Cardiovascular remodeling: key mechanisms and clinical implications linking sarcopenia and heart failure
Jinghong Yang, Xinyu Zhang, Jun Zhong

TL;DR
This paper explores how heart failure and muscle loss are linked through shared mechanisms like inflammation and how this understanding can lead to better treatments.
Contribution
The paper provides a unified framework for the mechanistic links between sarcopenia and heart failure, highlighting novel therapeutic targets.
Findings
Cardiovascular remodeling mediates the bidirectional relationship between sarcopenia and heart failure.
Shared mechanisms include chronic inflammation, oxidative stress, and insulin resistance.
Targeting these pathways could improve outcomes for both conditions.
Abstract
Sarcopenia and heart failure (HF) are interconnected through a bidirectional relationship in which cardiovascular remodeling serves as a critical mediator. This review examines the shared pathophysiological mechanisms—such as chronic inflammation, oxidative stress, and insulin resistance—that underlie both conditions. By integrating recent clinical and experimental evidence, we emphasize the role of cardiovascular remodeling in aggravating muscle loss in sarcopenia and cardiac dysfunction in HF. Furthermore, we discuss novel therapeutic targets directed at disrupting these common pathways. This analysis offers a unified framework for understanding the mechanistic links between sarcopenia and HF, with implications for future research and clinical strategies aimed at enhancing patient outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
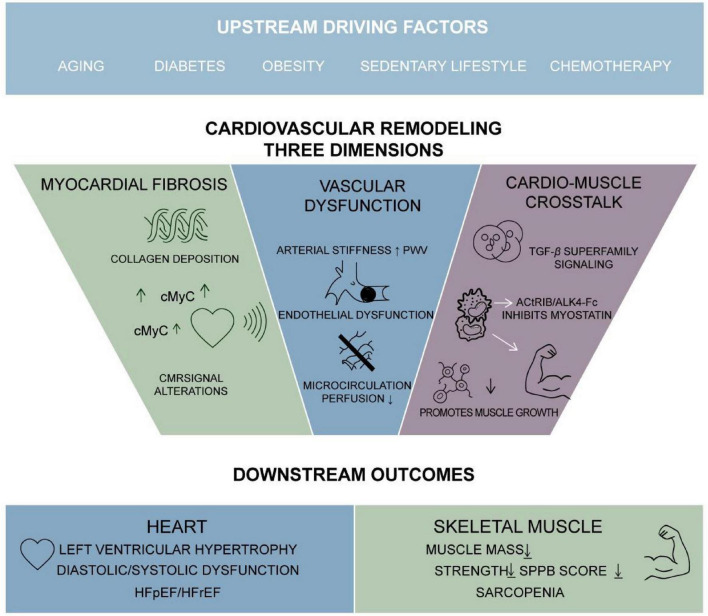 FIGURE 1
FIGURE 1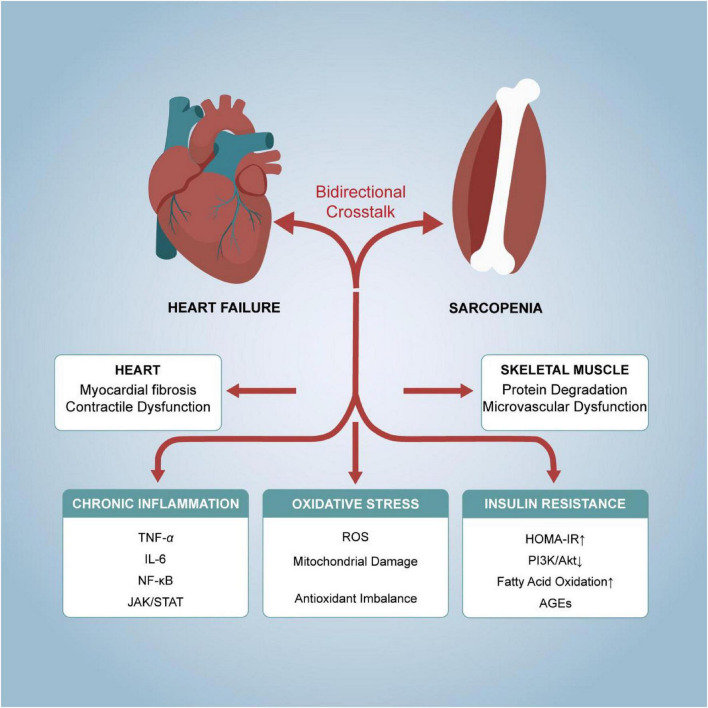 FIGURE 2
FIGURE 2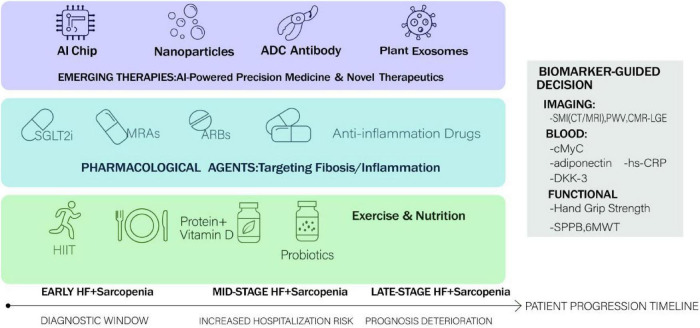 FIGURE 3
FIGURE 3| Mechanism | Role in sarcopenia | Role in HF | Proposed centrality | Rationale |
|---|---|---|---|---|
| Chronic inflammation | Activates NF-κB → muscle proteolysis | Promotes fibrosis, endothelial dysfunction | High | Directly links muscle wasting and cardiac remodeling |
| Oxidative stress | Disrupts Ca2+ handling, contractile proteins | Induces apoptosis, fibrosis | Medium | Amplifies damage in both tissues |
| Insulin resistance | ↓ PI3K/Akt →↓ protein synthesis | ↓ glucose uptake → metabolic shift | High | Core metabolic dysregulation in both |
| Neurohormonal activation | ↑ Catabolism via RAAS and SNS | ↑ Preload/afterload, fibrosis | Medium | Modulated by drugs (ACEi/ARB) |
| Biomarker | Sample type | Primary clinical context | Role/association | Key limitations |
|---|---|---|---|---|
| Leptin | Serum/plasma | Obesity, HF, cachexia | Positively correlates with LVEF; negatively with LV mass index. Reflects adiposity and may indicate adipose tissue dysfunction. | Strongly influenced by total fat mass; exhibits complex, non-linear relationships with clinical outcomes. |
