Case Report: Complete response to the concurrent neoadjuvant radiation therapy and pembrolizumab in a locally recurrent, chemotherapy-refractory undifferentiated pleomorphic sarcoma of bone
Brina A. Patel, Jason T. Smith, Sintawat Wangsiricharoen, Wei-Lien Wang, Patrick P. Lin, Ahsan Farooqi, Elise F. Nassif Haddad, Kamal Ummed, Alexander F. Mericli, David M. Adelman, John Andrew Livingston, Anthony P. Conley

TL;DR
A patient with a rare and aggressive bone cancer achieved a complete response using a combination of radiation therapy and pembrolizumab, an immune checkpoint inhibitor.
Contribution
This case report presents the first documented complete and durable response to pembrolizumab and radiotherapy in chemotherapy-refractory undifferentiated pleomorphic sarcoma of bone.
Findings
The patient achieved a complete pathologic response after concurrent pembrolizumab and radiotherapy.
Molecular profiling showed high PD-L1 expression and high tumor mutational burden, suggesting immunogenicity.
The patient remained recurrence-free for 24 months following treatment.
Abstract
Undifferentiated pleomorphic sarcoma of bone (UPS-B) is a rare and aggressive cancer that accounts for a small fraction of bone sarcomas. Compared to both undifferentiated pleomorphic sarcoma of soft tissue (UPS-ST) and osteosarcoma, UPS-B demonstrates lower chemosensitivity and a poorer prognosis, with reported five-year survival rates of only 7.3%. Standard management has generally mirrored osteosarcoma regimens, surgery, multi-agent chemotherapy, and radiotherapy, though the optimal approach remains undefined. In contrast, immune checkpoint inhibitors (ICIs) targeting PD-1/PD-L1 have shown promising activity in UPS-ST but minimal efficacy in osteosarcoma, leaving the role of ICIs in UPS-B largely unknown. We report the case of a 61-year-old male with recurrent, chemotherapy-refractory UPS-B of the left ilium who achieved a complete and durable response with concurrent neoadjuvant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
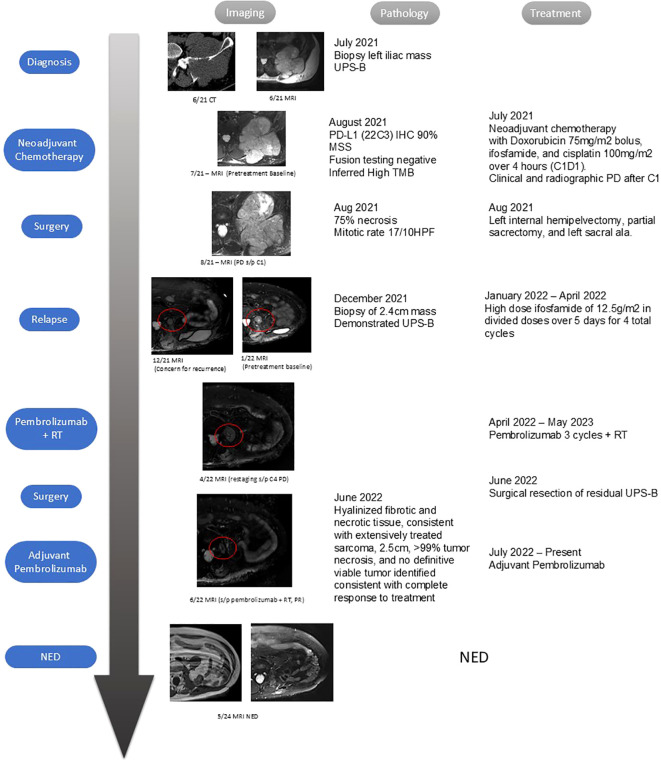 Figure 1
Figure 1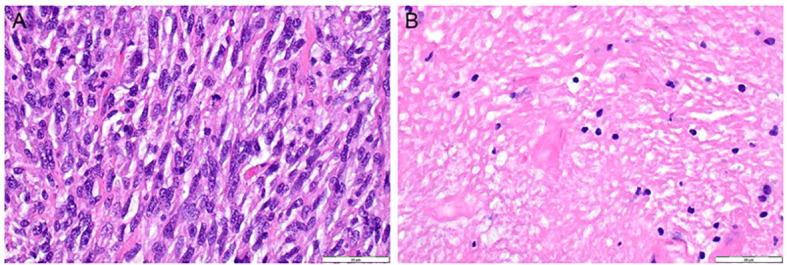 Figure 2
Figure 2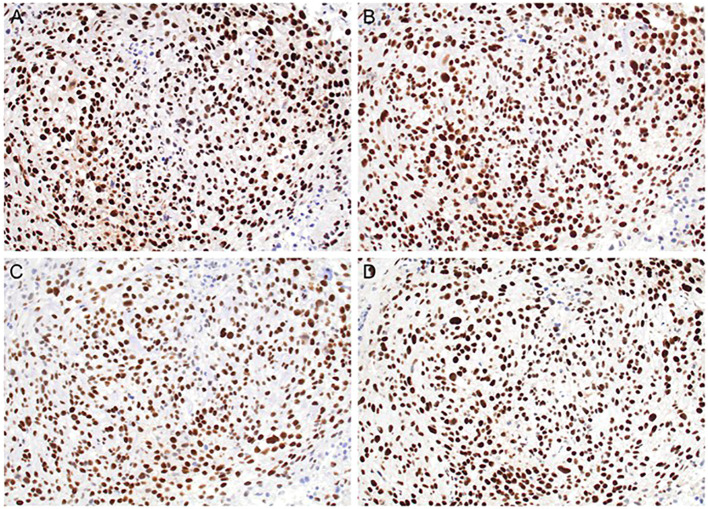 Figure 3
Figure 3| Somatic mutations | |||||
|---|---|---|---|---|---|
