Point-of-Care Ultrasound Diagnosis of Emphysematous Cholecystitis
Helena L Kons, Ariana Gorman, Maxwell Thompson, Katherine Griesmer, Samuel L Burleson, David C Pigott, John P Gullett, Luke R Bishop

TL;DR
This paper shows how point-of-care ultrasound can quickly diagnose emphysematous cholecystitis, a serious gallbladder infection, in emergency settings.
Contribution
The paper demonstrates the utility of POCUS as a rapid diagnostic tool for emphysematous cholecystitis in the emergency department.
Findings
POCUS can detect intramural or intraluminal gallbladder gas in EC patients.
Using POCUS can reduce diagnostic delays and expedite treatment in the ED.
Early diagnosis with POCUS may lower the risk of gallbladder perforation and mortality.
Abstract
Emphysematous cholecystitis (EC) is a form of cholecystitis characterized by the presence of intramural or intraluminal gallbladder gas secondary to infection by gas-forming bacteriaand is considered a surgical emergency. Computed tomography (CT) is considered the gold standard for the diagnosis of EC, but it can result in increased time to diagnosis and may not be readily available in the emergency department (ED). This delay in diagnosis may contribute to increased rates of gallbladder perforation and associated mortality. As emergency medicine door-to-first-provider times continue to increase, point-of-care ultrasonography (POCUS) can facilitate the diagnosis of this serious condition and expedite definitive care. We present a patient with EC diagnosed using POCUS and highlight the utility of POCUS in the evaluation and management of patients with this rare but serious condition.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1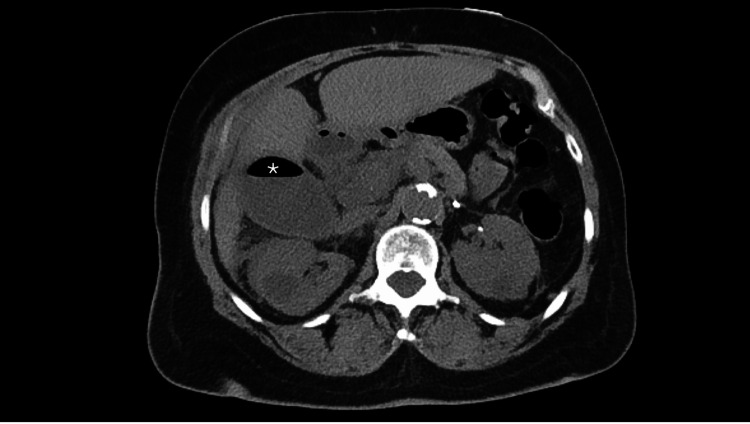 Figure 2
Figure 2 Figure 3
Figure 3| Patient lab value | Reference range | |
| WBC | 7.00 x 103/cmm | 4.00-11.00 |
| Hgb | 9.2 gm/dL | 11.3-15.2 |
| AST | 16 units/L | 12-39 |
| ALT | 11 units/L | 7-52 |
| Total Bili | 0.8 mg/dL | 0.3-1.4 |
| Alk Phos | 69 units/L | 37-117 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Abdominal vascular conditions and treatments · Biliary and Gastrointestinal Fistulas
Introduction
Abdominal pain is one of the most common chief complaints for patients presenting to the emergency department (ED) [1]. While acute cholecystitis is a relatively common cause of right upper quadrant (RUQ) pain in the ED, other sources of gallbladder (GB) pathology, such as gangrenous cholecystitis, GB perforation, and emphysematous cholecystitis, represent less common etiologies but may be associated with much higher morbidity and mortality [2]. The timely evaluation of patients in the ED with RUQ pain for whom acute GB pathology is suspected is imperative. While contrasted computed tomography (CT) offers a higher sensitivity with regard to GB pathology, prolonged turnaround times for CT results in the ED setting may lead to significant delays in the timely diagnosis and management of this patient population. Thus, the use of point-of-care ultrasonography (POCUS) can aid in the early detection of disease and should be utilized in patients for whom acute GB pathology is suspected.
Case presentation
A 69-year-old female with an extensive past medical history, including chronic obstructive pulmonary disease, coronary artery disease, chronic kidney disease, and diabetes, presented to the ED with a two-day history of RUQ abdominal pain accompanied by anorexia and altered mental status. On arrival to the ED, she was mildly tachycardic to a heart rate of 124, with a temperature of 98.4°F, a respiratory rate of 20 breaths per minute, a blood pressure of 110/70 mmHg, and an oxygen saturation of 90% on room air. The patient’s physical exam was notable for significant RUQ tenderness to palpation in addition to a positive Murphy’s sign. Laboratory evaluation revealed a white blood cell count of 7.0 x 10^9^ per liter, alanine transaminase level of 11 units per liter, aspartate aminotransferase level of 21 units per liter, and total bilirubin level of 0.5 milligrams per deciliter (Table 1).
POCUS of the RUQ revealed a distended GB with numerous shadowing stones and air in the fundus (Figure 1). Subsequent CT of the abdomen and pelvis was performed due to the admitting surgeon’s request. This was performed without intravenous contrast due to the patient’s significant chronic kidney disease and glomerular filtration rate of 12 milliliters per minute. CT revealed pericholecystic inflammatory stranding with air in the GB fundus and cystic duct (Figure 2), consistent with acute EC. A comprehensive abdominal US was obtained later in the patient's hospital stay, which revealed findings similar to the POCUS study: gallstones and sludge with pericholecystic fluid and positive sonographic Murphy sign without GB wall thickening. In addition, intraluminal gas was noted that obscured the GB fundus and was consistent with EC.