| Adiponectin | Serum/plasma | HF, metabolic syndrome, sarcopenia | Elevated levels predict sarcopenia in males; correlates with BNP and left atrial diameter. A marker of metabolic dysregulation. | Paradoxically high in advanced HF/cachexia (“adiponectin paradox”); lacks disease specificity. |
| Thoracic skeletal muscle index (SMI) | CT/MRI | HFrEF, sarcopenic obesity | Values < 42.75 cm2/m2, especially with obesity, identify adverse LV remodeling and poor prognosis. Direct quantitative measure of muscle mass. | Requires advanced imaging (cost, radiation exposure for CT); diagnostic thresholds may vary across populations. |
| Phase angle | Bioelectrical impedance analysis (BIA) | HF, malnutrition, sarcopenia | A value < 5.45° is indicative of risk; reflects cellular membrane integrity and body cell mass. | Sensitive to hydration status; results vary with measurement device and protocol. |
| Cardiac myosin-binding protein C (cMyC) | Serum | General population, chronic myocardial injury | Associated with focal myocardial fibrosis and left ventricular remodeling; a potential indicator of systemic musculoskeletal health. | Still in exploratory research phases; clinical utility within the sarcopenia-HF dyad awaits validation. |
| Pulse wave velocity (PWV) | Non-invasive vascular assessment | Vascular aging, sarcopenia, HF | Significantly elevated in individuals with sarcopenia; provides a direct link between arterial stiffness and muscle loss. | Requires specialized equipment; measurements are influenced by concurrent blood pressure. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutrition and Health in Aging · Muscle Physiology and Disorders · Cardiovascular and exercise physiology
Introduction
1
Sarcopenia and heart failure (HF) commonly coexist in older adults and are interconnected through a reciprocal interplay that adversely affects clinical morbidity and mortality. Heart failure with reduced ejection fraction (HFrEF) is clinically defined as symptomatic HF with a left ventricular ejection fraction (LVEF) ≤ 40%, as per the 2021 ESC Guidelines and 2022 AHA/ACC/HFSA recommendations. Sarcopenia, as operationalized by the European Working Group on Sarcopenia in Older People (EWGSOP2), is characterized by low muscle strength, reduced muscle quantity or quality, and impaired physical performance. Converging evidence indicates that cardiovascular remodeling acts as a central pathophysiological link between these two conditions (1, 2). While sarcopenia increases susceptibility to HF and accelerates its clinical course, HF itself promotes muscle wasting via mechanisms such as persistent low-grade inflammation, endocrine dysregulation, and physical deconditioning. This bidirectional relationship is particularly pronounced in high-risk phenotypes such as sarcopenic obesity. For example, in diabetic individuals with HF and reduced ejection fraction (HFrEF), the co-occurrence of low muscle mass and obesity correlates with maladaptive left ventricular (LV) remodeling and unfavorable outcomes, underscoring the need for targeted clinical recognition (3, 4).