| Gene | Standardized nomenclature (HGVS) | Location | DNA change | Variant type | COSMIC ID |
| ARID1A | Exon 5 | SNV | Missense | ||
| ARID1A | Exon 16 | SNV | Missense | ||
| ATR | Exon 45 | SNV | Nonsense | COSM35421 | |
| AXL | Splice (intron 14) | Splice | Unknown | ||
| BRAF | Exon 15 18 | SNV | Missense | COSM471 | |
| CDKN2A | Exon 2 | SNV | Missense | COSM12476 | |
| CHEK1 | Exon 6 | SNV | Missense | ||
| ERBB2 | Exon 22 | Complex | Missense | ||
| EZH2 | Exon 18 | SNV | Missense | COSM49154 | |
| FANCA | Exon 28 | SNV | Missense | ||
| FBXW7 | Exon 2 | SNV | Missense | ||
| FGFR2 | Exon 12 | SNV | Missense | ||
| FGFR2 | Exon 9 | SNV | Missense | ||
| FGFR2 | Exon 8 | SNV | Missense | ||
| FGFR2 | Exon 7 | SNV | Missense | ||
| NBN | Exon 10 | SNV | Missense | ||
| NF1 | Exon 30 | SNV | Nonsense | COSM28019 | |
| NTRK3 | Exon 19 | SNV | Missense | ||
| POLE | Exon 35 | SNV | Missense | ||
| RAC1 | Exon 2 | SNV | Missense | ||
| ROS1 | Exon 36 | SNV | Missense | ||
| SMARCA4 | Exon 4 | SNV | Missense | ||
| SMARCA4 | Splice? (Exon 16) | SNV | Unknown | ||
| STK11 | Exon 6 | SNV | Missense | ||
| TERT | UTR5 | SNV | |||
| TP53 | Exon 7 | SNV | Missense | COSM10812 | |
| TSC1 | Exon 17 | SNV | Missense | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Chromatin Remodeling and Cancer · Bone Tumor Diagnosis and Treatments
Introduction
Undifferentiated pleomorphic sarcomas (UPS) are a highly aggressive type of cancer that can develop in either soft tissues or bones, but UPS of bone (UPS-B) is exceedingly rarer and has a worse prognosis than UPS of the soft tissue (UPS-S) (1, 2). The distinction between UPS-S and UPS-B is significant, as it highlights the need for treatment tailored to the specific type of UPS. Traditionally, UPS-B has been treated similarly to primary bone tumors like osteosarcoma, using surgery and combination chemotherapy regimens containing methotrexate, cisplatin, and doxorubicin (1, 3), but the optimal chemotherapy course for UPS-B remains unclear (3, 4). It is important to note that studies have also highlighted UPS-B’s lower chemosensitivity than osteosarcoma (3, 5, 6). The 5-year survival rate for UPS-B patients is around 7.3%, considerably lower than that of osteosarcoma at 77% (1, 2, 5).
