 75.0%, while AAS showed high sensitivity (94.3%) and an apparent specificity of 100%. RIPASA and Alvarado demonstrated moderate sensitivity (86.8% for both) and specificity (75.0% for both). Positive predictive values were high across all scoring systems, reflecting the high prevalence of appendicitis in the study cohort; however, negative predictive values were relatively low, particularly for Alvarado and RIPASA scores, indicating limited reliability in excluding appendicitis when scores were below the cutoff. These findings suggest that while these scoring systems are useful for confirming the diagnosis of AA, caution is warranted when using them to rule out the disease. ROC curve analysis further supported these findings, with AAS demonstrating the highest area under the curve (AUC = 0.988, p = 0.001), indicating excellent diagnostic performance. This was followed by the AIR score (AUC = 0.920, p = 0.005) and RIPASA score (AUC = 0.825, p = 0.03), while the Alvarado score exhibited lower discriminatory ability (AUC = 0.715, p = 0.155). These results confirm that AAS and AIR provide superior diagnostic accuracy compared with Alvarado and RIPASA in the present cohort. In agreement with the current findings, Shuaib et al. (2017) reported superior sensitivity and specificity of the RIPASA score compared with the modified Alvarado score, along with better negative predictive value and diagnostic accuracy [18]. Similarly, Chong et al. (2010) documented sensitivity and specificity values of 88% and 67%, respectively, for RIPASA in an Asian population, with a negative appendectomy rate of 22.9% [19]. Nanjundaiah et al. (2014) also demonstrated higher sensitivity for RIPASA compared with Alvarado, although specificity varied between studies [20]. Conversely, Ak et al. (2020) reported higher diagnostic accuracy for RIPASA compared with AIR and Alvarado scores, with AIR demonstrating the highest sensitivity but lower specificity [14], highlighting the influence of population characteristics and study design on scoring system performance. Correlation analysis in the present study demonstrated significant positive relationships among the evaluated scoring systems, particularly between AAS and AIR (r = 0.683, p < 0.05), indicating strong concordance in their assessment patterns. Moderate correlations were observed between Alvarado and both AIR and AAS, while RIPASA showed weaker but statistically significant correlations. These findings support the concurrent validity of the scoring systems and suggest that AAS and AIR may offer complementary diagnostic value in clinical practice. Importantly, the apparent 100% specificity observed for AAS in the present study should be interpreted with caution. This finding is most likely attributable to the limited sample size and the small number of non-appendicitis cases, which may have resulted in an overestimation of specificity. Consequently, while AAS and AIR appear highly promising tools for the diagnosis of acute appendicitis, larger prospective studies are required to validate these results and establish definitive conclusions regarding their true diagnostic performance.
Conclusion
Among the evaluated clinical scoring systems, the Adult Appendicitis Score (AAS) and the Appendicitis Inflammatory Response (AIR) score demonstrated the highest diagnostic accuracy for acute appendicitis, with AAS showing the best overall performance. These scoring systems may represent reliable tools for supporting clinical decision-making and improving diagnostic confidence, potentially reducing unnecessary imaging or negative appendectomies. However, further validation in larger, more diverse cohorts is required before firm recommendations can be made.
Limitations
This study has an important limitation related to its relatively small sample size. The limited number of cases likely contributed to an overestimation of specificity, particularly for the AAS, which demonstrated an apparent specificity of 100%. This inflated specificity restricts the ability to draw definitive conclusions regarding the true diagnostic performance of the scoring systems. Larger prospective studies are therefore necessary to confirm these findings and ensure their generalizability. In addition, our study was the one-centered design.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Echevarria S, Rauf F, Hussain N, Zaka H, Ahsan N, Broomfield A, Akbar A, Khawaja UA, Farwa UE (2023) Typical and atypical presentations of appendicitis and their implications for diagnosis and treatment: a literature review. Cureus. ;15(4)10.7759/cureus.37024 PMC 1015240637143626 · doi ↗ · pubmed ↗
- 2Shuaib A, Shuaib A, Fakhra Z, Marafi B, Alsharaf K, Behbehani A (2017) Evaluation of modified Alvarado scoring system and RIPASA scoring system as diagnostic tools of acute appendicitis. World J Emerg Med 8(4):27610.5847/wjem.j.1920-8642.2017.04.005PMC 567596829123605 · doi ↗ · pubmed ↗