Cardiovascular remodeling—encompassing structural and functional alterations in the heart and vasculature, including arterial stiffening, LV hypertrophy, and microvascular dysfunction—represents a common pathway in both sarcopenia and HF (5). For the purpose of this review, cardiovascular remodeling is operationally defined as the integrated spectrum of maladaptive structural and functional alterations affecting three interrelated compartments: the myocardium (e.g., hypertrophy, fibrosis), the macrovasculature (e.g., arterial stiffening, endothelial dysfunction), and the microcirculation. These alterations collectively contribute to a state of impaired cardiac efficiency, increased hemodynamic burden, and compromised peripheral perfusion. The mechanistic link to sarcopenia lies in the resultant chronic reduction in oxygen and nutrient delivery to skeletal muscle, concomitant with a systemic milieu of inflammation and metabolic dysregulation that adversely affects muscle protein turnover. A systematic review and meta-analysis support this association, revealing that elevated pulse wave velocity (PWV), a recognized indicator of arterial stiffness, is significantly linked to sarcopenia, implying a shared vascular basis for muscle deterioration and cardiac impairment (6).
Inflammatory and metabolic disturbances further underpin this relationship. Adipokines such as leptin and adiponectin contribute to cardiac remodeling processes; leptin exerts cardiodepressive effects, while adiponectin reflects metabolic dysfunction associated with inflammation and muscle loss in cardiovascular patients (7). Interventions like high-intensity interval training (HIIT) have been shown to improve skeletal muscle perfusion and vascular reactivity in older adults, suggesting that enhancing microcirculatory function and lowering blood pressure may alleviate sarcopenia and its cardiovascular sequelae (8). Emerging strategies, including probiotic supplementation, also exhibit potential in moderating cardiac remodeling and sarcopenia metrics by influencing inflammatory states, oxidative stress, and gut microbiota composition, thereby modulating key pathways such as Wnt signaling involved in muscle homeostasis (5, 9).
A deeper understanding of these interconnected mechanisms is crucial to designing effective interventions that disrupt the vicious cycle linking sarcopenia and HF, with the ultimate goal of improving health outcomes in an aging global population.
Epidemiological association between sarcopenia and HF
2
Sarcopenia, characterized by the progressive and generalized loss of skeletal muscle mass, strength, and function, is increasingly recognized as a major comorbidity and a critical determinant of clinical outcomes in heart failure (HF) (2, 10). Epidemiological studies reveal a substantial disease burden, with a global pooled prevalence of approximately 34% among HF patients (5). This prevalence is markedly influenced by clinical setting and disease severity, escalating to 55% in hospitalized cohorts compared to 26% in ambulatory patients, and is further modulated by sex and HF phenotype, being more common in males and those with reduced ejection fraction (HFrEF) (11). The pathophysiological interplay between sarcopenia and HF is driven by a self-perpetuating cycle of chronic systemic inflammation, neurohormonal activation, metabolic dysregulation, and anabolic resistance, which collectively promote muscle protein catabolism. This muscle wasting is not merely a peripheral epiphenomenon but is independently associated with exacerbated physical frailty, diminished functional capacity as measured by tools like handgrip strength, and impaired quality of life (12–14).
Emerging evidence supports a bidirectional predictive relationship between sarcopenia and HF. Sarcopenia, particularly when accompanied by low handgrip strength, independently predicts incident HF in older adults (hazard ratio ≈ 1.5–2.0), likely mediated through vascular dysfunction and chronic inflammation. Conversely, HF—especially HFrEF—predicts accelerated muscle loss attributable to reduced perfusion, anabolic resistance, and physical inactivity. Notably, sarcopenia serves as a strong prognostic indicator, with severe cases conferring a 2.5-fold increased risk of cardiac mortality or HF rehospitalization within 1 year (12, 15, 16). Objective measures such as low phase angle (<5.45°) and reduced spot urinary creatinine concentration have been validated as biomarkers for identifying high-risk patients (17, 18). However, integrated prediction models that combine both sarcopenia and HF remain underdeveloped; future studies should incorporate imaging biomarkers (e.g., pulse-wave velocity, cardiac myosin-binding protein C) along with functional assessments to improve risk stratification. Therefore, early diagnosis and management of sarcopenia—through targeted resistance exercise training and comprehensive nutritional support—represent a promising therapeutic strategy to disrupt this pathophysiological cycle and improve long-term prognosis and wellbeing in patients with HF.