Immune checkpoint inhibitors (ICIs), which target the PD-1/PD-L1 pathway to boost immune response against cancerous cells, have revolutionized cancer care across different cancer types but unfortunately have very limited efficacy in osteosarcomas (7, 8). However, ICIs have been shown to be effective in advanced UPS-S: in a study examining the safety and efficacy of pembrolizumab in advanced sarcomas, UPS-S emerged as being particularly sensitive to immunotherapy, with a 23% objective response rate, suggesting the potential of this class of drugs for this sarcoma subtype (9, 10). Two studies evaluated neoadjuvant ICI for surgically resectable UPS-S in combination with radiation therapy (RT): the first was a phase 2 randomized trial with nivolumab (PD-1 inhibitor) ± ipilimumab (CTLA4 inhibitor), which demonstrated a pathologic response rate of 89% in 10 patients with UPS-S, and the second trial, SARC032, was a randomized trial investigating the addition of pembrolizumab to standard of care (SOC) RT in stage 3 soft-tissue sarcoma (85% of patients had UPS-S) and demonstrated a significant improvement in 2-year disease-free survival from 53% to 70% (11). Collectively, these findings suggest that concurrent ICI and RT may be more effective than single-agent therapy for treating UPS-S, but the response of UPS-B to this strategy remains largely unclear. Notably, it is unknown whether UPS-B will have a similar response to ICI as osteosarcoma or as UPS-S. Herein, we report on a case of a patient with locally recurrent ups-B with a complete durable response to a combination of pre-operative ICI and RT (Figure 1).
Chronological progression of patient exams and treatments. Stage of treatment is listed from top to bottom, with dates of related imaging, pathology findings, and subsequent treatments from left to right.
Case description
A 61-year-old male with a past medical history of osteoarthritis, benign prostatic hyperplasia, repaired hiatal hernia, hypertension, neuropathy, and a stable pulmonary nodule for 10 years presented with progressive left hip pain in February 2021, soon noticing a palpable left hip mass in June 2021. Imaging of the mass conducted in June 2021 displayed a large destructive tumor arising in the left upper iliac bones with cortical breakthrough of soft tissue to the left psoas muscle (11.0 cm × 12.0 cm × 10 cm). In July 2021, a biopsy of the tumor was performed and revealed a UPS-B with an observed mitotic rate of 7 per single high-power field and the presence of foci of necrosis (Figure 2A).
Representative Pathology Slides Before and After Treatment. (A) Pre-treatment, December 2021, H&E, 400x. (B) Post-treatment, June 2022, H&E, 400x. Extensive hyalinization with scattered lymphocytes.
A Solid Tumor Genomic Assay was conducted using next-generation sequencing (NGS) through a targeted 500-gene panel (FoundationOne CDx). Variant calling was performed using GRCh37/hg19 as the reference genome. Variants were prioritized based on allele frequency, predicted pathogenicity, cancer-relevance annotation, and presence in oncogenic pathways. Copy-number alterations were assessed using NGS-based computational CNV algorithms as part of the FoundationOne CDx analytic pipeline. On the biopsy specimen, the resulting DNA report highlighted multiple missense mutations in oncogenes and tumor suppressor genes: ARID1A, ATR, AXL, BRAF, CDKN2A, CHEK1, ERBB2, EZH2, FANCA, FBXW7, FGFR2, NBN, NF1, NTRK3, POLE, RAC1, ROS1, SMARCA4, STK11, TERT, TP53, and TSC1. Germline DNA was not available for comparison; therefore, the identified alterations are described as tumor-identified variants rather than definitively somatic. The presence of numerous tumor-identified alterations across oncogenic pathways suggests a relatively elevated mutational burden based on this targeted panel, which may be associated with increased tumor immunogenicity (Table 1). Immunochemistry demonstrated retained nuclear expression of the mismatch repair proteins MLH1, MSH2, MSH6, and PMS2, consistent with proficient mismatch repair (Figure 3). PD-L1 immunohistochemistry using clone 22C3 showed a tumor proportion score of 90%, with membranous staining in 90% of viable tumor cells. NY-ESO-1 immunohistochemistry was negative, with no tumor cell labeling observed (0%) (data not shown).
Mismatch repair (MMR) protein immunohistochemistry demonstrating retained nuclear expression of all four markers at 200× magnification. (A) MLH1, (B) MSH2, (C) PMS2, and (D) MSH6. Retained expression across all markers is consistent with proficient mismatch repair status.
