Training requirements and associated factors for nursing assistants in Jiaxing City, China: a cross-sectional study in healthcare settings
Feng-Yan Pu, Li-Ping Yu, Hui-Ping Shan

TL;DR
This study evaluates the training needs and barriers for nursing assistants in Jiaxing City, China, and proposes improvements to training programs based on survey data.
Contribution
The study introduces a training requirements model for nursing assistants based on empirical data and identifies factors influencing training needs.
Findings
High training coverage exists, but training durations are short and formats are limited.
Preferred training formats include short, frequent sessions led by experienced staff and held in hospitals.
Training needs are higher among those in specific care models and those who previously received on-the-job training.
Abstract
The aim of this study is to systematically evaluate the training requirements of nursing assistants in clinical settings and to identify influencing factors, with the objective of developing a training requirements model to inform the design of evidence-based training programs. A cross-sectional design was implemented using stratified sampling across 48 healthcare institutions in Jiaxing City. A total of 1,600 questionnaires were distributed to nursing assistants, yielding 1,470 valid responses (valid response rate: 91.9%). Descriptive statistics, chi-square (χ2) tests, and multivariate logistic regression were conducted using SPSS version 22.0 to assess training coverage, content, format, and influencing factors. High training coverage was observed for both pre-employment (92.6%) and on-the-job (87.0%) programs; however, the reported training durations were relatively brief.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
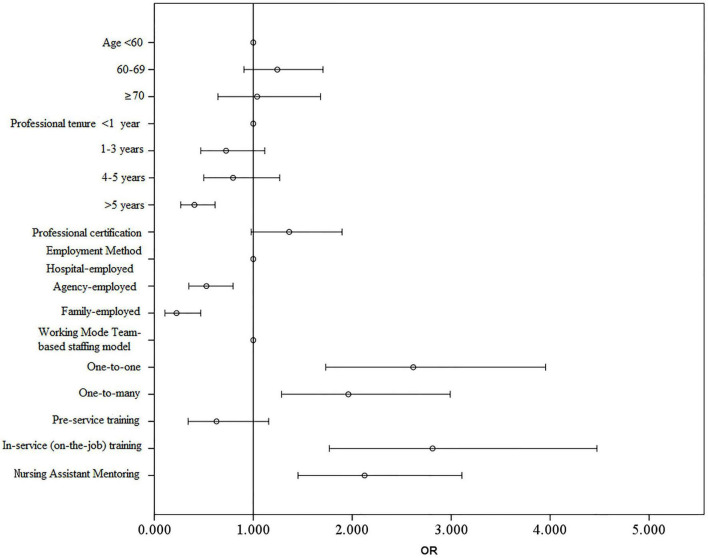 FIGURE 1
FIGURE 1| Item | Content | Number of | (%) |
|---|---|---|---|
| Pre-employment training | Yes | 1,361 | 92.6 |
| No | 109 | 7.4 | |
| Training duration | 1–3 days | 519 | 35.3 |
| 4–7 days | 457 | 31.0 | |
| 1–2 weeks | 167 | 11.3 | |
| More than 1 month | 132 | 8.9 | |
| 2–4 weeks | 86 | 5.8 | |
| Training hours | 1–3 h | 616 | 41.9 |
| More than 6 h | 317 | 21.5 | |
| 4–6 h | 235 | 15.9 | |
| Less than 1 h | 192 | 13.0 | |
| On-the-job training | Yes | 1,279 | 87.0 |
| No | 191 | 13.0 | |
| Training frequency | Once a month | 843 | 57.3 |
| Once a quarter | 208 | 14.1 | |
| Once every 6 months | 129 | 8.7 | |
| Once a year | 46 | 3.1 | |
| Other | 33 | 2.2 | |
| Over 1 year | 20 | 1.3 | |
| Centralized training method | Mentorship by senior nursing assistants | 978 | 66.5 |
| Classroom lectures | 932 | 63.4 | |
| Knowledge and skills assessment | 680 | 46.3 | |
| Site visits | 458 | 31.2 | |
| Skill competitions | 265 | 18.0 | |
| WeChat groups/official accounts | 258 | 17.6 | |
| Mobile apps | 200 | 13.6 | |
| Computer platforms | 139 | 9.5 |
| Category | Content | Analysis | Result | ||
|---|---|---|---|---|---|
| Requirement for training/retraining | χ2 |
| |||