Temporal dynamics and causal interplay: unraveling the sequence
2.1
The intricate relationship between cardiovascular remodeling and sarcopenia raises a pivotal question regarding temporal precedence and causal directionality. The sequence is likely bidirectional and phenotype-dependent. In scenarios such as chronic hypertension or primary valvulopathies, maladaptive cardiovascular remodeling may constitute the inciting event. Progressive myocardial fibrosis and vascular stiffening impair cardiac output reserve and peripheral perfusion, ultimately fostering an environment conducive to the development of sarcopenia. Conversely, primary sarcopenia, arising from aging, sedentarism, or nutritional deficiencies, can instigate a pathophysiological cascade characterized by systemic inflammation, insulin resistance, and reduced physical activity. This cascade promotes endothelial dysfunction and arterial stiffening, thereby driving adverse cardiac remodeling and potentially precipitating or exacerbating HF. In clinical practice, particularly among the elderly, these processes frequently coexist and engage in a vicious, self-perpetuating cycle, making the delineation of a primary driver challenging. Future longitudinal studies employing serial, multimodality assessments of cardiac structure/function and muscular parameters are essential to elucidate predominant temporal sequences across distinct clinical phenotypes.
Shared pathophysiological mechanisms between sarcopenia and heart failure
3
The interplay between sarcopenia and HF is orchestrated through several overlapping pathways, with chronic inflammation and insulin resistance emerging as central drivers due to their dual impact on cardiac structure and skeletal muscle metabolism (Table 1 and Figure 1).
The bidirectional interplay between sarcopenia and heart failure mediated by shared pathophysiological mechanisms.
The role of chronic inflammation
3.1
Chronic inflammation plays a significant role in the pathogenesis of sarcopenia and heart failure (HF). Inflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) are markedly elevated in both conditions (19–21). TNF-α promotes muscle protein degradation by activating the nuclear factor-κB (NF-κB) pathway, thereby contributing to the development of sarcopenia (19, 22, 23). Concurrently, TNF-α exacerbates the pathological progression of heart failure by inhibiting myocardial contractility (24). IL-6 further intensifies cardiac remodeling by promoting myocardial fibrosis and vascular endothelial dysfunction. Studies indicate that serum IL-6 levels in HF patients correlate positively with the severity of left ventricular dysfunction, while IL-6 levels in sarcopenia patients are closely associated with diminished muscle mass and function (25–27). The combined action of these inflammatory mediators not only accelerates functional decline in both muscle and heart but also amplifies the inflammatory response by activating downstream signaling pathways (such as JAK/STAT), thereby establishing a vicious cycle (28).
The inflammatory response also plays a central role in cardiovascular remodeling. Under chronic inflammatory conditions, inflammatory mediators such as TNF-α and IL-6 promote myocardial fibrosis and vascular endothelial dysfunction, leading to left ventricular hypertrophy and diastolic dysfunction (29). Furthermore, inflammation accelerates extracellular matrix degradation by activating matrix metalloproteinases (MMPs), thereby exacerbating cardiac structural alterations. In patients with sarcopenia, the persistent release of inflammatory mediators not only causes muscle wasting but also indirectly promotes cardiovascular remodeling by impairing myocardial cell energy metabolism and contractile function (21, 30, 31). For instance, TNF-α exacerbates cardiac dysfunction by suppressing insulin signaling pathways and intensifying insulin resistance in cardiomyocytes. Consequently, inflammation serves not only as a shared pathological basis for sarcopenia and HF but also as a crucial bridge linking the two conditions.
The contribution of oxidative stress
3.2
Oxidative stress plays a critical role in the pathogenesis of both sarcopenia and HF. Reactive oxygen species (ROS) accumulate due to mitochondrial dysfunction and impaired antioxidant defenses, leading to cellular damage (32, 33). In skeletal muscle, excessive ROS disrupts calcium handling and contractile proteins, accelerating muscle atrophy. In the myocardium, ROS contribute to cardiomyocyte apoptosis, fibrosis, and impaired excitation-contraction coupling (34). Oxidative stress also exacerbates insulin resistance, further impairing muscle and cardiac metabolism. Therapeutic strategies targeting ROS, such as antioxidants or mitochondrial enhancers, may help preserve muscle mass and cardiac function in these conditions (35–37).