The multidisciplinary recommendation was for the patient to receive neoadjuvant chemotherapy following osteosarcoma-like regimens. The patient began a course of doxorubicin 75 mg/m^2^ bolus, zinecard, and cisplatin 100mg/m^2^ over 4h in the inpatient setting in July 2021 (C1D1). However, the initial treatment plan was complicated by acute kidney injury, with an increase in creatinine from 0.91 mg/dl to 2.91 mg/dl. In August 2021, the patient developed multiple thrombosis emboli from the right subclavian vein and pulmonary embolism. Post C1, the patient reported an enlargement of the mass, which was confirmed with an MRI in August 2021, revealing the mass measured 15.5 cm × 14.3 cm × 12 cm. Thus, the chemotherapy was discontinued in August 2021, and the patient underwent surgical resection consisting of a left internal hemipelvectomy, partial sacrectomy, and left sacral ala in August 2021. Postoperative complications included upper extremity weakness (transient ischemic attack) and surgical site infection requiring debridement and washout of the left pelvic and abdominal flank. Additionally, the patient was managed for an infection at the surgical site and underwent debridement and washout of the left pelvic and abdominal flank by long-term antibiotic therapy to address MSSA bacteremia as a source of pelvic abscess.
In December 2021, 4 months after the surgery, an MRI of the pelvis noted a soft tissue process measuring 1.8 cm × 1.6 cm along the medial margin of the resection site, adjacent to the superolateral osteotomy of the right sacral ala, concerning for recurrent disease (Figure 1 labeled as UPS-B relapse). A biopsy was performed in December 2021 and demonstrated recurrent UPS. Restaging imaging in January 2022 noted an interval increase in the size of the tumor, now measuring 2.4 cm × 2 cm. From January 2022 to February 2022, the patient was treated with a high dose of ifosfamide of 12.5 g/m^2^ in divided doses over 5 days, consistent with osteosarcoma-like treatment. After his second cycle, an imaging evaluation with MRI showed a stable tumor size, leading the patient’s course of treatment to be continued. However, the patient’s imaging after the fourth cycle demonstrated an increase in size of 3.4 cm (previously 2.7 cm). This course of therapy was discontinued due to progressive disease in April 2022, and it was recommended the patient undergo preoperative RT followed by surgery.
Based on the patient’s favorable molecular biology (high TMB, PD-L1 of 90%, and mutations in SMARCA4 and POLE genes), previous progression through systemic chemotherapy, based on SARC028 data demonstrating activity of pembrolizumab for UPS-S, and previous experience demonstrating activity of nivolumab and ipilimumab in conjunction with RT for UPS-S, he was recommended to proceed with RT with concurrent pembrolizumab therapy for three cycles between April and May 2022. The patient tolerated this course of treatment well without any toxicities.
In June 2022, the patient underwent his final surgical resection. Final pathology noted hyalinized fibrotic and necrotic tissue, consistent with extensively treated sarcoma, 2.5 cm, >99% tumor necrosis, and no definitive viable tumor identified, consistent with complete response to treatment (Figure 2B). The patient continued adjuvant pembrolizumab to complete 1 year of therapy. During that time in January of 2023, the patient did develop a mild rash on the left upper back, which was treated with topical steroid cream (Grade 1). In May of 2023, the patient started post-operative pembrolizumab. The patient remains on pembrolizumab treatment without evidence of disease as of the last follow-up in May 2024.
Discussion
The exceptional response of this patient poses a question in the approach of the typical treatment of UPS-B: should we begin to consider UPS-B as an immune-sensitive type of tumor like UPS-S?
There is a possibility that this great pathologic response may be due to the combination of ICI and RT, as a previous study examining the use of neoadjuvant ICI and RT therapy in patients with UPS and DDLPS has shown a much higher median pathologic response in UPS-S (89%) compared to DDLPS patients (22.5%) with improved disease-free survival (12, 13). Recently, the SARC032 confirmed the synergy of RT and ICI in patients with localized UPS-S, showing a clear benefit in disease-free survival (14). However, despite good responses noted in patients with UPS-S, some patients with UPS-S are resistant to ICI, and reliable biomarkers of response are lacking. In this case, the patient received RT with concurrent pembrolizumab therapy due to the histologic type (UPS) and after failure of other osteosarcoma-like SOC chemotherapies.