| No requirement for training/retraining ( | Requirement for training/retraining ( | ||||
| Gender | Female | 257 | 952 | 0.380 | 0.537 |
| Male | 60 | 201 | |||
| Age | < 60 | 156 | 563 | 9.452 | 0.009 |
| 60–69 | 115 | 486 | |||
| > 70 | 46 | 104 | |||
| Educational level | Illiterate | 53 | 222 | 4.602 | 0.203 |
| Primary school | 138 | 482 | |||
| Junior high school | 91 | 284 | |||
| High school or above | 35 | 165 | |||
| Years of experience | < 1 year | 61 | 278 | 23.459 | < 0.001 |
| 1–3 years | 78 | 325 | |||
| 4–5 years | 50 | 244 | |||
| > 5 years | 128 | 306 | |||
| Relevant certificates | No | 111 | 304 | 9.182 | 0.002 |
| Yes | 206 | 849 | |||
| Employment type | Hospital-employed | 55 | 242 | 22.281 | < 0.001 |
| Labor dispatch | 237 | 883 | |||
| Family-employed | 25 | 28 | |||
| Work model | Team-based model | 65 | 163 | 7.819 | 0.020 |
| One-on-one care | 168 | 648 | |||
| One-to-many care | 84 | 342 | |||
| Pre-employment training | No | 34 | 75 | 6.452 | 0.011 |
| Yes | 283 | 1,078 | |||
| On-the-job training | No | 83 | 104 | 66.068 | < 0.001 |
| Yes | 233 | 1,046 | |||
| Mentorship by other nursing assistants | No | 80 | 132 | 45.731 | < 0.001 |
| Yes | 207 | 983 | |||
| Category |
| S.E. | Wald |
| OR | 95% CI | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| < 60 | 1.000 | ||||||
| 60–69 | 0.217 | 16.10% | 1.817 | 0.178 | 1.243 | 0.906 | 1.705 |
| > 70 | 0.038 | 24.50% | 0.024 | 0.876 | 1.039 | 0.642 | 1.68 |
|
| |||||||
| < 1 year | 1.000 | ||||||
| 1–3 years | −0.322 | 22.10% | 2.124 | 0.145 | 0.725 | 0.47 | 1.117 |
| 4–5 years | −0.228 | 23.70% | 0.922 | 0.337 | 0.796 | 0.5 | 1.268 |
| > 5 years | −0.902 | 21.10% | 18.214 | < 0.001 | 0.406 | 0.268 | 0.614 |
| Certificates | 0.31 | 16.80% | 3.385 | 0.066 | 1.363 | 0.98 | 1.897 |
|
| |||||||
| Hospital-employed | 1.000 | ||||||
| Labor dispatching | −0.64 | 21.00% | 9.29 | 0.002 | 0.527 | 0.35 | 0.796 |
| Family-employed | −1.491 | 37.60% | 15.741 | < 0.001 | 0.225 | 0.108 | 0.47 |
|
| |||||||
| Team-based model | 1.000 | ||||||
| One-on-one care | 0.962 | 21.10% | 20.863 | < 0.001 | 2.617 | 1.732 | 3.954 |
| One-to-many care | 0.673 | 21.50% | 9.772 | 0.002 | 1.961 | 1.286 | 2.991 |
| Pre-employment training | −0.464 | 31.00% | 2.237 | 0.135 | 0.629 | 0.342 | 1.155 |
| On-the-job training | 1.034 | 23.70% | 19.069 | < 0.001 | 2.812 | 1.768 | 4.473 |
| Mentorship by other nursing assistants | 0.754 | 19.40% | 15.044 | < 0.001 | 2.125 | 1.452 | 3.110 |
| Item | Options | Number of cases | (%) |
|---|---|---|---|
| Training format | Demonstrations and hands-on practice | 1,174 | 79.9 |
| Multimedia lectures | 699 | 47.6 | |
| Scenario simulations (countermeasure simulations) | 580 | 39.5 | |
| Experiential learning | 488 | 33.2 | |
| Simulation-based training systems | 468 | 31.8 | |
| Role-playing | 418 | 28.4 | |
| Training content | Qualities and requirements of nursing assistants | 989 | 67.3 |
| Communication skills | 870 | 59.2 | |
| Job responsibility | 859 | 58.4 | |
| Basic protection | 813 | 55.3 | |
| Identification and prevention of patient safety risks | 799 | 54.4 | |