Beyond this, oxidative stress exerts strikingly similar effects on both cardiac and skeletal muscle function. Within cardiomyocytes, reactive oxygen species (ROS) impair mitochondrial DNA and membrane lipids, leading to reduced ATP production and abnormal calcium regulation, which in turn disrupts cardiac contraction and relaxation. Similarly, in skeletal muscle, ROS inhibit myofibril synthesis while promoting their degradation, resulting in diminished muscle mass and strength (38). Notably, oxidative stress further exacerbates functional decline by impairing vascular endothelial function, thereby reducing blood perfusion to both skeletal and cardiac muscle. For instance, impaired skeletal muscle microvascular function in HF patients correlates closely with elevated ROS levels, while antioxidant therapies (such as N-acetylcysteine) can partially reverse this damage (39).
Insulin resistance and metabolic dysregulation
3.3
Insulin resistance is a common metabolic feature of sarcopenia and heart failure. In sarcopenia, insulin resistance reduces muscle protein synthesis by inhibiting the PI3K/Akt signaling pathway, whilst activating the UPS system to accelerate protein degradation (40). In HF, insulin resistance diminishes glucose uptake by cardiomyocytes, shifting energy dependence toward fatty acid oxidation (41). This process is not only inefficient but also generates substantial ROS, further damaging myocardial tissue. Furthermore, insulin resistance exacerbates inflammatory responses in muscle and heart tissue by promoting the release of inflammatory mediators such as TNF-α and IL-6. Clinical studies demonstrate a significant correlation between the insulin resistance index (HOMA-IR) in HF patients and the severity of sarcopenia, indicating a close metabolic link between the two conditions (42).
Metabolic abnormalities (such as hyperglycemia and dyslipidemia) similarly promote cardiovascular remodeling through multiple pathways. Hyperglycemia activates inflammatory and oxidative stress pathways via advanced glycation end products (AGEs), leading to myocardial fibrosis and vascular stiffening (43). Dyslipidemia exacerbates cardiac contractile dysfunction by promoting lipotoxicity and impairing mitochondrial function in cardiomyocytes (44). In patients with sarcopenia, metabolic abnormalities further deteriorate muscle function by reducing blood flow perfusion and energy supply to muscles. For instance, skeletal muscle microvascular dysfunction in diabetic patients is closely associated with metabolic abnormalities, and improved metabolic control (e.g., via SGLT2 inhibitors) can partially reverse this damage. Consequently, metabolic abnormalities represent not only a shared pathophysiological basis for sarcopenia and HF but also a critical target for intervention (45, 46).
The key role of cardiovascular remodeling
4
Cardiovascular remodeling represents a fundamental pathological process in numerous cardiac conditions, characterized by structural and functional alterations in both the myocardium and vasculature (Figure 2). This complex process involves myocardial fibrosis, vascular dysfunction, and intricate cross-talk between cardiac and skeletal muscle systems. In salt-sensitive cardiovascular disease, high dietary sodium promotes myocardial fibrosis through non-hemodynamic mechanisms involving redox-sensitive and profibrotic pathways, contributing to diastolic dysfunction and potentially heart failure with preserved ejection fraction (HFpEF) (47, 48). Cardiac magnetic resonance (CMR) imaging has emerged as a crucial diagnostic tool for assessing myocardial fibrosis, ventricular remodeling, and mitral regurgitation severity, enabling early detection before irreversible damage occurs (49, 50). The development of novel biomarkers such as cardiac myosin binding protein C (cMyC) further enhances our understanding of chronic myocardial injury and left ventricular remodeling in general populations. Chemotherapy-induced cardiovascular injury demonstrates how myocardial edema, inflammation, and fibrosis can be detected through advanced imaging techniques, highlighting the sensitivity of CMR in identifying early, potentially reversible tissue remodeling. Machine learning approaches have improved risk stratification in mitral valve prolapse by identifying distinct echocardiographic phenotypes associated with myocardial fibrosis and clinical outcomes, emphasizing the importance of integrating left ventricular dilatation and fibrosis assessment with quantitative mitral regurgitation evaluation for optimal intervention timing (51, 52).
Cardiovascular remodeling as a central mediator linking sarcopenia and heart failure.
Myocardial fibrosis and sarcopenia
4.1
Myocardial fibrosis and sarcopenia share common pathophysiological pathways that extend beyond their individual clinical manifestations, representing interconnected processes in cardiovascular and musculoskeletal health (1). Myocardial fibrosis, characterized by fibroblast activation and excessive extracellular matrix collagen deposition, contributes significantly to ventricular stiffness and both systolic and diastolic dysfunction, ultimately progressing to heart failure (53). The relationship between cardiac fibrosis and muscle wasting becomes evident through several mechanisms, including shared inflammatory pathways, neurohormonal activation, and metabolic dysregulation (54). In primary mitral regurgitation, substantial left ventricular volume overload leads to adverse cardiac remodeling and myocardial replacement fibrosis, which parallels the muscle degradation processes observed in sarcopenia. The emerging application of sodium magnetic resonance imaging (23Na-MRI) provides novel insights into myocardial sodium overload and its association with fibrotic remodeling, while circulating biomarkers like cMyC demonstrate associations with focal myocardial fibrosis and left ventricular remodeling in general populations (55–57). These imaging and biomarker advancements reveal how cardiac structural changes may reflect or contribute to systemic muscle wasting processes. Furthermore, therapeutic interventions targeting myocardial fibrosis, including mineralocorticoid receptor antagonists, angiotensin receptor blockers, and sodium-glucose cotransport 2 inhibitors, may have implications for addressing skeletal muscle deterioration, suggesting potential cross-benefits in managing both cardiac and musculoskeletal health.
