Acute Fulminant Cerebral Edema Caused by Coxsackievirus A6 Infection: A Case Report
Kang An, Juan Qian

TL;DR
A 6-year-old boy with Coxsackievirus A6 infection developed severe hand foot mouth disease leading to fatal cerebral edema and cardiopulmonary arrest.
Contribution
This case report highlights CV-A6 as a rare but severe cause of fulminant cerebral edema in hand foot mouth disease.
Findings
CV-A6 infection can cause severe neurological complications including fulminant cerebral edema.
A 6-year-old patient with CV-A6 developed fatal outcomes despite medical intervention.
CV-A6 is increasingly the main pathogen for hand foot mouth disease in China.
Abstract
In recent years, Coxsackievirus A6 (CV‐A6) has gradually replaced Enterovirus 71 (EV‐71) and Coxsackievirus A16 (CV‐A16) as the main pathogen causing hand foot mouth disease (HFMD) in China. This article reports a fatal case of HFMD caused by CV‐A6, leading to fulminant cerebral edema and cardiopulmonary arrest. A 6‐year‐old boy was admitted with a chief complaint of “fever for 1 day, two episodes of seizures”. On admission, the patient exhibited unresponsiveness, no spontaneous breathing, bilateral fixed and dilated pupils, complete muscle weakness, and loss of muscle tone. The brain computed tomography (CT) revealed diffuse decrease in brain parenchymal density. On the 3rd day of admission, the patient presented with a red rash on the hands, feet, knees, buttocks, and perianal area, and a nasopharyngeal swab was positive for CV‐A6. Considering the symptoms, physical examination,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
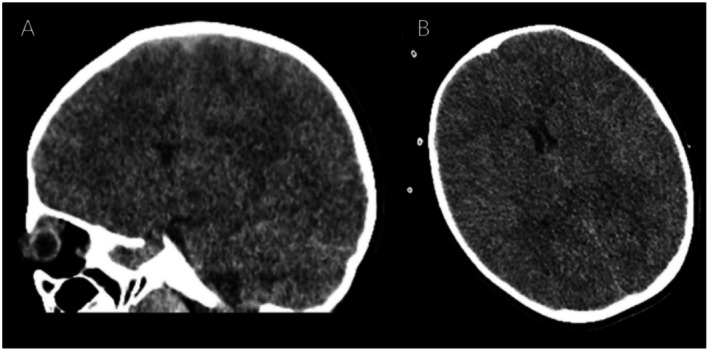 FIGURE 1
FIGURE 1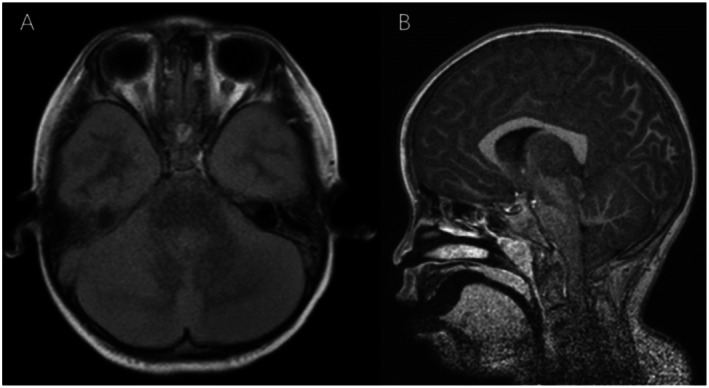 FIGURE 2
FIGURE 2| Laboratory test | Result | Normal value |
|---|---|---|
| WBCs, billion/L | 19.80 | 4–10 |
| Neutrophils, % | 81.8 | 33–74 |
| RBCs, trillion/L | 4.87 | 4.5–6.2 |
| HGB, g/dL | 128 | 131–179 |
| PLT, billion/L | 276 | 100–550 |
| CRP, mg/L | 18 | 0–8 |
| TBIL, μmol/L | 5.5 | 3–22 |
| DBIL, μmol/L | 0 | 0–5 |
| ALT, U/L | 185 | < 50 |
| AST, U/L | 253 | 15–46 |
| BUN, mmol/L | 3.8 | 3.2–7.1 |
| Cr, μmol/L | 55 | 58–110 |
| cTnI, μg/L | 2.38 | < 0.06 |
| NT‐proBNP, pg/mL | 247 | 0–125 |
| IL‐6, pg/mL | 95.45 | 1.05–15.80 |
| Influenza A | Negative | Negative |
| Influenza B | Negative | Negative |
| Case | 1 | 2 |
|---|---|---|
| Age (years) | 4 | 6 |
| Sex | Female | Male |
| Related viruses | Throat swab positive for CV‐A6 and stool swab positive for CV‐A6 | Nasopharyngeal swab positive for CV‐A6 |
| Initial symptoms and signs | Day 1: Fever of 39°C; Day 4: Rash on the face and trunk; Day 5: Generalized stiffness and spasms, cardiac arrest, respiratory arrest, dilated and fixed pupils, loss of corneal reflex and pupillary light reflex | Day 1: Fever of 39°C, generalized stiffness and spasms; Day 2: Generalized stiffness and spasms, cardiac arrest, respiratory arrest, dilated and fixed pupils, loss of corneal reflex and pupillary light reflex; Day 3: Rash on the hands, feet, and buttocks; Day 16: Brain death |
| Initial laboratory data | WBC 11300/μL, CRP 0.3 mg/dL; Cerebrospinal fluid: NA; Liver and kidney function: Normal; IL‐6: 32.1 pg/mL | WBC 19.80 × 109/L, HGB 128.0 g/L, PLT 276 × 109/L; Cerebrospinal fluid: NA; Liver and kidney function: Mildly elevated ALT and AST, normal for the rest; IL‐6: 95.45 pg/mL |
| Imaging | Brain CT: Marked cerebral edema | Brain CT: Diffuse decrease in brain parenchymal density, cerebral edema; Brain MRI: Cerebral edema, tonsillar herniation |
| EEG | No electrical activity | No electrical activity |
| Course of illness(days) | 21 | 57 |
| Outcome | Death | Death |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Herpesvirus Infections and Treatments · Infectious Encephalopathies and Encephalitis
Introduction
1