| Relevant laws, regulations, and policies | 770 | 52.4 | |
| Recognition of common patient symptoms | 751 | 51.1 | |
| Work-related emotional management | 710 | 48.3 | |
| Hand hygiene | 699 | 47.6 | |
| Medical waste disposal | 690 | 46.9 | |
| Use of wheelchairs | 670 | 45.6 | |
| Work task/time management | 665 | 45.2 | |
| Management of abnormal urination and defecation | 633 | 43.1 | |
| Body hygiene | 630 | 42.9 | |
| Cleaning and disinfection | 628 | 42.7 | |
| Bed unit arrangement | 626 | 42.6 | |
| Feeding care | 626 | 42.6 | |
| Care for patients with cognitive impairment | 618 | 42.0 | |
| Oral hygiene | 615 | 41.8 | |
| Pain management for patients | 614 | 41.8 | |
| Patient mobility | 604 | 41.1 | |
| Head hygiene | 599 | 40.7 | |
| Assistance with dressing | 586 | 39.9 | |
| Toileting care | 578 | 39.3 | |
| Use of positioning cushions | 567 | 38.6 | |
| Medication management | 556 | 37.8 | |
| Use of walkers | 541 | 36.8 | |
| Use of stretchers | 539 | 36.7 | |
| Use of ice packs and hot water bags | 485 | 33.0 | |
| End-of-life care | 458 | 31.2 | |
| Postmortem care | 277 | 18.8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNursing education and management · Geriatric Care and Nursing Homes · Nursing Roles and Practices
Background
1
China, now navigating the world’s most rapid demographic aging, confronts healthcare challenges of an unprecedented scale. Projections suggest that by 2050, over 400 million citizens will be aged 65 or older (1, 2). This profound demographic transition, occurring against a backdrop of high chronic disease prevalence and a growing number of empty-nest households, is intensifying the societal demand for long-term care. The traditional reliance on family-provided care is increasingly strained by sustained low fertility rates, exposing the vulnerabilities of an informal system where caregivers often lack professional skills and face their own health challenges (3).
This growing care deficit intersects with a critical constraint within the formal health sector: a global shortage of registered nurses (4, 5). Inadequate nurse staffing not only fuels occupational burnout and turnover but also compromises the consistent delivery of safe, high-quality care (6). In response, health institutions across China have come to depend significantly on nursing assistants, often termed “healthcare caregivers,” to perform essential, non-specialized tasks under professional supervision (7). Unlike licensed nurses, this workforce enters the system without standardized formal education, creating a foundational challenge for quality assurance (8).
The current profile of nursing assistants in China, typically older, with limited formal education (72.71% completed junior high school or less), and exhibiting high turnover, further complicates the development of a skilled caregiving cohort (9). The central dilemma lies in this paradox: an escalating need for high-quality care is being met by a workforce for which effective, standardized training is not yet fully realized.