Vascular dysfunction and skeletal muscle atrophy
4.2
Vascular dysfunction and skeletal muscle atrophy maintain a bidirectional relationship where impaired vascular function contributes to muscle wasting, while muscle deterioration further exacerbates vascular compromise. The activin receptor signaling pathway provides crucial insights into this interconnection, as demonstrated by the heterodimeric ligand-trapping fusion protein ActRIIB:ALK4-Fc, which exhibits distinct ligand binding properties affecting both vascular regulation and muscle growth (58). This therapeutic agent specifically sequesters ActRIIB ligands known to inhibit muscle growth while avoiding the trapping of vascular regulatory ligand bone morphogenetic protein 9 (BMP9), highlighting the delicate balance required in modulating these interconnected systems. The differential effects observed in retinal explant assays between ActRIIB:ALK4-Fc and its homodimeric variant ActRIIB-Fc underscore the complexity of vascular-muscle interactions. In clinical contexts such as chemotherapy-induced cardiovascular injury, vascular remodeling occurs alongside myocardial tissue changes, with CMR capable of detecting not only established morphologic and functional abnormalities but also early signs of vascular compromise. The improvement in neuromuscular junction abnormalities and alleviation of acute muscle fibrosis observed in murine models of Duchenne muscular dystrophy and amyotrophic lateral sclerosis following ActRIIB:ALK4-Fc treatment further emphasizes the therapeutic potential of targeting shared pathways between vascular function and muscle preservation (59).
Cardiac-skeletal muscle cross-talk
4.3
The pathophysiological interplay between heart failure (HF) and sarcopenia is mediated by specific molecular pathways, with the TGF-β/activin signaling axis being a central mechanism (60). Elevated circulating activins in HF activate the ActRIIB/ALK4 receptors on skeletal muscle, directly promoting proteolysis and muscle wasting. This explains the efficacy of agents like ActRIIB:ALK4-Fc in preclinical models, which simultaneously ameliorate cardiac dysfunction and muscle loss by blocking this shared pathway (61).
Clinically, this organ crosstalk is substantiated by biomarkers and phenotypic clustering. For instance, cardiac-specific biomarkers such as cMyC correlate not only with myocardial injury but also with systemic muscle depletion. Similarly, machine learning-derived echocardiographic phenotypes link specific patterns of cardiac remodeling to a higher risk of generalized sarcopenia, indicating that primary cardiac pathology can broadcast systemic signals affecting muscle health (59). Furthermore, circulating biomarkers like cMyC reflect not only cardiac remodeling and focal myocardial fibrosis but also associate with cardiovascular risk factors and ventricular dysfunction, serving as potential indicators of systemic muscle health status (59).
Future research should move beyond documenting coexistence to defining the precise hierarchy and timing of signals within this cross-talk. Key questions include whether sarcopenia in HF is primarily driven by specific cardiac-derived factors (e.g., from failing myocardium versus activated fibroblasts) or by amplified systemic inflammation. Furthermore, the role of skeletal muscle as an endocrine organ, potentially releasing myokines that feedback to accelerate or attenuate cardiac remodeling, remains poorly explored. Defining these directional signals will be crucial for identifying whether therapeutic strategies should primarily target the heart to protect muscle, the muscle to support the heart, or nodal points within their shared signaling network.
Clinical research evidence on sarcopenia and heart failure
5
Recent meta-analysis summarizing the association between sarcopenia and HF
5.1
Recent meta-analyses have revealed a strong association between sarcopenia and heart failure (HF). A systematic review and meta-analysis involving 5,476 participants demonstrated that pulse wave velocity was significantly higher in individuals with sarcopenia compared to those without (SMD = 0.73, 95% CI 0.39–1.08), suggesting a marked association between increased aortic stiffness and sarcopenia (62, 63). The study further found that elevated PWV positively correlates with the risk of developing sarcopenia, suggesting vascular dysfunction may represent one potential mechanism underlying the co-morbidity of sarcopenia and HF. Another cardiac MRI study in diabetic patients with HFrEF demonstrated that sarcopenic obesity (SO) patients exhibited more severe left ventricular dilatation and dysfunction, with a 3-fold increased risk of cardiovascular adverse events compared to non-SO patients (HR = 3.03, 95% CI 1.39–6.63) (64). Collectively, these findings suggest that sarcopenia not only constitutes an independent risk factor for HF but may also worsen HF prognosis by influencing cardiac remodeling and vascular dysfunction.