Specifically, the tumor harbored oncogenic mutations in SMARCA4, POLE, and STK11, which have been associated with response to ICIs (15). Additionally, this tumor had a high number of mutations on the limited NGS targeted panel, suggesting a high TMB, which has been associated with response to ICI across cancer types (16). Yet, biomarkers of response to ICIs are not well defined in sarcomas, and there is a general uncertainty in patient selection since there are no clear indicators of who will respond well to ICI, leading to limited treatment efficacy.
Although osteosarcomas exhibit an inflamed tumor microenvironment, they paradoxically respond poorly to ICI, suggesting differential immune sensitivity among bone sarcoma subtypes and emphasizing the need for further research to understand these disparities (17). Biomarkers will be crucial to target and overcome low immunogenicity and therapeutic resistance in sarcomas (18). In sarcomas, recent research suggests that the presence of tertiary lymphoid structures (TLS) in a tumor is associated with better response to ICI treatment (19, 20). In a phase 2 trial examining pembrolizumab combined with low-dose cyclophosphamide for advanced sarcomas (PEMBROSARC trial), the trial’s primary endpoint of a 6-month non-progression rate (NPR) was achieved after specifically selecting patients with TLS (40% NPR) with an overall improved objective response rate (30% from 2.4%) and a median progression-free survival of 4.1 months (20). These findings may relate to the current case by suggesting that UPS-B tumors with TLS or a highly inflamed phenotype could demonstrate improved ICI responsiveness.
Limitations of this study include its single-patient nature and the lack of direct TLS or immune infiltration assessment. Future studies should include immune profiling and multi-omic analyses of UPS-B to identify predictive biomarkers of ICI response. Additionally, prospective studies evaluating the RT and ICI combination in UPS-B are warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gusho CA Lee L Guntin J Blank AT . Comparison of features and outcomes of undifferentiated pleomorphic sarcoma of bone and soft tissue. J Surg Res. (2022) 270:313–20. doi: 10.1016/j.jss.2021.09.032, PMID: 34731728 · doi ↗ · pubmed ↗
- 2Malik AT Baek J Alexander JH Voskuil RT Khan SN Scharschmidt TJ . Malignant fibrous histiocytoma of bone: A survival analysis from the National Cancer Database. J Surg Oncol. (2020) 121:1097–103. doi: 10.1002/jso.25878, PMID: 32133661 · doi ↗ · pubmed ↗
- 3Liu B Wei H Ren YJ Zou D Zhang K Ma Q . Clinicopathological characteristics and survival of Malignant fibrous histiocytoma of the bone: A population-based study using the SEER database. Plo S One. (2020) 15:e 0232466. doi: 10.1371/journal.pone.0232466, PMID: 32492019 PMC 7269251 · doi ↗ · pubmed ↗
- 4Bramwell VH Steward WP Nooij M Whelan J Craft AW Grimer RJ . Neoadjuvant chemotherapy with doxorubicin and cisplatin in Malignant fibrous histiocytoma of bone: A European Osteosarcoma Intergroup study. J Clin Oncol. (1999) 17:3260–9. doi: 10.1200/JCO.1999.17.10.3260, PMID: 10506628 · doi ↗ · pubmed ↗
- 5Veitch ZW Fasih S Griffin AM Al-Ezzi EM Gupta AA Ferguson PC . Clinical outcomes of non-osteogenic, non-Ewing soft-tissue sarcoma of bone—-experience of the Toronto Sarcoma Program. Cancer Med. (2020) 9:9282–92. doi: 10.1002/cam 4.3531, PMID: 33063945 PMC 7774718 · doi ↗ · pubmed ↗
- 6Whelan JS Davis LE . Osteosarcoma, chondrosarcoma, and chordoma. J Clin Oncol. (2017) 36:188–93. doi: 10.1200/JCO.2017.75.1743, PMID: 29220289 · doi ↗ · pubmed ↗
- 7Korman AJ Garrett-Thomson SC Lonberg N . The foundations of immune checkpoint blockade and the ipilimumab approval decennial. Nat Rev Drug Discov. (2022) 21:509–28. doi: 10.1038/s 41573-021-00345-8, PMID: 34937915 · doi ↗ · pubmed ↗
- 8Le Cesne A Marec-Berard P Blay JY Gaspar N Bertucci F Penel N . Programmed cell death 1 (PD-1) targeting in patients with advanced osteosarcomas: results from the PEMBROSARC study. Eur J Cancer. (2019) 119:151–7. doi: 10.1016/j.ejca.2019.07.018, PMID: 31442817 · doi ↗ · pubmed ↗