Existing literature adequately outlines these structural and educational challenges in broad terms. However, a critical gap persists: a lack of granular, context-specific evidence detailing how these general challenges translate into concrete, actionable training needs for nursing assistants at the local level. Studies that move beyond generic descriptions to identify the specific factors influencing training requirements within distinct socio-economic contexts, such as Jiaxing, a rapidly aging yet economically vibrant city in the Yangtze River Delta, are notably absent. This gap limits the development of targeted training frameworks.
To address this, our cross-sectional study investigates the existing training landscape for nursing assistants in Jiaxing and identifies key factors shaping their training requirements. The findings are intended to inform the creation of a more systematic, standardized, and tiered training approach, which is becoming an urgent necessity for building a resilient healthcare workforce capable of meeting the demands of an aging China.
Materials and methods
2
Design
2.1
A cross-sectional study design was employed.
Setting
2.2
The study was conducted in Jiaxing City, located in the core area of the Yangtze River Delta, China. Stratified sampling was conducted across seven sub-centers under the Jiaxing Nursing Quality Control Center, involving 48 healthcare institutions. These included tertiary Grade A and B hospitals, secondary Grade A and B hospitals, and long-term care facilities, ensuring adequate representation of institutional diversity. Before data collection, a preparatory meeting was held with the directors of all seven sub-centers. To ensure consistency and data quality, each sub-center director recruited 3–4 research assistants who underwent standardized training before participating in the study. A total of 28 trained research assistants were responsible for distributing questionnaires and guiding nursing assistants in completing them. Given that many nursing assistants were older and had lower educational levels, research assistants administered the questionnaires orally when necessary and recorded responses accordingly. Prior to data collection, research assistants received formal training, and all participants were provided with a brief explanation of the study’s purpose and significance.
Participants and samples
2.3
Participants were from 48 different health care institutions in Jiaxing. Stratified sampling was utilized to recruit nursing assistants employed at these institutions. Inclusion criteria were: ➀ aged 18 years or older; ➁ possessing adequate communication skills; and ➂ voluntary participation with informed consent. The required sample size was estimated based on statistical recommendations indicating a sample size of 10–20 times the number of variables (10). Considering a 10% expected attrition rate and a questionnaire comprising 60 items, the minimum required sample size was calculated to be 667 participants.
Measurement
2.4
Two instruments developed by Wang were used to collect data (11): the In-Service Training Status Questionnaire for Nursing Assistants and the In-Service Training Needs Questionnaire for Nursing Assistants (Supplementary material). The content validity index (CVI), including both item-level and scale-level indices, was evaluated by a panel of 10 experts specializing in nursing assistant training (2 directors of nursing departments, 6 clinical head nurses, and 2 faculty members from nursing colleges). The In-Service Training Status Questionnaire demonstrated a CVI of 0.904, test-retest reliability of 0.883, and a Cronbach’s α coefficient of 0.869. The In-Service Training Needs Questionnaire reported a CVI of 0.910, test-retest reliability of 0.893, and a Cronbach’s α coefficient of 0.879.
The questionnaire used in this study consisted of the following sections: (1) General information of the participants: including gender, age, educational background, and years of professional experience. (2) Current training status: whether the participant had received pre-employment training, duration of the pre-employment training, whether in-service training had been received, duration of in-service training, as well as the trainer’s background and the training location. Participants were also asked to indicate the difficulties encountered during pre-employment or in-service training (multiple choices allowed). (3) Training needs: whether the participant had a need for retraining, preferred training duration, preferred training methods, trainer background, and desired training content (multiple choices allowed).