Hand, foot, and mouth disease (HFMD) is a common infectious disease among children, predominantly affecting those under the age of 5 years. The primary etiological agents responsible for HFMD include enterovirus 71, coxsackievirus (CV)‐A16, and others. In recent years, CV‐A6 has gradually replaced enterovirus 71 and CV‐A16 as the main pathogen causing HFMD in China [1, 2, 3].
The main symptoms and signs caused by CV‐A6 infection include fever, rash, peeling, and desquamation [3]. This article reports a case of acute fulminant cerebral edema in a 6‐year‐old male following CV‐A6 infection. After a literature review, a similar case of a 4‐year‐old female in Japan was found to have been previously reported [4]. Both patients were previously healthy children who developed cerebral edema after CV‐A6 infection ultimately leading to death, which is exceedingly rare.
The cause of acute fulminant cerebral edema caused by CV‐A6 infection is currently unclear. We aimed to analyze and summarize the clinical manifestations, laboratory findings, and imaging characteristics of this case as well as the literature review cases to raise awareness among clinicians, particularly in regions and seasons where enterovirus outbreaks are prevalent.
Case Presentation
2
A 6‐year‐old boy presented to the Emergency Department with a complaint of fever for 1 day and two episodes of seizures. The patient developed a fever 1 day before admission, with a maximum temperature of 39°C. Ibuprofen was used to reduce the fever. Six hours after the fever started, the patient experienced a seizure characterized by staring eyes and unresponsiveness, which lasted for several seconds before subsiding. There was no stiffness in the limbs, no urinary incontinence, and no cyanosis of the lips. Thirty minutes before admission, the patient came to our hospital due to a high fever. While waiting in the emergency department, the patient had a second seizure, which presented as a generalized convulsion. The patient was immediately taken into the resuscitation room for emergency treatment. Cardiac monitoring was initiated, oxygen was administered via face mask, and intramuscular midazolam was administered. Subsequently, the child developed cardiac and respiratory arrest, prompting immediate cardiopulmonary resuscitation and administration of adrenaline. After 15 min, the child regained spontaneous sinus rhythm. The child had a febrile seizure at the age of 2 years. The child was in good health with normal growth and development. There was no reported family history of neurological disorders.
The child was comatose and receiving tracheal intubation with positive pressure ventilation via a balloon catheter. The heart sounds were dull but regular, with coarse wet rales in the posterior lungs. The abdomen was flat without palpable liver or spleen. The Glasgow Coma Scale score was 3 (E1V1M1, range: 3–15). The pupils were dilated and fixed at 5 mm and unresponsive to light. Brudzinski's sign and Kernig's sign were negative. The patient had no physiological reflexes, including corneal, abdominal, patellar, and Achilles reflexes. Babinski's sign and Oppenheim's sign were also negative. The extremities were cold, and capillary refill time was 3 s.
Methods
3
The laboratory test results of the patient are shown in Table 1. On the day of admission, cranial computed tomography revealed a diffuse decrease in the density of the brain parenchyma and significant cerebral edema (Figure 1). On the third day of hospitalization, cranial magnetic resonance imaging revealed tonsillar herniation (Figure 2). On the third day of hospitalization, the patient presented with a red rash on the hands, feet, knees, buttocks, and perianal area. Nasopharyngeal swab PCR testing confirmed the presence of CV‐A6 infection. Combined with the patient's medical history, the final diagnosis was severe HFMD, CV‐A6 infection, and fulminant cerebral edema.