Right upper quadrant point-of-care ultrasonography showing shadowing gallstones (arrowhead) and prominent gas shadowing () originating from within the nondependent fundus and obscuring most of the gallbladder and posterior wall.*
Noncontrasted computed tomography of the abdomen and pelvis demonstrating a large, distended gallbladder with surrounding inflammatory changes and a large collection of gas in within GB ().*
Right upper quadrant ultrasound image from radiologic ultrasound that was also ordered, showing gallstones and air shadowing from the GB wall, read via radiology as emphysematous cholecystitis.
The patient was initiated on broad-spectrum intravenous antibiotics, and gastrointestinal surgery was consulted in the ED. However, the patient was deemed a poor surgical candidate secondary to multiple medical comorbidities, including congestive heart failure, coronary artery disease, chronic kidney disease, and diabetes. Given these conditions, she ultimately underwent cholecystostomy tube placement, and cultures obtained from the GB during this procedure were positive for Clostridium perfringens. She completed a five-day course of intravenous piperacillin/tazobactam with subsequent discharge on hospital day seven with the cholecystostomy tube in place for a total of six weeks.
Discussion
EC is a form of acute cholecystitis in which gas-forming bacteria such as Clostridium or Escherichia coli species infect the GB wall [3,4]. Risk factors associated with EC include male sex, diabetes, age >50 years, previous abdominal surgery, peripheral vascular disease, and immunosuppression. Clinical suspicion in patients with one or more of these risk factors should raise suspicion for EC in the ED [5,6].
EC often presents similarly to uncomplicated acute cholecystitis with right upper quadrant pain, nausea, vomiting, and lab abnormalities, including elevated serum bilirubin levels and leukocytosis [2]. However, laboratory evaluation in these patients may vary, and the mortality risk of EC remains markedly higher than that of acute cholecystitis due to the elevated risk for perforation and gangrene [7]. Thus, prompt diagnosis and treatment in patients with EC is critical. Plain radiographs, POCUS, abdominopelvic CT with contrast, and magnetic resonance imaging (MRI) have all been used to aid in the diagnosis of EC. Due to its high sensitivity in the detection of EC and GB perforation, CT remains the gold standard imaging modality for the diagnosis of acute EC [8]. Despite its higher sensitivity for the detection of EC, the abdominopelvic CT scan is associated with a longer time to diagnosis than bedside POCUS. A recent retrospective analysis from an urban tertiary care center found a median time to CT completion of 108 minutes [9]. This delay in diagnosis associated with CT imaging may contribute to the increased mortality associated with this disease. Despite its lower sensitivity in the diagnosis of acute EC, the use of POCUS has a specificity of 95% in the detection of EC and may aid in earlier detection and treatment of patients with EC and consequently decrease their risk of perforation and mortality [10].
Sonographic imaging results in acute EC vary; certain findings on POCUS offer diagnostic clues in the detection of EC. For example, large volumes of gas in or around the gallbladder can appear as a ring-down artifact, in which echogenic foci from gas bubbles result in a grayish or “dirty” appearance of posterior acoustic shadowing [11,12]. The presence of multiple gas bubbles appears as migrating echogenic foci known as the “effervescent gallbladder” or “champagne sign” [10]. Notably, as is the case with the patient presented above, any detection of intraluminal gas or gas within the gallbladder is also concerning for acute EC. The presence of these imaging findings on POCUS should prompt an expedited CT scan for diagnostic confirmation and immediate surgical consultation. Given its proven use to expedite care in potentially critically ill patients, POCUS remains a valuable diagnostic tool in the early detection of EC in the ED setting. While POCUS does not eliminate the need for an abdominopelvic CT scan in the diagnosis of EC, its ability to aid in the early detection of EC can lead to decreased rates of perforation and improved mortality.
Conclusions
CT remains the gold standard diagnostic modality for the detection of EC in the ED. However, CT scanning in the ED is associated with increased wait times and may contribute to the increased rates of perforation and higher mortality associated with this disease. Therefore, it is imperative that emergency medicine providers recognize and implement the utility of bedside ultrasonography in making this diagnosis and expediting care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Initial assessment in emergency departments by chief complaint and respiratory rate J Gen Fam Med Soeno S Hara K Fujimori R 2022082220213422179410.1002/jgf 2.423PMC 8245737 · doi ↗ · pubmed ↗
- 2Emphysematous cholecystitis: a deadly twist to a common disease J Diagn Med Sonogr Safwan M Penny SM 131137322016
- 3Emphysematous cholecystitis Radiology Esguerra-Gómez G Arango O 369373801963
- 4Emphysematous cholecystitis. Overview, etiology and pathophysiology, presentation Medscape 9 2023 Eric M Sieloff M 2023 https://emedicine.medscape.com/article/173885-overview
- 5Emphysematous cholecystitis in a young patient with no risk factors Pan Afr Med J Manatakis D Tsoukalos G 2692820172988151110.11604/pamj.2017.28.269.13923 PMC 5989254 · doi ↗ · pubmed ↗
- 6Gangrenous cholecystitis: mortality and risk factors Int Surg Önder A Kapan M Ülger BV Oğuz A Türkoğlu A UslukayaÖ 25426010020152569242710.9738/INTSURG-D-13-00222.1PMC 4337439 · doi ↗ · pubmed ↗
- 7Emphysematous cholecystitis: imaging findings in nine patients Indian J Radiol Imaging Sunnapwar A Raut AA Nagar AM Katre R 1421462120112179959810.4103/0971-3026.82300 PMC 3137852 · doi ↗ · pubmed ↗
- 8Emphysematous cholecystitis: a deadly disguise of a common culprit Clin Case Rep Mechineni A Manickam R Singh B 09202110.1002/ccr 3.4341 PMC 822264934194808 · doi ↗ · pubmed ↗