Interventional studies: effects of exercise training and nutritional supplementation
5.2
Regarding intervention measures, high-intensity interval training has demonstrated dual improvements for both sarcopenia and heart failure. A randomized controlled trial found that after 6 weeks of HIIT, skeletal muscle microvascular reactivity to contraction significantly increased in older adults aged 65–85 years (blood perfusion rising from 1.8 ± 0.63 to 2.3 ± 0.8 AU), alongside concurrent improvements in cardiorespiratory fitness and blood pressure control (65, 66). In addition, regarding nutritional interventions, probiotic supplementation offers multiple benefits under cardiac remodeling conditions: by modulating the Wnt signaling pathway (significantly correlated with improved grip strength, p < 0.05), and reducing inflammatory markers such as hs-CRP, it may concurrently mitigate sarcopenia and HF progression. Notably, improvements in Short Physical Performance Battery (SPPB) scores were closely correlated with changes in muscle metabolic markers including Dkk-3 and SREBP-1, suggesting that combined interventions may produce synergistic effects via the metabolic-inflammatory axis (67).
Biomarkers for predicting sarcopenia and HF risk
5.3
Biomarker studies have revealed the pivotal role of leptin and adiponectin in the association between sarcopenia and heart failure (56). Studies in cardiovascular surgery patients demonstrate that serum adiponectin levels correlate positively with cardiac function parameters such as BNP and left atrial diameter (LAD), whilst leptin correlates positively with LVEF but negatively with LV mass index (68, 69). Notably, adiponectin independently predicts sarcopenia in male patients (OR not reported, p < 0.05), and the possible mechanisms potentially involve activation of the pro - inflammatory factor TNF - α and abnormal muscle protein metabolism (7). Additionally, skeletal muscle index (SMI) of the thoracic skeleton—as a surrogate marker for muscle mass—effectively distinguishes high - risk phenotypes in HFrEF patients (70). When SMI < 42.75 cm^2^/m^2^ coexists with obesity, patients exhibit more pronounced left ventricular remodeling and poorer outcomes. These biomarkers provide objective evidence for early identification of high - risk populations for sarcopenia - associated HF (71). We have summarized some potential biomarkers and their correlations and shortcomings, which are summarized in Table 2.
Future research directions and clinical implications
6
Targeting common mechanisms for therapeutic intervention
6.1
Future research should prioritize the development of therapies targeting the shared pathological mechanisms between HF and sarcopenia. For instance, artificial intelligence (AI) holds promise for these specific conditions by analyzing multi-omics data to identify novel therapeutic targets, predict individual patient responses, and optimize treatment strategies, thereby moving toward precision medicine in cardiometabolic-musculoskeletal disorders (72, 73). Another relevant approach is the exploration of bioactive compounds, such as resveratrol, for their multi-dimensional benefits including anti-inflammatory and mitochondrial-protective effects, which are pertinent to both cardiac and muscle pathology. However, their clinical application is limited by poor bioavailability, necessitating research into improved formulations or delivery systems for these patient populations.
Multidisciplinary integrated intervention strategies
6.2
A multidisciplinary approach is essential for managing the sarcopenia-heart failure continuum, integrating nutritional support, pharmacotherapy, and tailored physical interventions (Figure 3). For HF, this includes guideline-directed medical therapy (e.g., ACE inhibitors, beta-blockers), salt-restricted diets, and cardiac rehabilitation. For sarcopenia, management combines protein and vitamin D supplementation with resistance and aerobic training to improve muscle mass and function (74). AI can aid in personalizing these strategies through the integrated analysis of body composition, cardiac function parameters, and biomarker profiles. Incorporating psychosocial support is also crucial for enhancing adherence and quality of life. Future initiatives should focus on standardizing multidisciplinary care pathways and utilizing digital health tools to improve coordination between cardiology, geriatrics, nutrition, and rehabilitation services (75).
Integrated and personalized therapeutic strategies for disrupting the sarcopenia-heart failure cycle.