Procedures
2.5
The survey was administered electronically using the “Wenjuanxing” (Questionnaire Star) platform. A total of 28 research assistants were recruited through the seven sub-centers. To support data integrity, research assistants visited participating institutions to assist with questionnaire administration. Before formal data collection, all research assistants received training on standardized procedures. Given the older age and relatively low educational levels of many nursing assistants, oral explanations and assistance with questionnaire completion were provided when needed. All respondents received a brief explanation outlining the study’s purpose and significance. Informed consent was obtained through a digital prompt requiring participants to select either “Yes” or “No.” Those who selected “No” were automatically excluded from participation. Participants were informed of their right to withdraw at any time. Once consent was confirmed, the questionnaire could be completed using mobile phones, computers, or other electronic devices. To prevent duplicate responses, each questionnaire could be submitted only once. Incomplete questionnaires were excluded from the final analysis. The data were stored and verified by two principal investigators to ensure accuracy and confidentiality.
Analysis
2.6
Data were analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, United States). Categorical variables were summarized as frequencies and percentages. Differences in retraining requirements (yes/no) across demographic and occupational characteristics were examined using the chi-squared (χ^2^) test. Variables with p < 0.05 in univariate analyses were entered into a multivariate logistic regression model (enter method) to identify independent factors associated with retraining requirements. The Omnibus Tests of Model Coefficients was used to assess the overall significance of the model coefficients. In this study, p = 0.001, indicating that at least one of the variables included in the model has an odds ratio with statistical significance; in other words, the model as a whole is meaningful. The Hosmer and Lemeshow Test was used to evaluate the goodness-of-fit of the model. Here, p = 0.544, suggesting that the information in the current dataset has been adequately captured by the model and that the model demonstrates a good fit. All statistical tests were two-tailed, with a significance level set at p < 0.05.
Results
3
Current training status of nursing assistants in Jiaxing
3.1
Of the 1,600 questionnaires distributed, 1,470 were valid (response rate: 91.9%). As shown in Table 1, coverage of pre-employment (92.6%) and on-the-job training (87.0%) was high. However, training was predominantly short in duration: 35.3% of participants received only 1–3 days of training, and 31.0% received 4–7 days. Hospital-based lectures (63.4%) and traditional mentorship (66.5%) were the most common training formats. Key barriers included scheduling conflicts (38.0%), limited smartphone use (31.7%), and insufficient practical content (9.7%). Despite these constraints, most participants (78.4%) expressed willingness to attend retraining. Among those unwilling, age-related limitations (40.7%) and lack of time (34.1%) were the primary reasons.
Univariate analysis of training and retraining requirements
3.2
Univariate analysis (Table 2) showed that retraining needs were significantly associated with most demographic and work-related factors (all p < 0.05), except educational level. Lower retraining needs were reported by nursing assistants aged ≥ 70 years and those with more than 5 years of experience. In contrast, higher retraining needs were observed among participants holding professional certificates, working under one-on-one or one-to-many care models, and those employed by hospitals or third-party agencies. Notably, individuals who had received pre-employment or on-the-job training, or who were mentored by experienced nursing assistants, reported higher retraining needs, suggesting increased awareness of skill gaps following prior training exposure.
Multivariate analysis of training and retraining requirements
3.3
Variables significant in univariate analysis were entered into a multivariate logistic regression model (Table 3 and Figure 1). Longer work experience (> 5 years) and employment via labor dispatch or direct family hire remained independently associated with lower retraining needs. Conversely, one-on-one or one-to-many care models, prior on-the-job training, and mentorship by other nursing assistants were independently associated with higher retraining needs (all p < 0.05). These findings indicate that both work organization and prior training exposure play key roles in shaping perceived retraining demand.
Adjusted odds ratios for factors influencing nursing assistants’ retraining intent (multivariate logistic regression). The forest plot shows adjusted odds ratios from multivariate logistic regression for factors associated with nursing assistants’ willingness to participate in retraining. Higher retraining intent was observed among assistants working in one-to-one or one-to-many care models, those who had completed on-the-job training, and those mentored by experienced caregivers (OR ≈ 2–4). Conversely, assistants with ≥ 5 years of experience or employed through agencies or directly by families showed lower retraining intent (OR < 1).