Cranial computed tomography showing a diffuse decrease in brain parenchymal density. (A) Sagittal view; (B) Transverse view.
Cranial magnetic resonance imaging. (A) Magnetic resonance imaging revealed widespread shallow cerebral sulci, indistinct gray‐white matter differentiation, generalized abnormal signal intensity in the cerebral and cerebellar parenchyma, with low signal on T1‐weighted images, high signal on T2‐weighted images, high signal on fluid attenuated inversion recovery images, and high signal on diffusion‐weighted imaging; (B) There was displacement of the cerebellar tonsils laterally located below the foramen magnum and becoming pointed. The lowest point is at the level of the C3 vertebral body.
Results
4
After admission, the patient was given mannitol to lower intracranial pressure. Fentanyl and midazolam were administered for pain relief and sedation. Additionally, measures for hypothermic brain protection were initiated. On the second day of hospitalization, the patient developed central diabetes insipidus, which was managed symptomatically. On the 16th day of admission, the patient was diagnosed with brain death. The patient died on the 57th day after admission.
Discussion
5
CV‐A6 is a single‐stranded RNA virus belonging to the Picornaviridae family and Enterovirus genus and is primarily transmitted through close contact and respiratory droplets [5]. CV‐A6 infection presenting initially with acute fulminant cerebral edema is extremely rare, with only 1 case [4] besides the present case reported in the literature. The characteristics of these 2 cases are summarized in Table 2. Both patients were previously healthy individuals with no underlying diseases. Each patient experienced the onset with high fever that was followed by seizures and the rapid occurrence of cardiac arrest. Severe cerebral edema was observed by brain CT of both patients. In the present case, the brain MRI revealed cerebral edema and tonsillar herniation, and it was postulated that tonsillar herniation might have directly contributed to the cardiac arrest. IL‐6 is a multifunctional cytokine that plays a critical role in various physiological and pathological processes. It is produced by a variety of cell types, including immune cells, fibroblasts, and endothelial cells [6, 7]. Excessive levels of IL‐6 can lead to tissue damage, organ failure, and even death. Both the patient in this case and the Japanese patient showed elevated levels of IL‐6, which we consider to be related to CV‐A6 infection. Monitoring the levels of IL‐6 dynamically in clinical practice can help understand the changes in the infection status of pediatric patients.
Recently, CV‐A6 has emerged as the primary pathogen causing HFMD in China. Zhao et al. analyzed relevant epidemiological data [8]. They found that annual outbreaks have been caused by CV‐A6 since 2013. CV‐A6 predominantly causes mild cases, and severe cases accounted for 0.1% [95% confidence interval (CI): 0%–0.2%]. Currently, research on risk factors associated with severe CV‐A6 infection is limited and primarily focuses on genetic and clinical factors. Meng et al. analyzed the genetic susceptibility of Han Chinese children with severe and mild HFMD caused by CV‐A6 infection [9]. The analysis revealed that the single nucleotide polymorphism (commonly known as SNP) rs10879355 was associated with severe CV‐A6 HFMD. The CC genotype had a higher risk of severe infection compared to the TT or TC genotypes [odds ratio (OR): 2.48; 95% CI: 1.34–4.56]. Additionally, the SNPs rs4290270 and rs10879355 were found to be in complete linkage disequilibrium.
Another study conducted by Li et al. [10] indicated that the presence of birth complications (OR: 4.18; 95% CI: 1.64–10.63), peak body temperature exceeding 39°C during the course of illness (OR: 4.04; 95% CI: 2.29–7.10), and being the first‐born child (OR: 2.17; 95% CI: 1.27–3.70) increased the risk of severe HFMD in children. On the other hand, breastfeeding (OR: 0.52; 95% CI: 0.32–0.87) and handwashing after play (OR: 0.58; 95% CI: 0.34–0.97) showed a negative correlation with the severity of the disease.
In this study, our patient was presented with acute cerebral edema caused by CV‐A6. There is an increasing number of large‐scale studies on pediatric acute cerebral edema. A study from Taiwan indicated that the incidence of acute cerebral edema among patients diagnosed with acute encephalitis was 2.4% (25/1038), with 48% of the patients in the age group of 5–8 years, and the mortality rate was 65%. Survivors all had neurological sequelae. The neurological symptoms of pediatric acute cerebral edema patients included altered consciousness, vomiting, and headache; among those, 76% of patients had seizures 24–48 h before the onset of severe signs of cerebral edema. Signs of brain herniation appeared 0–9 days after the appearance of neurological symptoms [11]. Another study from the United States revealed that patients diagnosed with acute encephalitis had an incidence of acute cerebral edema of 1.5% (30/1955), with a median age of 8.2 years (ranging from 1 to 18 years) and a high mortality rate of 80%. In comparison to non‐fulminant cerebral edema cases (14%), there was a higher proportion of individuals of Pacific Islander descent in the fulminant cerebral edema cases (44%, p < 0.01) [12]. Unlike the previous two studies, Nukui et al. proposed that acute cerebral edema is a new subtype of acute encephalopathy [13].