Development of personalized treatment approaches
6.3
Personalized medicine for HF and sarcopenia involves tailoring interventions based on individual patient profiles, leveraging biomarkers, AI, and advanced delivery systems. AI algorithms analyzing patient-specific multi-omics data can help predict disease progression, the risk of cachexia/sarcopenia, or response to specific therapies, enabling timely intervention. Furthermore, technologies like nanoparticle-based delivery systems could be adapted to enhance the bioavailability and targeted action of drugs or nutraceuticals relevant to muscle and cardiac health (e.g., specific anti-inflammatory agents). Plant-derived extracellular vesicles (EVs) are also being explored as novel delivery platforms with potential applications in regenerative medicine, which may be relevant for tissue repair in these conditions. The primary focus for future research must be the validation of such personalized approaches in large-scale clinical trials specific to HF and sarcopenia, incorporating robust functional and patient-reported outcomes.
Current guideline incorporation of sarcopenia in HF management
6.4
A review of major HF guidelines reveals limited explicit integration of sarcopenia. The 2022 AHA/ACC/HFSA guidelines mention “muscle wasting” as a comorbidity but lack screening recommendations. The 2021 ESC Guidelines note nutritional support in cachexia but do not address sarcopenia specifically. Chinese HF guidelines (2024) acknowledge sarcopenia as a prognostic factor but offer no standardized assessment protocol. This gap underscores the need for guideline updates that incorporate routine sarcopenia screening (e.g., SARC-F questionnaire, grip strength) in HF clinics, along with tailored interventions (resistance exercise, protein supplementation) to break the detrimental cycle.
Conclusion
7
In conclusion, cardiovascular remodeling emerges as a pivotal pathophysiological nexus linking sarcopenia and heart failure, driven by shared mechanisms of chronic inflammation, oxidative stress, and metabolic dysregulation. This interplay establishes a vicious cycle wherein cardiac dysfunction and skeletal muscle wasting mutually reinforce each other, leading to worsened clinical outcomes. Evidence underscores the prognostic significance of sarcopenia in HF populations and highlights the potential of targeting common pathways—such as with exercise training, nutritional support, and novel pharmacological agents—to disrupt this detrimental crosstalk. Moving forward, future research should prioritize the development of integrated, multidisciplinary management strategies and leverage advances in biomarker discovery, imaging technologies, and artificial intelligence to enable early detection and personalized therapeutic interventions. By addressing both cardiac and muscular health in a coordinated manner, we can aspire to improve functional capacity, quality of life, and long-term survival for patients afflicted with these interrelated conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Curcio F Testa G Liguori I Papillo M Flocco V Panicara V Sarcopenia and heart failure. Nutrients. (2020) 12:211. 10.3390/nu 12010211 31947528 PMC 7019352 · doi ↗ · pubmed ↗
- 2Lena A Anker MS Springer J. Muscle wasting and sarcopenia in heart failure-the current state of science. Int J Mol Sci. (2020) 21:6549. 10.3390/ijms 21186549 32911600 PMC 7555939 · doi ↗ · pubmed ↗
- 3Campbell P Rutten FH Lee MM Hawkins NM Petrie MC. Heart failure with preserved ejection fraction: everything the clinician needs to know. Lancet. (2024) 403:1083–92. 10.1016/S 0140-6736(23)02756-3 38367642 · doi ↗ · pubmed ↗
- 4Redfield MM Borlaug BA. Heart failure with preserved ejection fraction: a review. JAMA. (2023) 329:827–38. 10.1001/jama.2023.2020 36917048 · doi ↗ · pubmed ↗
- 5de Jorge-Huerta L Marco-Alacid C Grande C Velardo Andrés CA. Narrative review of the diagnosis and treatment of Sarcopenia and malnutrition in patients with heart failure. Nutrients. (2024) 16:2717. 10.3390/nu 16162717 39203852 PMC 11357594 · doi ↗ · pubmed ↗
- 6Amarasekera AT Chang D Schwarz P Tan TC. Does vascular endothelial dysfunction play a role in physical frailty and sarcopenia? A systematic review. Age Ageing. (2021) 50:725–32. 10.1093/ageing/afaa 237 33951149 · doi ↗ · pubmed ↗
- 7Komici K Dello Iacono A De Luca A Perrotta F Bencivenga L Rengo G Adiponectin and Sarcopenia: a systematic review with meta-analysis. Front Endocrinol. (2021) 12:576619. 10.3389/fendo.2021.576619 33935962 PMC 8082154 · doi ↗ · pubmed ↗
- 8Liu QQ Xie WQ Luo YX Li YD Huang WH Wu YX High intensity interval training: a potential method for treating Sarcopenia. Clin Interv Aging. (2022) 17:857–72. 10.2147/CIA.S 366245 35656091 PMC 9152764 · doi ↗ · pubmed ↗