Preferences of nursing assistants for retraining
3.4
Preferences for retraining are summarized in Table 4. Participants favored short-term programs (1–3 days; 49.5%) delivered on a monthly basis (56.3%). Senior nursing assistants (67.8%) and nursing experts (61.6%) were the most preferred trainers. Hospital training centers (64.6%) and inpatient wards (58.0%) were the preferred venues. Hands-on training, particularly bedside mentorship, was overwhelmingly favored (92.1%), whereas digital training tools were rarely used (< 20%). The most requested content areas were professional skills (67.3%), communication skills (59.2%), and patient safety (54.4%). Demand for specialized topics such as end-of-life care was comparatively lower (31.2%).
Discussion
4
The findings indicated high coverage rates of both pre-employment and on-the-job training among nursing assistants in Jiaxing. However, The length and depth of training were uneven. Most participants had completed pre-employment or on-the-job training, as reported by 92.6 and 87.2%, respectively, indicating that healthcare institutions in the region place considerable emphasis on professional training. Nevertheless, training duration was predominantly short, with 31.0% of participants receiving training lasting 4–7 days and 35.3% receiving training lasting only 1–3 days. This situation contrasts with the more systematic and structured training models established in developed countries such as the United States, the United Kingdom, Germany, and Japan (12–14). For example, the Health Education England Health Assistant Certification Program requires trainees to complete 15 competency-based modules within 12 weeks of employment, covering topics such as basic life support and infection control. These modules include both theoretical and practical components and culminate in certification. In addition, trainees must complete 10 online learning modules and practical sessions (15). In Germany, nursing care personnel are required to hold at least a secondary vocational school diploma, be 16 years or older, and be physically and mentally fit. Training must include a minimum of 2,100 h of theoretical instruction and 2,500 h of practical experience over at least 18 months, with alternating theoretical and clinical components (16). The limited duration and fragmented nature of current programs have led to suboptimal training outcomes, consistent with the findings of Li et al. (7).
Demographic characteristics among nursing assistants appeared to constrain the implementation of diversified training approaches. More than half of the participants were aged over 60 years (51.1%), with a majority being women. These characteristics contributed to the continued reliance on traditional training formats such as hospital-based lectures (63.4%) and mentorship provided by senior nursing assistants (66.5%). Moreover, limited use of digital instructional tools, including mobile applications and WeChat groups, hindered improvements in training accessibility and effectiveness, in line with previous observations (17).
Multiple factors were associated with training and retraining requirements. Univariate analysis demonstrated that nursing assistants aged 60–69 reported higher retraining requirements compared to those aged over 70. Similarly, those with shorter employment durations exhibited greater training demand than those with longer tenures. Individuals holding professional certificates expressed higher retraining requirements than their uncertified counterparts. Nursing assistants employed by hospitals or third-party agencies reported greater training requirements than those hired directly by families. The study found that practitioners working under one-to-one or one-to-many care models exhibited higher training needs than those engaged in team-based collaboration. Additionally, prior participation in pre-employment or on-the-job training and exposure to mentorship from experienced caregivers were associated with greater interest in retraining.
Multivariate logistic regression analysis confirmed that higher retraining requirements were significantly associated with caregivers working in one-on-one or one-to-many models, those who had previously received on-the-job training, and those mentored by peer caregivers (p < 0.05). These findings emphasize the influence of individual characteristics, workplace structures, and prior training experiences on ongoing educational needs.
Current preferred training models among nursing assistants in Jiaxing
4.1
Training duration and frequency
4.1.1
Participants demonstrated a preference for short-term training lasting 1–3 days (49.5%), likely reflecting the high clinical workload and the need to acquire skills efficiently. Additionally, 56.3% preferred training to occur monthly, indicating a need for continuous skill updates in response to evolving clinical demands. These findings indicate that training programs should be designed to optimize the balance between instructional depth and time efficiency, minimizing disruption to routine clinical responsibilities.