Considering the child's symptoms and signs of intracranial hypertension at the time, along with the imaging findings of diffuse cerebral edema and brain herniation, to avoid exacerbating the brain herniation with lumbar puncture, we did not perform lumbar puncture and cerebrospinal fluid testing on the child. We are also considering the most appropriate timing for lumbar puncture and cerebrospinal fluid examination in similar patients in the future, to avoid worsening the patient's condition. Due to the lack of cerebrospinal fluid testing in both this case and the reviewed case, combined with the patients' clinical presentation, laboratory data, and imaging characteristics, these two patients should be classified as having acute encephalopathy caused by viral infection.
Based on the findings of previous studies, we believe that fulminant cerebral edema, whether classified as a subtype of acute encephalitis or a subtype of acute encephalopathy, deserves significant attention due to its unique clinical course and radiographic characteristics. Prospective studies related to fulminant cerebral edema, particularly more aggressive surgical interventions such as ventricular drainage and decompressive craniectomy, warrant further exploration.
The early identification of fulminant cerebral edema and proactive intervention for reducing intracranial pressure is crucial for decreasing mortality. We suggest that clinicians in areas where enteroviruses are prevalent should suspect enterovirus infection when children present with severe neurological symptoms, regardless of the presence of typical skin and mucosal manifestations.
Conclusion
6
CV‐A6 infection can lead to severe neurological complications characterized by fulminant cerebral edema, which can be fatal.
Author Contributions
Kang An: data curation, methodology, writing – original draft. Juan Qian: conceptualization, supervision, validation.
Funding
The authors have nothing to report.
Consent
Verbal and written consent was obtained from the patient to publish this case.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1X. Tan , L. Li , B. Zhang , et al., “Molecular Epidemiology of Coxsackievirus A 6 Associated With Outbreaks of Hand, Foot, and Mouth Disease in Tianjin, China, in 2013,” Archives of Virology 160 (2015): 1097–1104, 10.1007/s 00705-015-2340-3.25680566 PMC 4629805 · doi ↗ · pubmed ↗
- 2Q. Liu , W. Zheng , C. Xia , et al., “Clinical Characteristics and Molecular Epidemiology of Coxsackievirus A 6 Hand, Foot, and Mouth Disease in Wenzhou, 2014,” Chinese Journal of Infectious Diseases 34, no. 11 (2016): 655–659, 10.3760/cma.j.issn.1000-6680.2016.11.004. · doi ↗
- 3P. Cui , Y. Li , C. C. Zhou , et al., “Clinical Analysis of 555 Outpatients With Hand, Foot and Mouth Diseases Caused by Different Enteroviruses,” Zhonghua Er Ke Za Zhi 57 (2019): 445–451, 10.3760/cma.j.issn.0578-1310.2019.06.009.31216802 · doi ↗ · pubmed ↗
- 4K. Aizaki , T. Tsuru , K. Okumura , and N. Kondo , “Three Pediatric Cases of Group A Coxsackievirus‐Associated Encephalitis/Encephalopathy,” No to Hattatsu 44 (2012): 397–400.23012870 · pubmed ↗
- 5J. Puenpa , S. Vongpunsawad , R. Österback , et al., “Molecular Epidemiology and the Evolution of Human Coxsackievirus A 6,” Journal of General Virology 97 (2016): 3225–3231, 10.1099/jgv.0.000619.27692044 · doi ↗ · pubmed ↗
- 6T. Tanaka , M. Narazaki , and T. Kishimoto , “IL‐6 in Inflammation, Immunity, and Disease,” Cold Spring Harbor Perspectives in Biology 6, no. 10 (2014): a 016295, 10.1101/cshperspect.a 016295.25190079 PMC 4176007 · doi ↗ · pubmed ↗
- 7C. A. Hunter and S. A. Jones , “IL‐6 as a Keystone Cytokine in Health and Disease,” Nature Immunology 16, no. 5 (2015): 448–457, 10.1038/ni.3153.25898198 · doi ↗ · pubmed ↗
- 8T. S. Zhao , J. Du , D. P. Sun , et al., “A Review and Meta‐Analysis of the Epidemiology and Clinical Presentation of Coxsackievirus A 6 Causing Hand‐Foot‐Mouth Disease in China and Global Implications,” Reviews in Medical Virology 30 (2020): e 2087, 10.1002/rmv.2087.31811676 · doi ↗ · pubmed ↗