Training instructors
4.1.2
Senior nursing assistants (67.8%) and nursing experts (61.6%) were most frequently identified as preferred trainers. This reflects a dual emphasis on both practical experience and theoretical expertise. Practical instruction from experienced nursing assistants can promote procedural accuracy, while expert-led sessions can provide theoretical grounding. The integration of these two formats may form an iterative “practice-theory” cycle that enhances training effectiveness.
Training venues and formats
4.1.3
Preferred venues included hospital training centers (64.6%) and inpatient wards (58.0%), indicating a preference for learning environments embedded in real clinical contexts. These venues facilitate direct observation and application of clinical workflows, thereby expediting the transfer of knowledge. Traditional bedside mentorship was the most favored instructional format (72.2%). However, the adoption of digital training tools remained limited (below 20%), indicating an area for improvement. Blended models incorporating virtual simulations alongside in-person mentorship could offer a more flexible and scalable training approach.
Training content
4.1.4
Core areas of interest included professional skills and competencies (67.3%), communication techniques (59.2%), and patient safety practices (54.4%). These priorities align with essential role competencies for nursing assistants. In contrast, demand for training in specialized scenarios, such as end-of-life care, was relatively low (31.2%), possibly reflecting limited exposure to such situations in routine care. Nonetheless, the low demand highlights a potential training gap. Gradual introduction of advanced content, such as case-based modules for specialized scenarios, may improve preparedness and expand the scope of care delivery.
Comparison with existing literature on training needs of nursing assistants
4.2
Our findings align with prior studies showing that high training coverage does not necessarily translate into adequate competency development among nursing assistants. Although more than 90% of participants in Jiaxing reported receiving pre-service or in-service training, the programs were generally brief and heterogeneous, with most lasting fewer than 7 days. This contrasts sharply with the multi-week, standardized training curricula required in countries such as the United States, the United Kingdom, Germany, and Japan, where longer training durations allow for repeated practice, supervision, and skill consolidation (18–20). Consistent with Li et al., fragmented and short-term training models are associated with limited learning gains and substantial variability in care competence (21).
The demographic profile of the workforce further shapes training delivery and uptake. In line with previous reports, our cohort was predominantly older, with more than half aged ≥ 60 years, which partly explains the continued reliance on traditional teaching formats such as hospital lectures and senior-assistant mentoring. Digital training modalities, including mobile applications and social media platforms, were used by fewer than 20% of respondents. Similar patterns have been reported in other studies of aging care workforces, where limited digital literacy and the absence of age-adapted online content restrict the effectiveness of e-learning approaches (22).
Our analysis also adds nuance to the literature by identifying subgroups with distinct retraining needs. Nursing assistants aged 60–69 years, those with shorter work experience, professional certification, and hospital- or agency-based employment demonstrated stronger demand for retraining, whereas longer tenure, labor-dispatch arrangements, or direct family employment were associated with lower demand, even after adjustment for confounders (23). These findings are consistent with studies suggesting that job stability, perceived career progression, and organizational support strongly influence motivation for continued learning. Moreover, care models involving one-to-one or one-to-many assignments, prior in-service training, and active mentorship were associated with higher retraining interest, underscoring the role of workplace structure and supervisory support in sustaining learning motivation (24).
Finally, respondents’ preferences for retraining are largely consistent with international evidence emphasizing practicality and feasibility. Short, high-frequency, on-site training sessions led by experienced nursing assistants or clinical experts were favored, with strong emphasis on hands-on practice. Core competencies, communication skills, and patient safety were prioritized over specialized topics such as end-of-life care, echoing findings from similar workforce surveys. While digital tools remain underutilized, the literature suggests that blended approaches, combining face-to-face instruction with simple, case-based digital resources, may gradually expand training reach and address unmet educational needs without increasing cognitive or technological burden (25).
Limitations
4.3
Several limitations should be noted. First, although this study provides a large, city-wide snapshot of training utilization and retraining demand among nursing assistants, its cross-sectional design precludes causal inference. Second, data were collected using a self-administered questionnaire with a relatively large number of items, which may have increased respondent burden, the risk of input errors, and susceptibility to recall or social-desirability bias. Third, while stratified sampling was conducted across 48 healthcare institutions in Jiaxing, an economically developed city in China’s Yangtze River Delta region, the findings may not be fully representative of nursing assistants in less developed or rural areas. Differences in workforce structure, training resources, and institutional support may limit the generalizability of the results. Future studies using longitudinal designs, streamlined instruments, and multi-regional samples are needed to strengthen causal interpretation and external validity.
Conclusion
5
This study shows that while the overall coverage of nursing assistant training in Jiaxing is high, important gaps remain in training duration, delivery methods, content relevance, and sustained participation. These limitations reduce the practical impact of current programs despite their broad reach. Given the study’s cross-sectional design and reliance on self-reported data, the findings should be interpreted as descriptive rather than causal. From a practical perspective, training policies should shift from an emphasis on coverage to a focus on quality. Extending course length, standardizing core curricula, and integrating low-threshold digital resources may improve training effectiveness. A tiered strategy could prioritize new entrants, certificate holders, and nursing assistants in personalized care roles as early adopters, while experienced or family-employed assistants may require tailored incentives to re-engage. Embedding mentorship and short, regular training sessions within routine ward workflows offers a feasible approach to sustainable skill development. Future research should employ longitudinal or interventional designs and include diverse regions to assess training effectiveness over time and improve generalizability. Drawing on international long-term care workforce models, the development of a structured, standardized training and assessment framework aligned with China’s healthcare context may support the professionalization and long-term sustainability of the nursing assistant workforce.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fang EF Xie C Schenkel JA Wu C Long Q Cui H A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. (2020) 64:101174. 10.1016/j.arr.2020.101174 32971255 PMC 7505078 · doi ↗ · pubmed ↗
- 2Dong B Yue J Cao L Yang M Ge N Qiukui H Transformation of a geriatric department in China. J Am Geriatr Soc. (2018) 66:184–90. 10.1111/jgs.15217 29168884 · doi ↗ · pubmed ↗
- 3Chen X Giles J Wang Y Zhao Y. Gender patterns of eldercare in China. Fem Econ. (2018) 24:54–76. 10.1080/13545701.2018.1438639 32863728 PMC 7451666 · doi ↗ · pubmed ↗
- 4Wong KL Chua WL Griffiths P Goh QLP Low KWC Tan JQA Teamwork between registered nurses and unlicensed assistive personnel in acute care settings: a scoping review. Int J Nurs Stud Adv. (2025) 8:100293. 10.1016/j.ijnsa.2025.100293 39906753 PMC 11791319 · doi ↗ · pubmed ↗
- 5World Health Organization. State of the World’s Nursing Report: 2020. World Health Organization (2020).
- 6Shah MK Gandrakota N Cimiotti JP Ghose N Moore M Ali MK. Prevalence of and factors associated with nurse burnout in the US. JAMA Netw Open. (2021) 4:e 2036469. 10.1001/jamanetworkopen.2020.36469 33538823 PMC 7862989 · doi ↗ · pubmed ↗
- 7Li F Ding Y Du J. Investigation on the current situation of the use and management of medical nursing assistants in 44 tertiary hospitals. Chin J Nurs. (2022) 57:2629–34. 10.3761/j.issn.0254-1769.2022.21.011 · doi ↗
- 8Blay N Roche MA. A systematic review of activities undertaken by the unregulated nursing assistant. J Adv Nurs. (2020) 76:1538–51. 10.1111/jan.14354 32190928 · doi ↗ · pubmed ↗